
Abstract
Objective:
To collate world reports of adverse events (AEs) resulting from lasers used in urology.
Methods:
The Manufacturer and User Facility Device Experience (MAUDE) database of the United States Food and Drug Administration (FDA) was searched using the term “Laser for gastro-urology use.” In addition, the Rockwell Laser Industries (RLI) Laser Accident Database was searched for the following types of lasers: neodymium-doped yttrium aluminum garnet (Nd:YAG), holmium:yttrium aluminum garnet (Ho:YAG), potassium titanyl phosphate (KTP), diode and thulium:YAG (Tm:YAG).
Results:
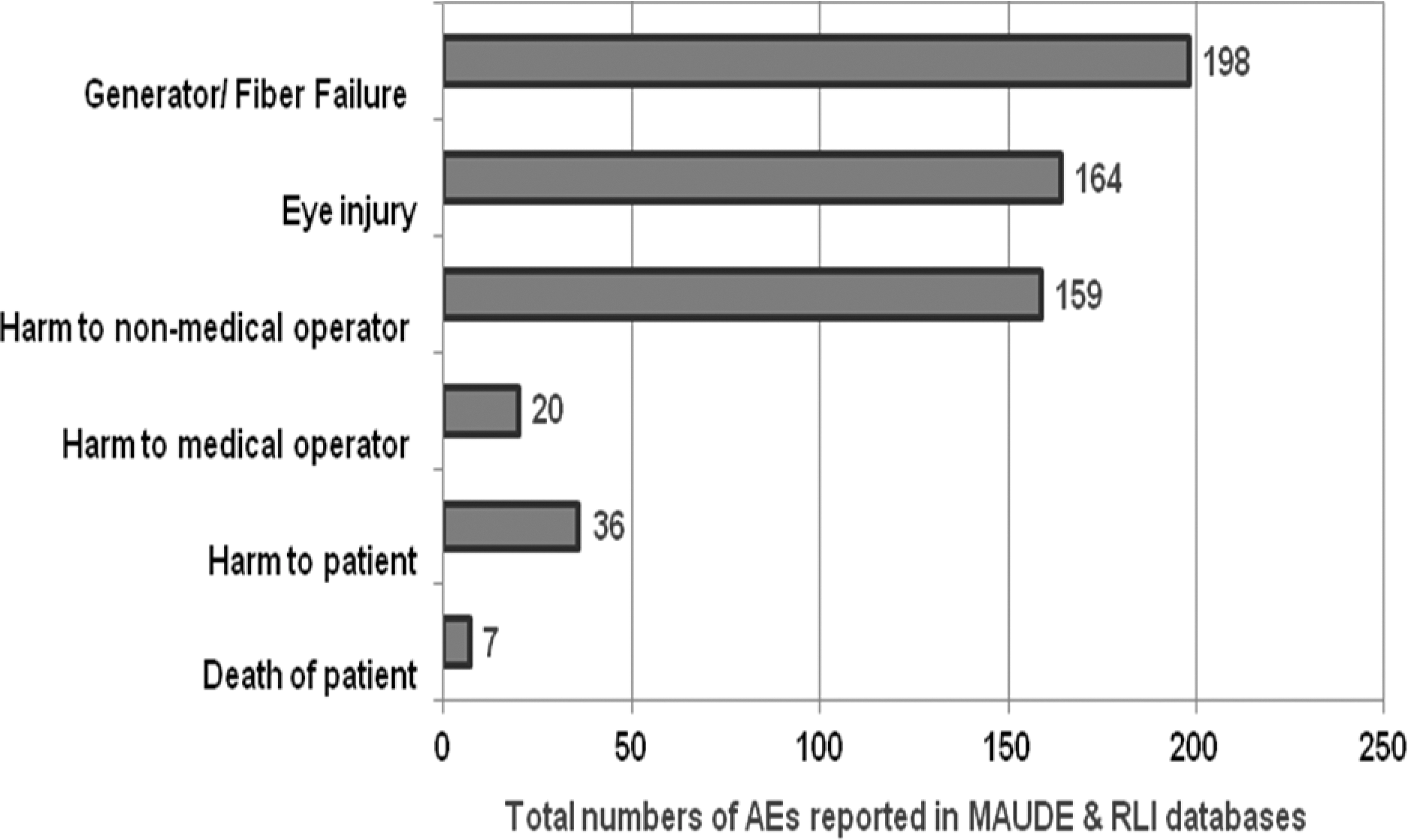
Both databases were last accessed on October 1, 2012. Overall, there were 433 AEs; 166 in MAUDE database (1992–2012) and 267 in RLI database (1964–2005). Most of the AEs (198/433 or 46%) resulted from generator failure or fiber tip breaking. Whereas there were 20 (4.6%) AEs harming medical operators, there were 159 (37%) AEs harming nonmedical operators using Nd:YAG, KTP, and diode lasers. Eye injuries ranging from mild corneal abrasions to total vision loss were reported in 164 AEs with the use of Nd:YAG, KTP, and diode lasers. Overall, there were 36 (8.3%) AEs resulting in patient harm, including 7 (1.6%) mortalities, 3 deaths from ureteral perforation using the Ho:YAG laser, and 4 deaths from air emboli using the Nd:YAG laser. Other reported patient injuries included bladder perforation resulting in urinary diversion in a patient, in addition to minor skin burns, internal burns, and bleeding in others. There were no AEs reported with the use of Tm:YAG laser.
Conclusions:
Most of the AEs reported relate to equipment failure. There were no eye injuries reported with the use of Ho:YAG lasers. Caution must be exercised when using lasers in urology, including wearing appropriate eye protection when using Nd:YAG, KTP, and diode lasers.
Introduction
L
