
Abstract
Aims and Objectives:
The optimal management method of lower caliceal calculi is still undefined. We performed a prospective randomized comparison to evaluate safety and efficacy of shock wave lithotripsy (SWL) and flexible ureteroscopy (RIRS) for lower caliceal calculus ≤2 cm.
Materials and Methods:
Between December 2011 and January 2012, 195 patients with single radio-opaque lower caliceal calculi ≤2 cm were included in the study. Randomization was done into two groups—group A: SWL performed as an outpatient procedure using the electromagnetic lithotripter (Dornier compact delta) and group B: RIRS was performed using the 6F/7.5F flexible ureteroscope (Richard Wolf) with holmium laser intracorporeal lithotripsy. Demographic characteristics, success, retreatment, and auxiliary procedure rates and complications were analyzed statistically.
Results:
Of 195 patients, 97 and 98 patients were enrolled in group A and B, respectively. Mean stone size was 12.1 mm in group A vs 12.3 mm in group B (p=0.52). The overall 3 month stone-free rate was (74/90) 82.2% for group A vs (78/90) 86.6% for group B (p=0.34); for stones <10 mm, it was (45/55) 84.9% for group A vs (43/51) 87.7% for group B (p=0.32) and for 10–20 mm stones, it was (29/35) 78.4% for group A vs (35/39) 85.4% for group B (p=0.12). Retreatment rate was significantly greater in group A compared with group B (61.1% vs 11.1%; p<0.001). Auxiliary procedure rate was comparable (21.1% vs 17.7%; p=0.45). The complication rate was 6.6% in group A vs 11.1% in group B (p=0.21).
Conclusions:
Both SWL and RIRS are safe and efficacious for lower caliceal calculi ≤20 mm. For stones <10 mm, SWL was less invasive and safer than RIRS with efficacy comparable to it. However, for 10–20 mm stones, RIRS was more effective, with lesser retreatment rate.
Introduction
M
Lower caliceal stones more than 2 cm are best managed by PCNL, 2 but for stones less than 2 cm SWL is the most common treatment modality used. 3 For lower caliceal stones less than 2 cm, both SWL and RIRS are available as treatment modalities. 4 SWL is minimally invasive, without anesthesia requirement, has a good patient tolerance with adequate analgesia, and can be performed with minimal complications. 5 However, SWL is affected by stone size, stone composition, anatomical factors, and patients body habitus, which may decrease the efficacy of SWL and increase the retreatment rate. 6 With improvement in endoscopic techniques and the development of flexible ureteroscopes, enthusiasm for this procedure is increasing as it gives good stone clearance with minimal complications and lower retreatment rate though it requires anesthesia. 7,8
We conducted a prospective randomized study between SWL and URS for lower caliceal stones ≤2 cm to evaluate the safety and efficacy of the procedures. To the best of our knowledge, after the best possible MEDLINE search, this is the first prospective randomized study in a single center, comparing SWL and RIRS, for inferior caliceal stones up to 2 cm.
Materials and Methods
After getting clearance from the institutional ethics committee, between September 2012 and June 2013, 234 consecutive patients attending Urology Outpatient Department with a single lower caliceal radiopaque calculus ≤2 cm (including stones ≤5 mm), were enrolled for this prospective randomized study. Exclusion criteria included patients with bleeding disorders, active urinary infection, age >60 years and <15 years, weight >100 and <40 kg, comorbid cardiovascular and respiratory illnesses, fever >38°C, total leukocyte count >12,000/dL, serum creatinine >1.5 mg/dL, solitary kidney, coexisting ureteric pathology, including tumor/stricture, pregnancy, moderate and severe hydronephrosis, unfavorable lower caliceal anatomy, radiolucent stones, caliceal diverticulum associated with the targeted stone, and pelvic kidney.
The eligible patients were randomized into two groups: group A (SWL group) and group B (RIRS group) using a computer-generated randomization table. Each group was further divided into two subgroups on the basis of stone size: subgroup A1 and B1—stone size ≤1 cm and subgroup A2 and B2—stone size 1–2 cm.
