
Abstract
Objective:
This study evaluated the outcomes of laparoscopic donor nephrectomy (LDN) and proposed modifications for kidney donation surgery. From February 1997 to February 2011, 1510 LDNs were performed.
Patients and Methods:
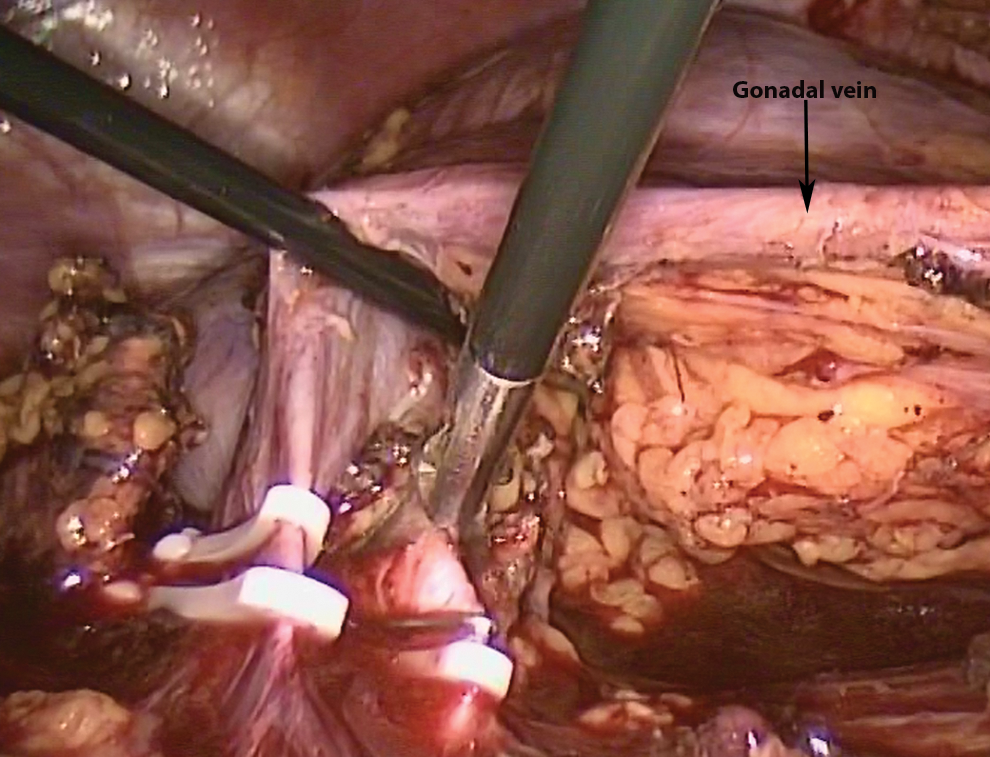
Surgical modifications included a modified open access technique for entry into the abdominal cavity, using vascular clips for safe and cost-effective control of the renal pedicle, control of the lumbar veins, and adrenal vein using bipolar cautery instead of clips, and leaving the gonadal vein intact with the ureter. Kidneys were extracted by hand through a Pfannenstiel incision. Heparin was not used after the first 300 cases to prevent potential hemorrhagic complications.
Results:
Although three major vascular injuries occurred using the closed access method that were managed successfully, no access-related complications occurred using the modified open access technique. Clip failure did not happen in any cases. Patient and graft survival at 1 year post-transplantation were 96.5% and 95.5%, respectively, and at 5 years post-transplantation were 95.3% and 89.5%, respectively.
Conclusion:
The proposed surgical modifications are based on 14 years of experience and 1510 cases, and make LDN simple, safe, and cost-effective. The excellent recipient and graft outcomes with minimal morbidity obtained further confirm that LDN can be considered as the gold standard for kidney donation surgery.
Introduction
R
The advantages of laparoscopic donor nephrectomy (LDN) include shorter hospital stays and recovery times, and enhanced cosmesis. 3,4 LDN is gaining popularity and has become the gold standard for donor nephrectomy in many major transplantation centers globally. However, some concerns remain about the safety and morbidity of LDN for donors, and graft survival in recipients. A previous report described a randomized controlled study involving 200 transplantations that compared LDN with open donor nephrectomy (ODN) and demonstrated lower morbidity and similar graft outcomes in the LDN group. 4
In this article, we report on a retrospective study that reviewed 1510 kidney donor/recipient pairs, where the donor underwent LDN. Further, some practical modifications to the surgical technique that might enhance the safety, simplicity, and cost-effectiveness of LDN are presented. To our knowledge, this is the largest series of LDN patients reported from a single center.