Despite their versatility, lasers are associated with occupational hazards to operators and patients resulting from either beam-related adverse events (AEs) resulting from direct effects of laser exposure to skin and eyes, or nonbeam-related AEs resulting from exposure to laser-generated air contaminants, electrical shock, noise, or even fires. 6,7 Therefore, the safety of lasers used in endourologic procedures similar to other technological advancements needs to be monitored to improve the safety of patients and healthcare workers. 8
Healthcare safety was initially defined as “freedom from accidental injury” 9 and was later expanded to mean a well-designed process of care that could prevent, recognize, and quickly recover from errors so that patients are not harmed. 10 In a landmark study in 1999, the Institute of Medicine reported that up to 98,000 hospital deaths per year occur due to medical errors. 8 The committee determined that patient safety was the key for addressing the overall quality of a given healthcare system. Since then, awareness and research on patient safety has blossomed especially regarding organizational culture of safety. 11 One of the four recommendations of that report was mandatory and voluntary reporting system for AEs, while protecting the confidentiality of the reporters. 10 Two such reporting systems for AEs resulting from the use of lasers were already in place. The first is the Manufacturer and User Facility Device Experience (MAUDE) database developed by the United States Food and Drug Administration (FDA). The second database is maintained by the Rockwell Laser Industries (RLI). Currently, there are no data available regarding AEs resulting from the use of these lasers to patients and operators. Therefore, the aim of the present study was to collate world reports of such AEs resulting from lasers used in urology.
Methods
The MAUDE database (
MAUDE database was searched using the term “Laser for gastro-urology use,” while RLI laser accident database was searched for the following types of lasers: Nd:YAG, Ho:YAG, KTP, diode, and Tm:YAG. Data collected for each AE included the year, location, type of laser, description of the AE with its severity, use of personal protection equipments, cause of the AE, eye damage, beam diameter, and output when available. Nonurological AEs from the RLI database were excluded. Both databases were last accessed on October 1st, 2012.
