
Abstract
Introduction:
Complication rates of open radical prostatectomies (ORPs) and laparoscopic radical prostatectomies (LRPs) performed by highly experienced surgeons in centers of excellence are well known. Using a standardized, national, risk-adjusted surgical database, we compared 30-day outcomes following ORP and LRP and analyzed how trainee involvement influenced outcomes.
Methods:
The American College of Surgeons-National Surgical Quality Improvement Program (ACS-NSQIP) is a risk-adjusted data collection analyzing preoperative risk factors, demographics, and 30-day postoperative outcomes. From 2005 to 2011, we identified 10,669 total prostatectomies. Of these, 2278 were ORP and 8391 were LRP. Data on trainee involvement were available on 63% of cases.
Results:
Comparison of all 10,669 prostatectomies showed a decreased incidence of overall morbidity, serious morbidity, surgical site infections, mortality, wound disruption, urinary tract infection, bleeding, and sepsis or septic shock (p<0.05) for LRP compared with ORP. Trainee involvement was associated with a higher incidence of bleeding, overall and serious morbidity (p<0.001). This difference is isolated to postgraduate year (PGY) 6–10 trainees performing ORP (p<0.001). Overall and serious morbidity was equivalent between PGY groups 1–10 versus attending without trainee performing LRP and PGY groups 1–5 versus attending without trainee performing ORP. Operative times were shorter for ORP versus LRP by an average of 38 minutes (p<0.05), and in cases involving trainees, operative times decreased with trainee experience for both procedures. The length of stay was shorter for LRP compared with ORP (3.2 vs. 1.8 days, p<0.001).
Conclusions:
The large sample size, standardized data definitions, and quality control measures of the ACS-NSQIP database allow for in-depth analysis of subtle, but significant differences in outcomes between groups. Trainee involvement in LRP appears safe to patients. However, the increased morbidity in ORP involving trainees may be mitigated by awareness, simulation laboratories, and standardized competency assessment.
Introduction
P
Patients and Methods
The American College of Surgeons-National Surgical Quality Improvement Program (ACS-NSQIP) is the first nationally validated, risk-adjusted, outcome-based program to measure and improve the quality of surgical care, analyzing preoperative risk factors, demographics, and 30-day postoperative outcomes. Since its inception in 1994 within the Veterans Health Administration System, NSQIP was piloted in the private sector by the ACS in 2001 and now includes over 250 participating hospitals, including those in the Department of Defense. At participating hospitals throughout the United States, medical records are reviewed by Surgical Clinical Reviewers. Specific variables, including the patient's demographics, preoperative comorbidities, laboratory values, intraoperative variables, and postoperative outcomes, are recorded as they relate to the 30-day index operation. Operations are recorded and searchable through Current Procedural Terminology (CPT) coding. The data are standardized in this fashion, and consistency is maintained by on-site audit programs at all participating ACS-NSQIP hospitals. 14,15
Using the NSQIP Participant User Files, a retrospective review was undertaken for the years of 2005–2011. We used the CPT codes for ORP (55840, 55842, 55845), and LRP (55866) as based on the International Classifications of Disease Diagnosis Codes 9th Edition (ICD9) and identified all of the recorded cases in the ACS-NSQIP database from January 1, 2005 to December 31, 2011. Preoperative demographics and intraoperative data, to include operative times, whether a surgical trainee participated or not, and most senior surgical trainee levels were recorded. We analyzed outcomes as they related to trainee involvement versus no trainee involvement. Our analysis also included stratification of trainees based on the level of experience with postgraduate year (PGY) 1–5 representing junior and midlevel residents, and PGY 6–10 representing senior residents and fellows.
Outcomes
Primary evaluated outcomes were overall morbidity, serious morbidity, nonserious morbidity, surgical site infection (superficial SSI, deep SSI, and organ space SSI), wound disruption, and mortality. Secondary evaluated outcomes included bleeding, urinary tract infection, deep venous thrombosis, and renal failure. Serious morbidity was defined as having documentation of at least one of the following ACS-NSQIP outcomes: mortality, organ space SSI, wound disruption, neurological event (stroke or cerebrovascular accident with or without neurologic deficit, or coma lasting >24 hours), cardiac arrest, myocardial infarction, bleeding requiring transfusion during a period from the surgical start time up to and including 72 hours postoperatively, pulmonary embolism, ventilator dependence >48 hours, progressive or acute renal insufficiency, and sepsis or septic shock. Overall morbidity was defined as having documentation of a serious morbidity, mortality, or at least one of the following ACS-NSQIP outcomes: superficial SSI, deep SSI, pneumonia, peripheral neurological deficit, unplanned intubation, urinary tract infection, and deep vein thrombosis. Nonserious morbidity was defined as at least one or more individual outcomes not considered a serious morbidity. Patients could experience more than one of the listed complications. Outcomes present at the time of surgery were excluded in the postoperative outcome analysis.