Patients and Methods
From February 1997 to February 2011, 1510 LDNs were performed. Evaluation of the kidney donors included their medical history, a physical examination, renal function tests, and renal computerized tomography angiography to visualize the renal vasculature.
When each kidney was similar in appearance, the left kidney was preferentially removed. If the left kidney had more than a single artery and the right kidney had a single main renal artery, the right kidney was chosen for donation, but only if the renal artery branched inside the renal hilum.
A senior urolaparoscopic fellow and an experienced senior urologist performed the LDNs, and the same urologist who performed the LDN, transplanted the kidney into the recipient. Patients were administered general anesthesia during the surgery that was performed in the modified flank position with the patient fully padded and taped securely to the table.
The peritoneum was accessed through an open access technique, wherein a semicircular 12 mm incision was made in the supraumbilical area, the rectus fascia was dissected under direct vision, the peritoneal layer was opened by blunt dissection, and a 12 mm trocar without a blade was inserted for the videoscope. Two 5 mm trocars were inserted in the subxiphoid and suprapubic positions under direct vision, and a single 10 mm trocar was secured in the pararectal position. The peritoneal cavity was insufflated with carbon dioxide at a pressure of 15 cm H2O during trocar insertion, and the pressure was reduced to 12 cm H2O during the operation.
After laparoscopic exploration of the abdominal cavity, the descending or ascending colon was taken down and retracted medially to expose the renal pedicle. The renal vein and artery were dissected in close proximity to their roots—the vein was dissected close to the inferior vena cava and the artery was dissected close to the aorta to obtain sufficient length for anastomosis. The ureter was dissected to the point where it traversed the iliac vessels. The vascular supply of the ureter was retained, while preserving the gonadal vein and periureteral tissues.
The left kidney was freed from the surrounding tissues using the extra-Gerotal approach (similar to that used in radical nephrectomy surgery) to minimize the iatrogenic trauma to the renal parenchyma and its vasculature, except at the upper pole where the kidney was separated from the adrenal gland. The lumbar veins and adrenal vein were cauterized by bipolar cautery, instead of using clips, and then divided. The pressure of the veins is not high, so these veins were coagulated sufficiently with bipolar energy. After division of coagulated vein, the edges of divided vein recoagulated to assure nice occlusion. Occasionally, lumbar veins are big and clips are preferred, but when we coagulate these big veins using bipolar cautery, the diameter of lumbar vein shrinks immediately and we can coagulate the cut edges following division in good length and enough time.
We administered heparin (3000 units [U]) to the first 300 cases during the operation before renal artery ligation, and this was neutralized by protamine sulfate administration on completion of the surgery. However, two cases of unexplained bleeding from the suture line and three cases of unexplained hematoma formation at the nephrectomy site led to a modification of our policy and heparin injections were discontinued.
Before 2005, medium/large titanium clips were used for the safe control of the main renal vessels. Subsequently, to double ligate the renal artery, we applied a 10-mm Hem-o-lok® (Weck Surgical Instruments; Teleflex Medical, Durham, NC) clip immediately adjacent to the aorta (a few millimeters distal to the insertion) and applied a medium/large titanium clip distally to the Hem-o-lok clip using a nonautomatic firing clip applier (Karl Storz, Endovision, Inc., Charlton, MA). The surgeon controlled the titanium clip's closing pressure (Fig. 1). Once satisfied that the renal artery was safely controlled, double ligation of the renal vein was performed using two 12-mm Hem-o-lok clips (Fig. 2).

We applied a 10-mm Hem-o-lok® (Weck Surgical Instruments; Teleflex Medical, Durham, NC) clip immediately adjacent to the aorta (a few millimeters distal to the insertion) and applied a medium/large titanium clip distally to the Hem-o-lok clip using a nonautomatic firing clip applier for double ligation of renal artery.
Once satisfied that the renal artery was safely controlled, double ligation of the renal vein was performed using two 12-mm Hem-o-lok clips.