Results
Overall, a total of 433 AEs were reported in both databases for the four types of lasers (Nd:YAG, Ho:YAG, KTP, and diode), including 166 (38.3%) in the FDA-MAUDE database from 1992 to 2012 and 267 (61.7%) in the RLI database from 1964 to 2005 (Table 1). There were no AEs reported with Tm:YAG laser or other types of diode laser in either database. Whereas all reported AEs in the MAUDE database came from the USA, a minority (59 or 22.1%) of AEs reported in the RLI database came from outside the USA, including 41 AEs from Asia (China, Japan, and Russia) and 17 AEs from Europe (France, Germany, and United Kingdom).
FDA=Food and Drug Administration; MAUDE=Manufacturer and User Facility Device Experience; RLI=Rockwell Laser Industries; Nd:YAG=neodymium-doped yttrium aluminum garnet; Ho:YAG=holmium:yttrium aluminum garnet; KTP=potassium titanyl phosphate; AEs=adverse events.
Of all the AEs reported, 209 (48.3%) were due to Nd:YAG laser, 140 (32.3%) were due to Ho:YAG laser, 45 (10.4%) were due to KTP laser, and 39 (9%) were the result of using the Indigo 830 nm diode laser. Urological procedures associated with AEs were reported in 133 of the 166 AEs reported in the FDA-MAUDE database. Out of 102 AEs reported in the FDA-MAUDE database with the use of Nd:YAG and Ho:YAG lasers, 40 prostate surgery (26 with Ho:YAG and 14 with Nd:YAG lasers) and 62 were associated with laser lithotripsy for ureteral or bladder stones (41 with Ho:YAG and 21 with Nd:YAG laser). The procedure was not identified in 33 AEs relating to the Nd:YAG and Ho:YAG lasers. All of the 25 AEs reported with KTP and 6 AEs reported with Indigo 830 nm diode laser in the FDA-MAUDE database were reported during transurethral prostate surgery for benign prostate hyperplasia (BPH).
Most AEs, 198 (46%), were the result of generator failure or fiber tip breakage, especially with smaller laser fibers (Fig. 1). However, there were 164 eye injuries associated with the use of Nd:YAG, KTP, and diode lasers with improper eye protection. These eye injuries were serious leading to varying degrees of harm from mild corneal abrasions to total vision loss (Table 1). There were no eye injuries reported with the use of Ho:YAG laser. There were 36 (8.3%) AEs resulting in patient harm, including 7 (1.6%) mortalities: 4 from air emboli using the Nd:YAG laser (from 1987 to 1990) and 3 from ureteral perforation and retroperitoneal bleeding using the Ho:YAG laser (between 2003 and 2005). Two other patients with air emboli from the Nd:YAG laser survived.
Laser adverse events (AEs) reported in the Manufacturer and User Facility Device Experience (MAUDE) and the Rockwell Laser Industries (RLI) databases.
The two databases also contain the following major complications during endourologic procedures necessitating open surgery for management. There were two cases with the use of Nd:YAG laser. In the first patient, ureteral perforation in addition to a broken laser fiber tip in the retroperitoneum during ureteroscopy was reported. Although not necessarily related to the Nd:YAG laser use, another patient suffered ureteral avulsion during ureteroscopy necessitating intestinal replacement. Similarly, there were two cases requiring open conversion while using the Ho:YAG laser. The first patient had bladder perforation requiring multiple corrective surgeries ultimately resulting in urinary diversion. In the second patient, the nitinol basket wires broke off while incising the ureteral orifice resulting in open conversion for basket retrieval. For the KTP laser, four patients were reported to have bladder perforations requiring open repair during photoselective vaporization of the prostate. In addition to these major complications, there were also minor complications reported such as minor skin burns, internal burns, and mucosal bleeding.
