
Abstract

I read with keen interest the article by Fischer and associates. The authors need to be congratulated for an interesting and a novel method to remove a proximally migrated stent in a remote hospital setting where access to a ureteroscope is not available. They have presented a single case experience of this technique. I want to voice my reservations about this technique.
The experience of proximally migrated stents has shown that the alignment of the stent's lumen in relation to the distal ureter is dependent on the location of the stent's distal end and not to the make and strength of the coil of the stent. If the stent has migrated only to the intramural part of the ureter, then the stent remains parallel to the ureteral lumen (Fig. 1). Once the stent migrates to the mobile extravesical portion of the lower ureter, it tends to kink and hook the ureter toward its coil (Fig. 2). We do not agree with the author's hypothesis that stent alignment to the ureter depends on the degree of the dilation of the distal ureter and the coil strength of the stent. The coil strength of the stent should, rather, be sufficient because poor coil strength could increase the risk of stent migration. 1
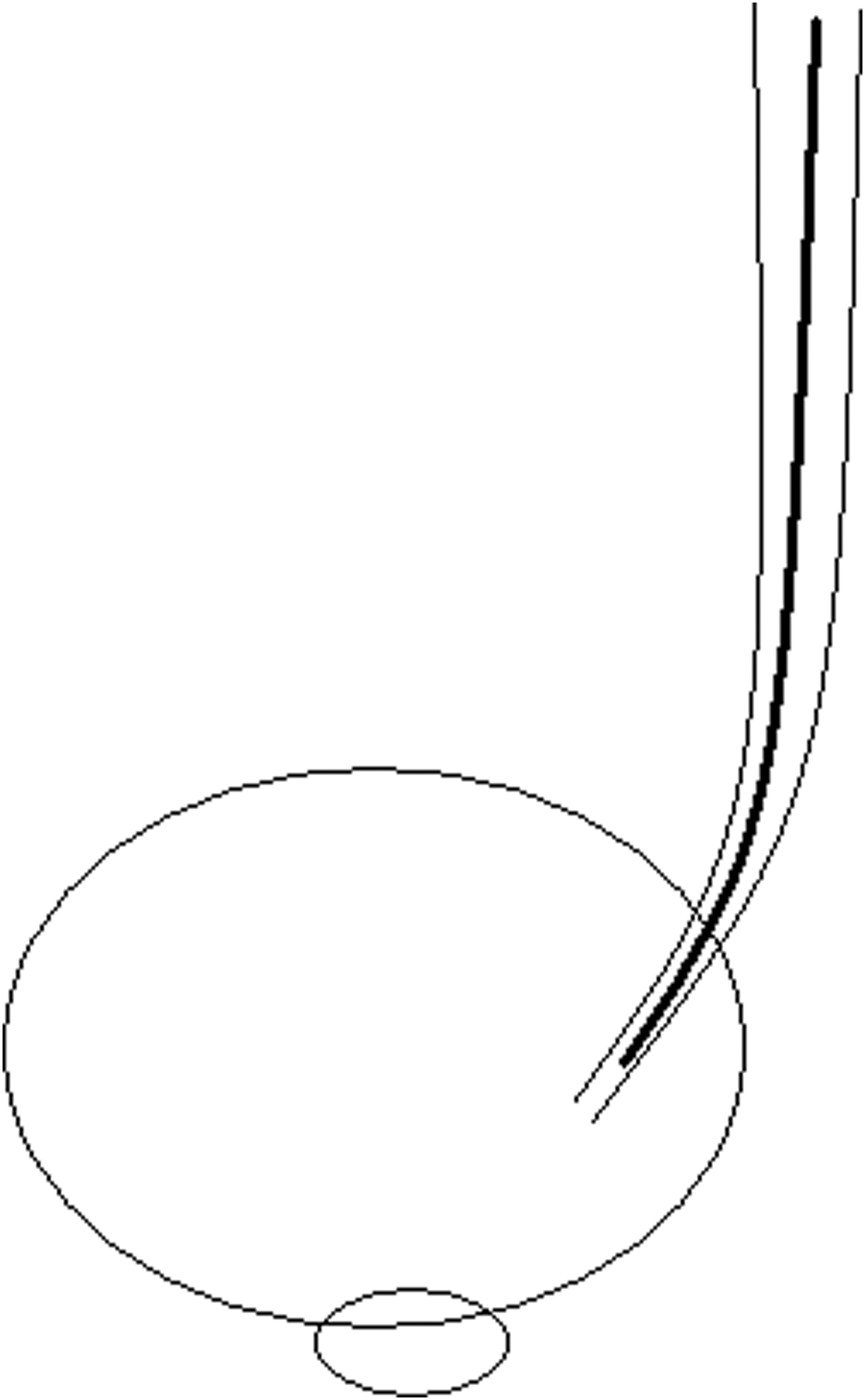
The stent is seen parallel to the ureter when the distal end is in the intramural segment of the ureter.