Initial evaluation included a detailed clinical history, urine analysis, and urine C&S test when indicated, complete hemogram, liver function test, kidney function test, serum calcium, serum phosphate, serum uric acid, urine routine microscopy, urine culture sensitivity, 24-hour urine analysis, including calcium, phosphate, and uric acid as a routine metabolic workup. Ultrasound and KUB X-ray (to assess the radiopacity of the calculus) and a noncontrast computed tomography with 3D reconstruction (to know the location and size of the calculus, to know the lower caliceal anatomy) was done.
In the SWL group (group A), SWL was performed as an outpatient procedure using the Dornier Compact Delta manufactured by Dornier Medizintechnik GmbH. Five grams of eutectic mixture of lignocaine and prilocaine was applied on ∼30 cm2 skin area corresponding to the entry site of the shock waves, 60 minutes before the procedure. A tablet of diclofenac sodium (dosage: 50 mg for body weight <70 kg, 100 mg for >70 kg) was given orally at the same time. The rate of shock wave delivery was 100 impulses per minute. The maximum number of shock waves to be given per session was 3000 shock waves. The patient was observed for 2 hours after each session. X-ray (KUB) and USG (KUB) were used to check stone fragmentation and clearance after each session at 2 weeks. Retreatment SWL was given for incomplete clearance and maximum of four sessions of SWL were given. RIRS and PCNL were the auxiliary procedures performed after failed SWL.
In the RIRS group (group B), the procedure was performed using a 6F/7.5F flexible ureteroscope dual channel (Cobra) manufactured by Richard Wolf. Dilation of ureteral orifice was done wherever required. Ureteral access sheath was used in all cases. The holmium laser (Lumenis versa plus 100 W) manufactured by Lumenis Ltd. was used for intracorporeal lithotripsy. The power setting of the holmium laser was 0.5–1 J. The pulse rate was set between 20 and 40 Hz. A 2.2F Nitinol stone basket was used for fragments removal. In cases of large stone burden, Double-J stent was kept in situ. Double-J stent was removed after 4 weeks. Stone analysis was done in all cases. PCNL was the auxiliary procedure performed after failed RIRS.
Study parameters in both the groups were patient demographics, stone characteristics, analgesic characteristics (supplemental analgesia, adverse effects), and treatment details. The outcome variables in both groups were the stone-free status at 3 month, retreatment rates, modified Efficiency Quotient (EQ), and auxiliary procedure rates. The stone-free status after initial SWL session or RIRS was defined as the radiological absence of stone, asymptomatic patients with stone fragment less than 3 mm and sterile urine culture at 3 months or earlier. Modified EQ was used to distinguish between patients who became stone free primarily by SWL or RIRS and those who were stone free by auxiliary procedure.
Observations were recorded and arranged on Microsoft Excel spreadsheet (Microsoft) and were analyzed by the SPSS software version 17.0. The chi-square test was used for categorical variables. Student's t-test and Wilcoxon rank sum test (group A/B, A1/A2, B1/B2) were used for continuous variables. p-Values less than 0.05 was considered significant.
Results
A total of 234 patients with single lower caliceal radiopaque calculus, ≤2 cm in size were included in the study. Of them, 39 patients were excluded as they failed to satisfy the eligible criteria. The rest of the patients (195 patients) were included in the study and were randomized into two groups using computer generated randomization table: 97 patients in group A and 98 patients in group B. Fifteen patients (seven from SWL group and eight from RIRS group) were lost to follow up. So, a total of 180 patients were analyzed in the study. The subgroups A1, A2, B1, and B2 had 55, 35, 51, and 39 patients, respectively (Fig. 1).