The right renal vein and artery were ligated using two clips, similar to the ligation on the contralateral side. For donor safety, we did not remove the right renal vein with a patch from the inferior vena cava; however, consequently, the right renal vein was very short. Although the length of the right renal vein was quite short for anastomosis, inverting the donated kidney in the right iliac fossa of the recipient, as per Hamburger's recommendation, 5 appears to resolve this problem by making a safe and simple venous anastomosis possible. 6
The specimen was extracted through a Pfannenstiel incision by hand to minimize the warm ischemia time (WIT), ensure better cosmesis, and lower surgical costs. The kidney was immediately immersed in ice slush and perfused with an intracellular electrolyte preservation solution.
Operating time was defined from the time of trocar insertion to the time of incision closure. WIT was defined as the time taken to clip the renal artery and immerse the kidney in ice slush, and delayed graft function (DGF) was defined as the need for dialysis within 1 week of transplantation.
Results
This study involved 1510 kidney donors with a mean age of 28.0±5.2 years and 1510 kidney recipients with a mean age of 36.6±15.7 years. Right-side donor nephrectomy was performed in 116 cases and the remaining cases underwent left-side donor nephrectomy. Patients were followed for a mean period of 950.5±720 days (range, 90–3670 days). Males comprised 64% of the recipients and 81% of the donors. More than 95% of the donors were not related to the recipient. Of the 74 donors who were related, the most common relationships with recipients were mothers (n=19) and brothers (n=19).
The mean operating time for kidney donation was 241 minutes (range, 70–345 minutes) and the mean duration of hospitalization was 4.3±1.15 days (range, 2–15 days). Analysis of these variables over the five preceding years showed that the mean operating time and the mean duration of hospitalization had decreased by 170 minutes (range, 70–210 minutes) and 4.09±1.35 days (range, 2–11 days), respectively.
The mean pre- and postoperative serum hemoglobin levels were 15.31 and 14.14 mg/dL, respectively (p=0.585). Three patients required blood transfusions during the operation and nine cases required blood transfusions in the postoperative period.
There were no major perioperative complications evident in 99.6% of donors, with no injuries to the main renal artery or dislodgment of clips at the stump of the pedicle. Among the donors, 93.9% had uneventful postoperative periods. Clavien grading of the perioperative and postoperative complications is presented in Table 1.
LDN=Laparoscopic donor nephrectomy.
Nine donors (0.6%) underwent open conversion because of hemorrhage from a divided accessory splenic artery (one case), uncontrolled cardiac arrhythmia that was successfully managed (one case), main renal vein injury (one case), bleeding from the aorta (two cases), iliac vein injury (one case), and main renal arterial anomalies (three cases, two of which had undergone right-sided nephrectomy). Major vascular injuries, including aortic and iliac vein injuries that were managed successfully by immediate conversion, occurred when the closed technique was used for peritoneal access (the first 470 cases). Following these cases, we changed the technique to the modified open access technique, and since then, no cases of major vascular injury have occurred. The mean WIT and cold ischemia time were 6.5±2.4 and 42.36±15.6 minutes, respectively.
Approximately 79.5% of the recipients had undergone previous sessions of dialysis and 8.1% of the recipients were undergoing their second or third kidney transplantation.
Arterial anastomosis involved the internal iliac artery in 59.7% and the common iliac artery in 32% of the recipients. The donor vein was anastomosed to the external iliac vein in 98.2% of the patients. Of the recipients, 93.2% underwent kidney transplantation on the right side, whereas 92.3% of the donated kidneys were from the left side.
Patient and graft survival were 96.5% and 95.5%, respectively, at 1 year post-transplantation and 95.3% and 89.5%, respectively, at 5 years post-transplantation (Tables 2 and 3).
SE = standard error.
SE = standard error.
A comparison of patient and graft survival among recipients with and without DGF demonstrated better outcomes in patients without DGF (p=0.0001). WIT did not have a significant impact on patient survival (p=0.92). Similarly, no statistically significant association was apparent between WIT and graft survival (p=0.13) (Fig. 3).