Comment
Preventing death and injury from medical errors requires dramatic changes in the organizational culture of healthcare system. This was the main message of the Institute of Medicine's report “To Err is Human” recommending implementation of voluntary reporting systems for AEs to improve patient safety. 8,10 Since lasers are routinely used in endourologic procedures, AEs associated with their use was collated using both the FDA-based MAUDE and RLI voluntary databases to assess their safety. Fortunately, only 36 AEs (9%) resulted in patient injury with the majority of AEs (198 or 46%) resulting from generator failure or laser fiber failure, especially with the smaller fibers. Laser energy is delivered through the core of a low hydroxyl silica fiber surrounded by two or three outer concentric layers, which confine laser radiation and provide mechanical stability. 12 Failure to confine energy emission to the tip of the laser can result in damage to equipment and injury to patients and operating room personnel. 13 Taking into consideration the significant variability of the commercially available laser fibers, thermal breakdown is much lower with the nontapered larger diameter laser fibers compared with the tapered 200-μm core fibers used with Ho:YAG lasers. 14 Furthermore, another study found that for Ho:YAG laser, sub-300-μm fibers were associated with significantly higher connector end failures with the laser generator compared with 365-μm fibers (4% vs. 0%; p<0.001). 15 In addition, it has been shown that when Ho:YAG lasers are activated with a deflected fiber in a tight bending radius, it may produce fiber failure and consequent irradiation of the ureteroscope resulting in instrument damage and possibly patient injury. 13 Therefore, it is not surprising that most reported AEs were related to the laser generator itself or fibers used to carry the laser energy.
To further understand the AEs associated with each of the lasers used in urology, it is important to list their wavelengths, depths of penetration, and approximate dates of introduction into clinical practice. The Nd:YAG laser was the first laser introduced to urology in 1976 with a wavelength of 1064 nm. It is absorbed by oxyhemoglobin and penetrates tissues to a depth of 5–6 mm with an unpredictable zone of coagulation. 1,4 The KTP laser is derived from the Nd:YAG laser by adding the KTP crystal, which shortens its wavelength to 532 nm. Similar to the Nd:YAG laser, the KTP laser is absorbed by oxyhemoglobin. However, it penetrates 0.8 mm with a more precise coagulation zone of 1–2 mm when compared with Nd:YAG. 16 Its use in urology was first reported in 1992. 17 On the contrary, the Ho:YAG laser, with a wavelength of 2100 nm, is absorbed by water and has a shallow depth of penetration of 0.5–1 mm. 4 The Ho:YAG laser was first reported for urologic procedures in canines in 1992 and then first reported in clinical practice in the treatment of superficial bladder tumors in 1994. 18,19 Because of its shallow depth of penetration and water absorption, the Ho:YAG laser is the current gold standard of energy source for intracorporeal lithotripsy and it has been extensively used for prostate ablative surgery. 20 There are several diode lasers manufactured by different companies with different wavelengths. These diode lasers came into market and experimental urology in the early 1990s, where the Indigo 830 nm diode laser has been used for BPH since 1995. The first reports on the use of the diode laser with a wavelength of 810 nm and depth of penetration of 8–9 mm was published in 1995, where photocoagulation of the prostate tissues was performed before radical prostatectomy. 21,22
The Tm:YAG laser, the latest commercial laser on the market, has a wavelength of 1910 nm, a zone of prostate coagulation of 0.5–2.0 mm, and was first reported in 2005. 23 The physical characteristics of these lasers explain the fact that there were significantly more AEs (209) reported with the Nd:YAG laser when compared with AEs reported with the use of Ho:YAG, KTP, and diode lasers, with 140, 45, and 6 AEs, respectively. Furthermore, the reported AEs associated with each of the lasers followed their chronological introduction into clinical practice. For example, AEs associated with the Nd:YAG laser increased since 1975 to a peak in 1995 and then declined to none, as the Nd:YAG laser was abandoned when other safer laser energy sources became commercially available (Fig. 2). On the other hand, AEs associated with Ho:YAG, KTP, and diode lasers are on the rise and it is expected that, as these lasers gain popularity worldwide, AEs associated with their use to rise as well. 7 Furthermore, there are no reported AEs related to the Tm:YAG laser since it was introduced only in 2005 and it has not been widely distributed.