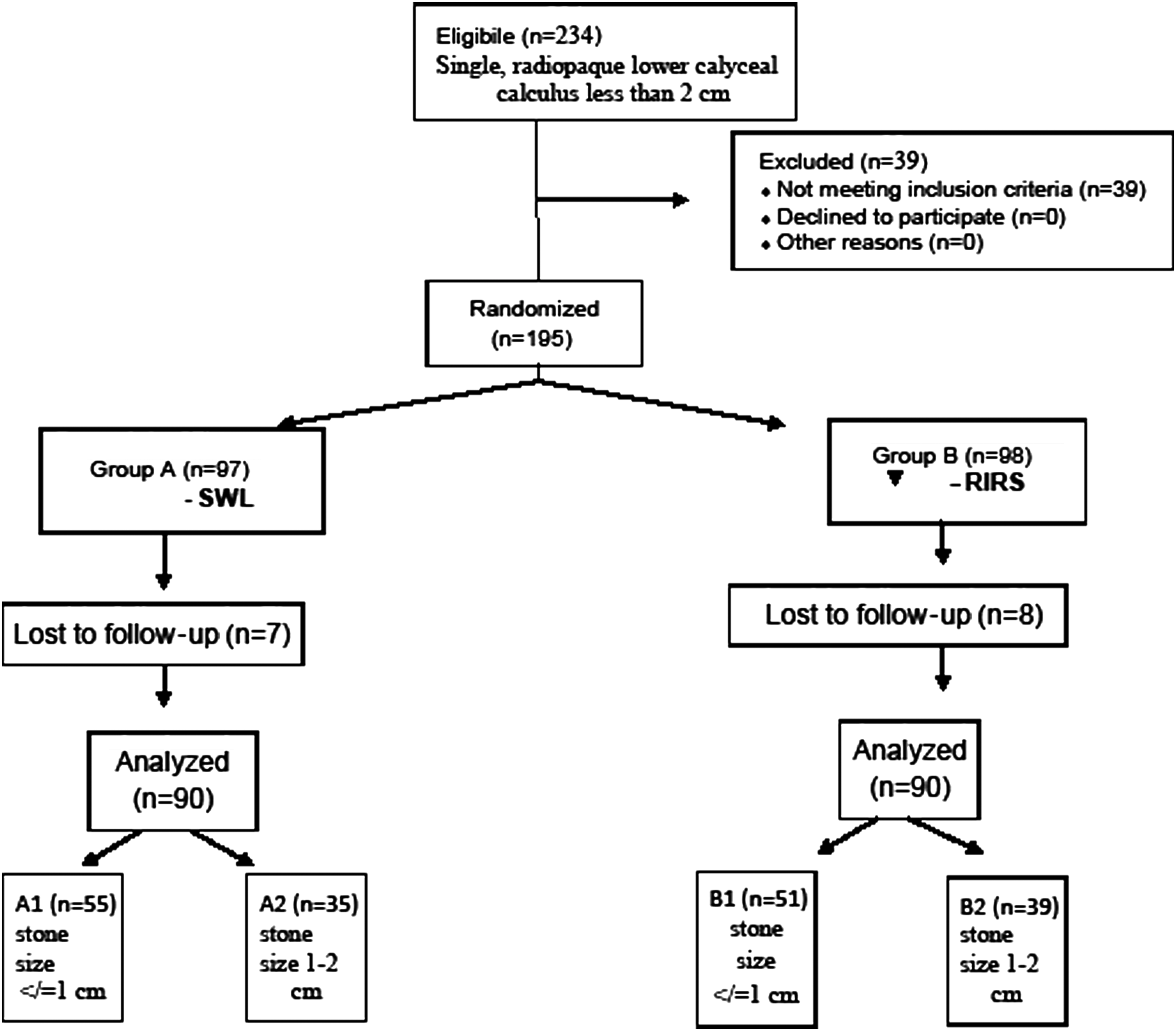
Flow diagram.
The demographic characteristics, stone locations, and size of the patients are listed in Table 1. The age, sex ratio, the height, the weight, the stone location (right/left), and size were comparable in both the groups and subgroups. The degree of hydronephrosis and lower caliceal anatomy was not significantly different between the groups and subgroups.