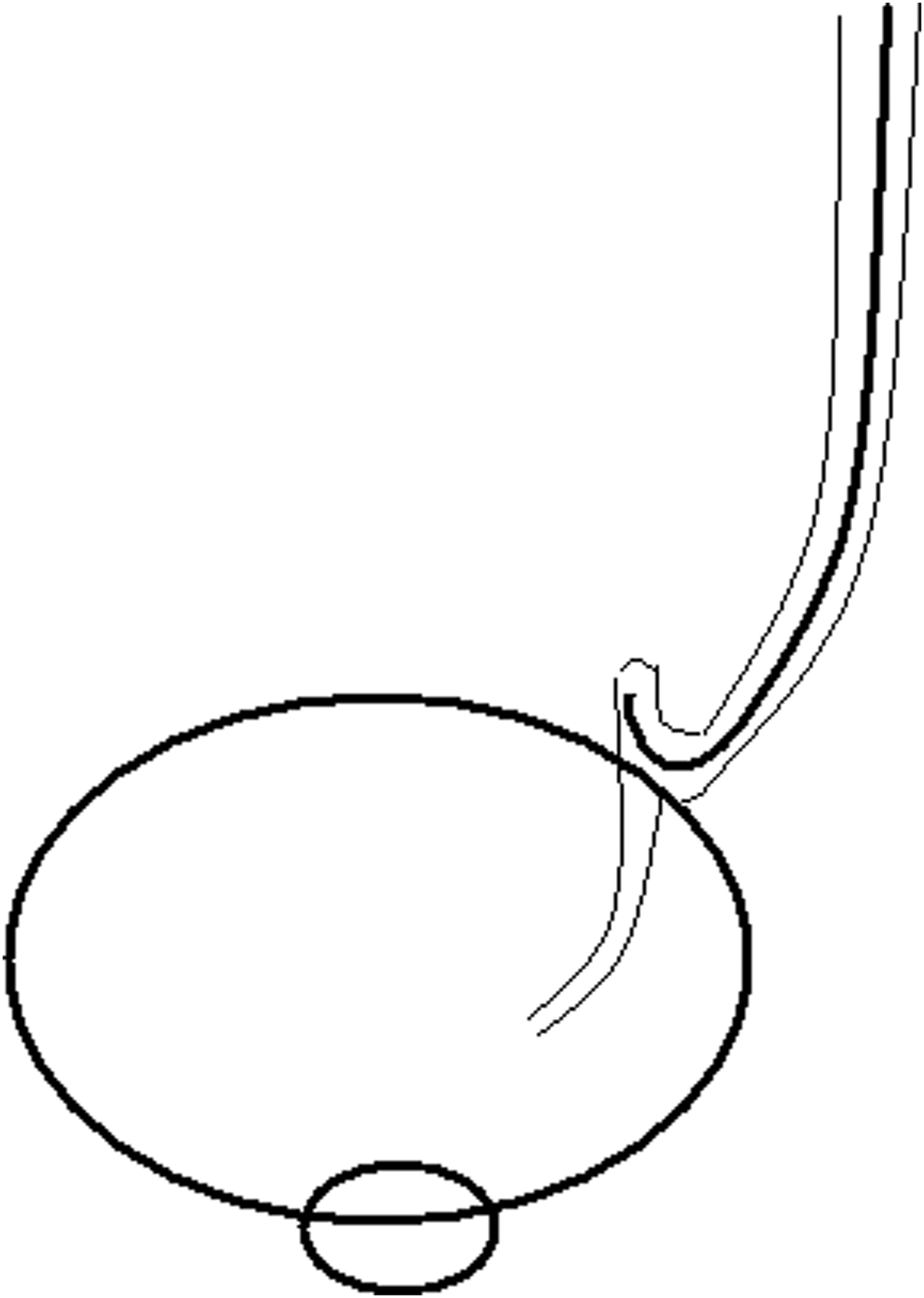
The ureter gets kinked in the direction of the coil when the stent migrates in the extravesical portion of the ureter.
Placing a wire through the stent's lumen would further be difficult in most cases because most of the stents (>64%) get blocked in situ. 2 The stents may get blocked as soon as within a week of placement.
Coaxial cannulation of a migrated stent's lumen by paired wire helical basket has been described in the literature, but that was performed under ureteroscopic vision. 3 Cystoscopic cannulation of a migrated stent under fluoroscopy guidance would be very difficult.
In this case, it is indeed the patient's and the surgeon's luck that the guidewire entered the stent's lumen and then got reflected back down the ureter to the bladder. This would be very difficult to replicate regularly; hence, to propose this technique as a method for removal of a proximally migrated stent is not justified.
If a stent migrates in a remote surgical setting, the patient should be referred to a center where ureteroscopy facilities are available.