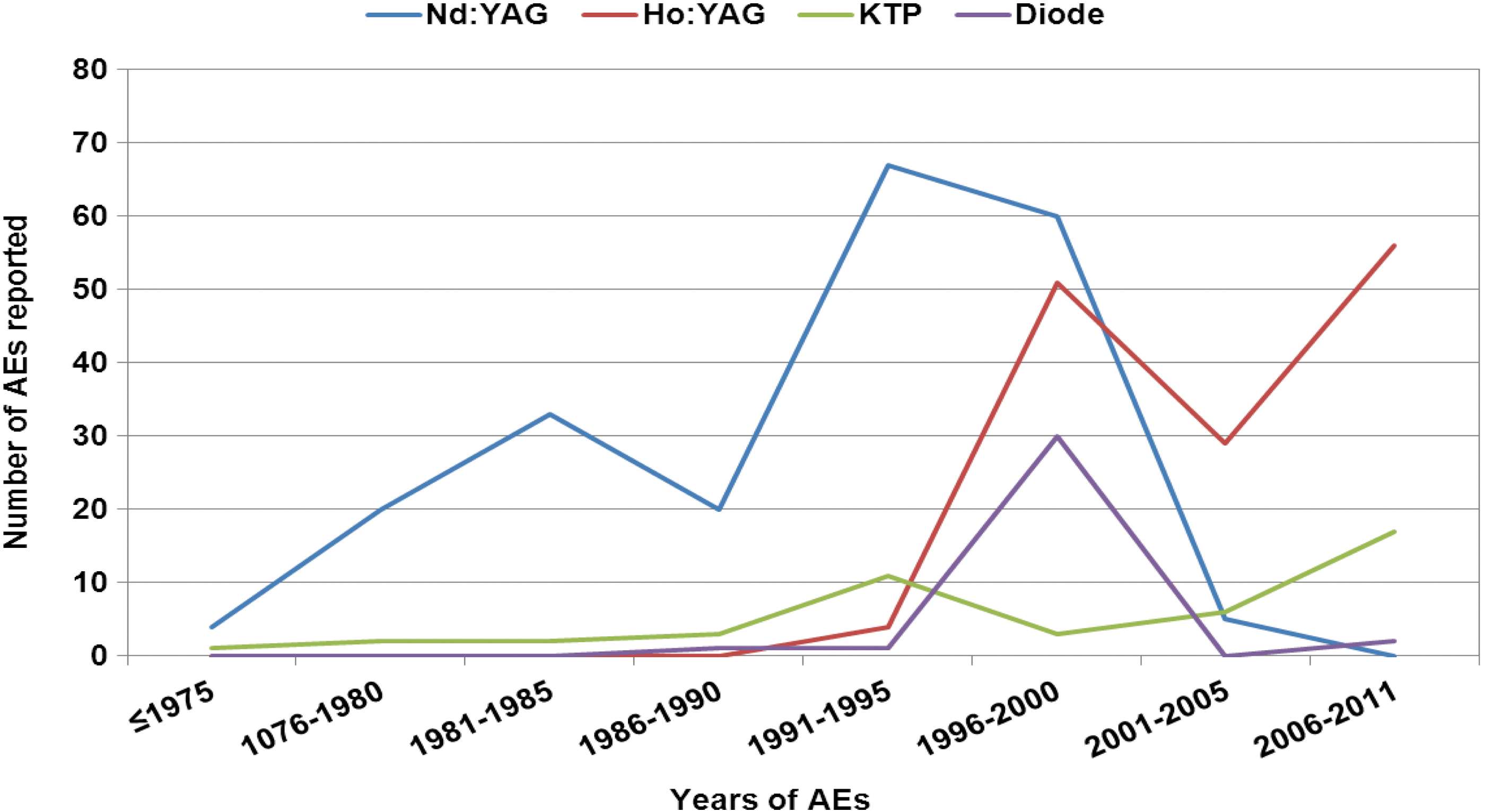
Incidence of adverse events (AEs) stratified by laser type.