Numbers in parentheses indicate±standard deviation in degree.
NS=not significant.
The treatment outcomes are summarized in Table 2. The operating time between the subgroups was not significantly different. The retreatment rate was significantly higher in SWL group. The number of auxiliary procedure required was higher in group A1 as compared to B1 and B2 as compared to A2, but the difference was not statistically significant. The stone-free rate at 3 months, although comparable in each subgroup, was higher in RIRS group (A1=84.9%, A2=78.4%, B1=87.7%, B2=85.4%). Modified EQ, which includes the retreatment rate of each patient for complete stone clearance was significantly higher in group B2 as compared to A2. But the difference between the groups A1 and B1 was not statistically significant. The stone composition between the subgroups was comparable (Table 3) and it had no effect on treatment outcome.
A1 vs B1 : NS
A2 vs B2 : S
EQ=efficiency quotient; NS=not significant; S=significant.
The complication rates between the subgroups are summarized in Table 4. In group A, the most common complication was severe pain, but could be managed with oral and parenteral analgesics, but in group B it was urinary tract infection which could be managed with oral antibiotics. Out of 180 patients, only 2 patients, 1 in each group had gross hematuria, which could be managed conservatively without any blood transfusion. There were no deaths in either group. The cost effectiveness of either procedure is not calculated.
Discussion
Treatment options for lower caliceal stones are varied, but the optimal treatment approach is still to be defined. Small, asymptomatic lower caliceal stones can be managed expectantly, but more than 30% patients will have progression and some will also develop pain in the future. 1 So intervention may be needed in many patients.
SWL has been the most accepted treatment modality for lower caliceal stones. 2,9,10 It is minimally invasive and has a good patient tolerance and a low complication rate. However, its efficacy for lower caliceal stones is less than that for upper and middle calyces. 11 Its efficacy is affected by patient's weight and body habitus. Stone size affects stone clearance after SWL, and as the stone size increases the efficacy of stone clearance decreases. 12 The lower caliceal anatomy (infundibular length, width, and infundibular angle) also affect the stone clearance after SWL. 6,13
However, SWL has been the most common treatment modality used for lower caliceal stones. 2,9,10 With the improvement of RIRS technology, it becomes an attractive option for the treatment of lower caliceal stones. It has the advantage of clearing the stone in one sitting as well as avoiding morbid complications of PCNL. 14 It has an excellent stone clearance rate and is less affected by stone density, stone size upto 2 cm, and stone location. 8
Prospective randomized trials comparing the two modalities are limited. In a prospective study taking 62 patients with stone less than 1 cm, Pearle et al. concluded that there is no difference in stone-free rate and complication rates between the two modalities. 10 El-Nahas et al. compared 37 patients with lower caliceal stones 1–2 cm and found that RIRS provided higher stone-free rate and lower retreatment rate compared to SWL and the complication rates of RIRS were not significantly higher. 15
In our study, we have included stones up to 2 cm in size. We have found that for stones less than 10 mm in size, efficacy and safety of SWL and RIRS were comparable. The stone-free rate at 3 months for both the procedures was not significantly different (82.2% in SWL and 86.6% in RIRS). The result is similar with the result of previous studies by Pearle et al. and El-Nahas et al.
In our study, the retreatment rate for SWL was significantly higher than URS. But when we calculated the modified EQ (which is an indirect evidence of retreatment rate), the difference was not significant. For stones 1–2 cm in size, the efficacy of RIRS was better than SWL, which was reflected by lower retreatment rate and higher modified EQ. The stone-free rate at 3 months was higher with RIRS, but the difference was not statistically significant.
Conclusion
For treatment of lower caliceal stones ≤2 cm in size, both SWL and RIRS are safe and highly efficacious. For stones ≤10 mm: SWL was safe, less invasive, and with comparable efficacy in comparison to RIRS. For stones 10–20 mm: RIRS was more effective, with a lesser retreatment rate than SWL.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.