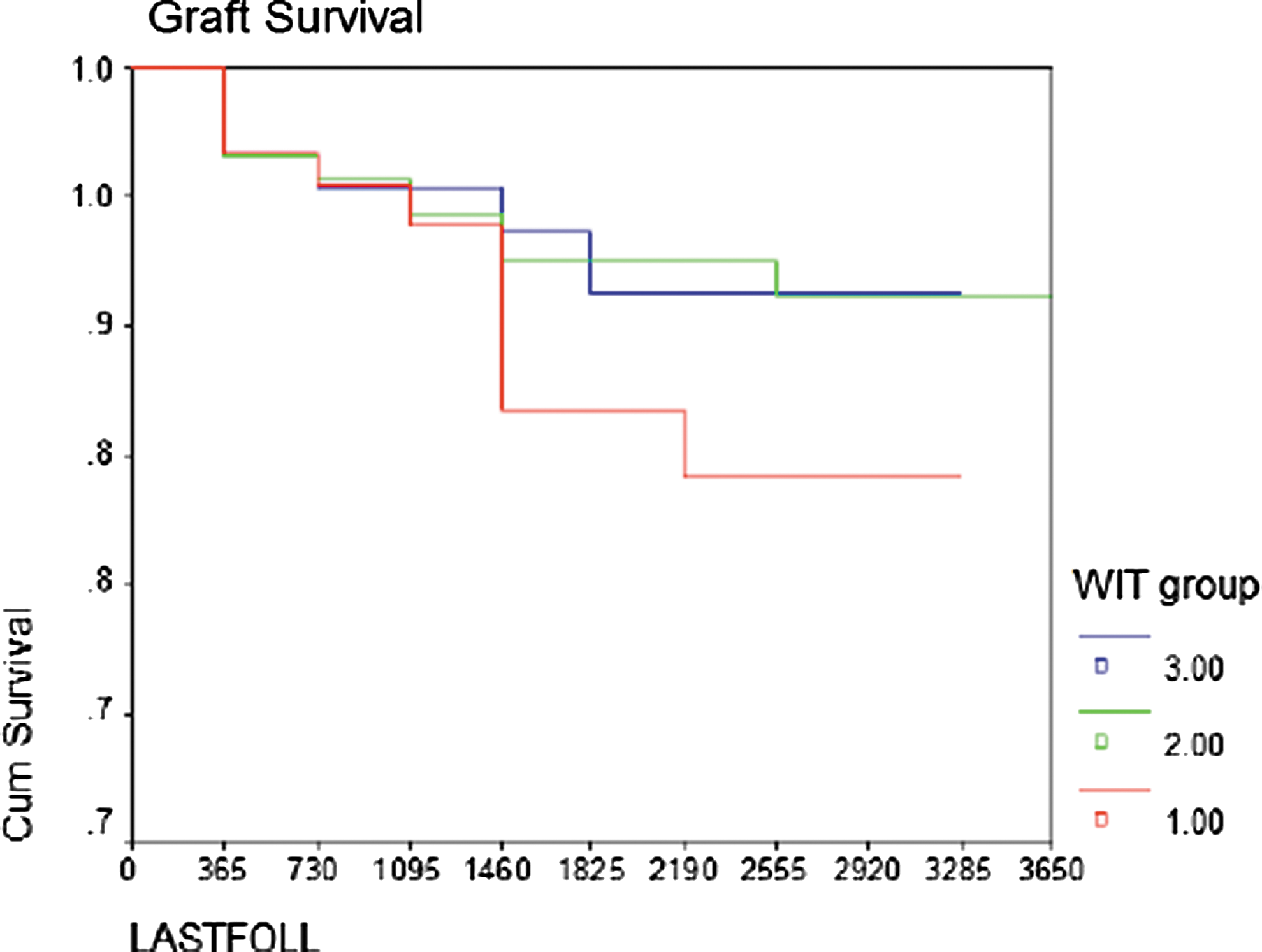
No statistically significant association was apparent between warm ischemia time (WIT) and graft survival.
Renal vein thrombosis and renal arterial thrombosis were noted in 0.2% (four cases) and 0.06% (one case) of recipients, respectively, and the transplanted kidneys were removed the day after transplantation in these cases. Ureteral leaks or stenosis (0.9%) occurred in 15 cases. Most ureteral complications (86%) were observed within the first year post-transplantation and only two cases of ureteral complications were noted thereafter.