Another major complication related to the nature of the Nd:YAG laser is air embolism. Unfortunately, there were six cases with air emboli resulting in four mortalities from 1987 to 1990. These events are thought to result from laser tip contact with tissues as cooling gas is forced into exposed bleeding vessels eroded by the tumor. 24 The other three mortalities resulted from retroperitoneal bleeding while using the Ho:YAG laser between 2003 and 2005. Although these AEs were reported with the use of these lasers during endourological procedures, it is possible that some of these AEs such as ureteral perforation and avulsion are related to the procedure or the surgeon's skill rather than the lasers used during the procedures.
As far as medical operators of lasers are concerned, there were 11 AEs with the use of Ho:YAG laser. These injuries were mostly minor skin burns relating to firing with a broken fiber. However, the more concerning AEs relating to medical operators are the five AEs from the use of the KTP laser leading to one case of eye injury (Table 1). Overall, there were a total of 18 eye injuries associated with the KTP laser, 33 with the diode laser, and 113 with the Nd:YAG laser. These were associated with improper eye protection. Interestingly, there were no reported eye injuries with the use of the Ho:YAG Laser. Again, this could be explained by the fact that Nd:YAG, KTP, and diode lasers are absorbed by oxyhemoglobin, whereas the Ho:YAG laser is absorbed by water. Therefore, when improper eye protection is used with the use of Nd:YAG, KTP, and diode lasers, a stray laser light could penetrate the eye and burn the retina. 7
Hence, appropriate eye protection must be worn when Nd:YAG, KTP, and diode lasers are in operation. This is consistent with what has been recommended by the Institute of Medicine to build a culture of safety, which starts by training operating room personnel to be compliant with safety precautions, including wearing appropriate eye protection. 8 Furthermore, the hospital needs to make sure that comfortable wavelength-specific goggles are available for operating room personnel and patients during these procedures. In addition, according to the WHO 2009 surgical safety checklist, laser equipment and fiber inspection need to be part of the preoperative checklist. 25 Routine inspection of laser generators by the biomedical engineers and having well-trained operating room personnel dedicated to the use of lasers are important for the safety of patients and operating room personnel. According to the Occupational Safety and Health Administration, 500,000 healthcare workers use lasers and are exposed to electrosurgical smoke yearly. 26 Therefore, AEs relating to the use of laser may happen. Once these AEs occur, they need to the reported to the institutional laser safety officer and the FDA-MAUDE database so that safety of these lasers could be monitored, thus satisfying the recommendations of the Institute of Medicine. 8
How representative is this data regarding the true incidence of AEs resulting from lasers used in urology remains unclear as the true incidence of these AEs might be higher than what is already reported. Therefore, the main limitation of the current study is the voluntary reporting of AEs in both databases. It is likely that many more events were not reported or could have been filed under different terms than those used in this study, especially for diode laser since different wavelengths are produced under the same category of diode laser. Moreover, it is not clear whether some cases have been reported in both databases. Unfortunately, there are no other databases collecting laser AEs. Previous studies on laser accidents also used both of these databases to report laser accidents in general. 27 Furthermore, PubMed search of the topic only revealed scattered case reports. 28 In addition, the denominator in terms of the number of cases performed during the same time period is unknown and is impossible to document. However, when MAUDE database was used to collate AEs related to robotic platforms used in urology, the incidence of AEs reported in that database correlated to those found in clinical audits. 29,30 Therefore, these AEs reported in both databases are reliable especially for serious outcomes such as mortalities from air emboli and loss of vision injuries. Notwithstanding its limitations, this is the first such study documenting AEs related to the use of lasers in urology.
Conclusions
Most of the AEs reported relate to equipment failure. There were no eye injuries reported with the use of Ho:YAG lasers. Caution must be exercised when using lasers in urology, including wearing appropriate eye protection when using Nd:YAG, KTP, and diode lasers.
Footnotes
Acknowledgments
This work was supported, in part, by the Canadian Urological Association Scholarship Foundation and the Montreal General Hospital Foundation Awards to Sero Andonian.
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.