Discussion
The need for kidney transplantation has exhibited a marked increase in recent years, and it appears that living kidney donation is the immediately available remedy. The introduction of living LDN has certainly generated renewed interest in minimizing donor morbidity. 7 The popularity of the laparoscopic approach with its emphasis on reducing operative morbidity may have increased the number of renal donor volunteers. 8
In our center, neither donor age nor donor obesity were included as exclusion criteria, and our findings showed that body mass index (BMI) had no significant impact on DGF and rejection episodes. Kuo et al. 9 compared two kidney donor groups with a BMI of >31 and a BMI of <31 that had undergone LDNs and concluded that morbidity, mortality, and surgical outcomes were similar for both groups. Jacobs et al. 10 assessed different variables in 41 LDN cases and showed that the operating time was 40 minutes longer in cases with BMI of >35 than in cases with lower BMI values; however, the recipient renal outcomes were comparable between these two groups of patients.
A standard technique for LDN has previously been reported 10,11 ; however, during our 14 years of experience, we have modified the LDN to improve safety, and save time and money. Hereafter, we discuss these technical modifications in the context of the literature.
We abandoned the closed technique using the Verres needle for laparoscopic entry into the abdominal cavity after the first 470 cases due to the occurrence of major vascular injuries in 3 cases that were treated by an attending urologist familiar with vascular surgery, and due to some vascular or visceral injuries previously reported by other centers. 12,13 Thus, the modified open access technique is preferred for the first trocar insertion in our center. We made a 1 cm incision above the umbilicus, and after incising the rectus fascia, the peritoneum was opened by blunt scissors while holding up the abdominal skin. No major vascular or visceral injuries occurred while using this method.
In the most centers, the lumbar veins and the adrenal vein are ligated using clips. In this study, we do not intend to present this technique to replace using clips, but we want to present our method for managing lumbar veins and adrenal vein as an alternative method. We never encountered any problem in this regard with good number of cases.
To ensure a sufficient length of the left renal vein, it was clipped distal to the gonadal vein; thus, we routinely preserved the gonadal vein with the ureter, leaving the vascular supply of the ureter intact. The ureter was freed en-block with the surrounding tissues and the gonadal vein was cauterized using bipolar cautery at the site of the pelvic entrance and divided.
In some transplantation centers, 3000 U heparin is infused before the renal artery is ligated; however, except for the first 300 cases, we did not use heparin in the present study. Ramani et al. 14 compared 40 LDN patients who were infused with 5000 U heparin and 39 LDN patients who did not receive a heparin infusion. The results indicated that the recipients' immediate, early, and DGFs were comparable between the groups and that graft thrombosis was not detected in either group. Therefore, they stopped heparin infusions during surgery to prevent possible intra- and postoperative bleeding. Friedersdorff et al. 15 showed that the WITs and the mean duration of hospitalization were similar in 65 donors who received heparin infusions and 54 donors who did not. They noted that the need for re-exploration and postoperative bleeding was higher in the heparin-infused group. 16 Hence, based on our experience with a large number of cases and reports in the literature, it appears that heparin infusion during LDN is unnecessary.
Before July 2005, we used three medium/large titanium clips to safely control the renal vessels. 16 Subsequently, a single 10-mm Hem-o-lok clip and one medium/large titanium clip were used for renal artery control; in addition, two 12-mm Hem-o-lok clips in the right and left side were used to control the main renal vein. 17 In our experience of LDN and 1834 laparoscopic nephrectomies performed for other reasons, no complications related to the vascular clips, including clip slippage or dislodgement, have occurred. 18
An endovascular stapler is the preferred approach to control the renal pedicle vessels in some centers; however, using the vascular Endo GIA™ is expensive and certain studies have reported about stapler malfunction. Chan et al. reported 10 cases of Endo GIA malfunction among 565 cases of laparoscopic nephrectomies and 2 cases involving conversions to open in this patient series. 19 Moreover, a few reports have linked two cases of mortality to endovascular stapler malfunction; these are described in the Manufacturer and User Facility Device Experience Database. 20 In addition, endovascular stapler malfunction was also associated with the need for cardiopulmonary resuscitation in a patient. 21 In another study, the failure rate of the endovascular stapler was estimated at 3%, whereas the failure rate of Hem-o-lok clips was 1.7%. 22 Furthermore, 6 of 10 major vascular injuries in 738 cases of LDN occurred during stapler usage. 23
To lessen the trauma to the kidney, and thus, to the renal parenchyma, the kidney was freed from the surrounding tissues similar to the approach in radical nephrectomy. Many centers routinely remove the perirenal fat to facilitate the placement of the kidney in the Endo Bag.
We chose to extract the donated kidney by hand from a transverse lower abdominal or Pfannenstiel incision, which results in good cosmetic outcomes. This approach was concomitant with improved safety and considerable cost savings. Shalhav et al. recommended using manual specimen retrieval instead of an Endo Catch™ bag based on similar recipient outcomes, lower complication rates, shorter operating times, and noticeable cost savings that were obtained using the two techniques. 24 Mohamed et al. 25 and Rao et al. 26 reported grade IV renal parenchymal lacerations and transection of the renal pelvis, respectively, after using Endo Catch bags for kidney extraction.
We introduced another modification in 116 cases undergoing transplantation of a right kidney with a short renal vein (<1.5 cm) that involved inverting the kidney in the right iliac fossa to position the renal vein posteriorly and as close as possible to the external iliac vein. 6
A survey of long-term graft outcomes did not reveal any significant differences between the LDN and ODN groups in relation to 5-year patient survival (91.9% and 96.7%, respectively, p=0.48) and 5-year graft survival (84.3% and 89.5%, respectively, p=0.96) in a randomized clinical trial. 27 Other reports have confirmed that patient and graft survival were comparable in donor kidneys obtained by either laparoscopy or open surgery. 28 –30 Brook et al. reported that patient and graft survival were similar in the LDN (315 cases from 11 centers) and ODN (1159 cases) groups during a 10-year follow-up period. 28 Chaykovska et al. compared long-term outcomes of LDN and ODN in pediatric kidney recipients and found no significant differences between the two groups; however, better clinical findings were noted in the LDN group at the mean 64-month follow-up point (graft survival at 1 and 5 years was 97% and 91%, respectively, in LDN vs 94% and 88%, respectively, in ODN). 31
Two retrospective studies by Nogueira et al. 32 and Amico 33 revealed worse graft outcomes in a large number of recipients with DGF compared with those without DGF. Their findings were similar to our results.
The major complication rates during nephrectomy and in the postoperative period in the study of 738 cases of LDNs by Jacobs et al. were 6.8% (10 vascular injuries) and 17.1%, respectively, and 1.6% of their cases required open conversion. 23 In a study by Hadjianastassiou et al., the total and major complication rates in LDN were 10.3% and 4.5%, respectively, and the major complications were comparable to those associated with ODN (p=0.549); however, the overall complication rate was significantly better in the LDN group (p=0.001). 34 In our survey, the overall complication rate was 6.1%, and 0.6% of cases underwent open conversion.
Vascular complications after transplantation were noted in 0.5%–8.8% of kidney recipients in previous reports. Osman et al. 35 detected rates of 0.4% for renal artery thrombosis and 0.1% for renal vein thrombosis in 1200 recipients after transplantation. Other studies by Zilinska et al. 36 and Salehipour et al. 37 indicated rates of 3.9% and 0.6% for renal artery thrombosis, respectively, and rates of 2.9% and 0.5% for renal vein thrombosis, respectively. In the current study, renal vein and renal arterial thrombosis were noted in 0.2% and 0.06% of recipients, respectively.
We were able to make LDN more cost-effective, by saving approximately USD 1.36 million over 1510 LDN operations by modifying the surgical technique. The use of vascular clips to achieve vascular control during laparoscopic nephrectomy saved a considerable amount of money (approximately USD 670 per operation), without jeopardizing surgical outcomes. 18 Moreover, using a hand-extraction technique instead of an Endo Catch bag in LDN saved at least USD 150 per operation, 9 and the use of nondisposable trocars saved approximately USD 45 per operation.
Conclusion
This retrospective study of 1510 cases with long-term follow-up further confirms that LDN is associated with lower morbidity and is more cosmetically acceptable compared with ODN, while has similar graft outcomes compared with ODN. Moreover, some minor modifications described may enhance the safety, simplicity, and cost-effectiveness of LDN.
Footnotes
Disclosure Statement
No competing financial interests exist.