Risk-adjustment factors
Multiple variables were evaluated as they pertained to 30 outcome risks. Broadly, we evaluated laparoscopic radical versus open approach, patient demographics, comorbidities, and preoperative laboratory values. Patient demographic variables included age, gender, and race/ethnicity. The patient's preoperative risk was also evaluated based on the body mass index, American Society of Anesthesiologists (ASA) class, and preoperative functional status assessed by the patient's ability to perform activities of daily living and stratified as independent, partially dependent, totally dependent, and unknown. Comorbidities included diabetes (requiring oral medications or insulin vs. none), renal disease (dialysis or acute renal failure with an increase in BUN and creatinine >3 mg/dL by 1–2 laboratory measurements as determined by preoperative documentation of renal failure by the surgeon), dyspnea, ascites, chronic obstructive pulmonary disease, current pneumonia, ventilator dependence, chronic steroid use, bleeding disorders, heart failure (within 30 days before index operation), hypertension, coronary artery disease (including angina, myocardial infarction within 6 months of the index operation, percutaneous cardiac intervention, or cardiac operation), peripheral vascular disease (including revascularization for peripheral vascular disease, claudication, rest pain, amputation, or gangrene), disseminated cancer, weight loss (>10% body weight within 6 months of index operation), current chemotherapy within 30 days or radiotherapy within 90 days, neurologic deficit (including stroke with or without neurologic deficit, transient ischemic attacks, hemiplegia, paraplegia, quadriplegia, or impaired sensorium), preoperative transfusion within 72 hours of the index operation, and preoperative systemic inflammatory syndrome/sepsis. Social risk factors of alcohol use (>2 drinks per day) and smoking status (within 1 year before the index operation) were also included.
Twelve preoperative serum laboratory values were also included (serum albumin, alkaline phosphatase, aspartate aminotransferase, bilirubin, white blood cell count, hematocrit, platelet count, prothrombin time, partial thromboplastin time, creatinine, and sodium). The stratification of laboratory values as normal or abnormal was based on ACS-NSQIP definitions.
Statistical analyses
All statistical analyses were conducted in SAS v. 9.2 (SAS Institute, Cary, NC). Fisher's exact tests (two sided) and chi-square tests were used to assess associations between the type of surgical approach and categorical variables. Two-sided t-tests were used to assess mean differences between LRP and ORP for continuous outcomes. An analysis of variance was used to compare means among the three experience level subgroups. Hospital LOS was transformed to the log scale to enhance normality for analysis. Stepwise logistic regression (LR) analyses using an inclusion criterion of p<0.05 were done to estimate odds ratios (OR) for overall morbidity and serious morbidity adjusted for significant risk factors. The LR analyses also examined interactions to evaluate whether the outcome of the surgical procedure varied with trainee involvement. Error bars in charts represent 95% confidence intervals (CIs) based on standard error of the mean for continuous variables and on the exact binomial distribution for categorical outcomes. A significance level of p<0.05 was used for all analyses unless otherwise stated.
Results
During the study period, 10,669 prostatectomies from a total of 182 participating hospitals were accrued into the ACS-NSQIP database. Of these, 2278 were ORP, and 8391 were LRP. Out of these 10,669 cases, 6737 (63.1%) contained data that indicated whether a trainee was involved in the patient's case versus an attending without a trainee involved. Trainee involvement among the two surgeries included 489 PGY 1–2 cases, 2177 PGY 3–5 cases, 1163 PGY 6–10 cases, and 2908 attending without trainee cases. ORP encompassed a total of 1580 (23.4%) cases, and LRP included a total of 5157 (76.6%) cases. Demographics were largely the same between LRP and ORP. Steroid use, recent chemotherapy, preoperative transfusion, and neurologic disorder were all slightly (though significantly) more common in ORP versus LRP (Table 1).
Statistically significant.
History of angina in the month before the index operation, history of myocardial infarction 6 months before the index operation, previous percutaneous cardiac intervention, or previous cardiac surgery.
History of revascularization/amputation for peripheral vascular disease and rest pain or gangrene.
CVA/stroke with or without neurologic deficit, history of transient ischemic attacks, hemiplegia, paraplegia, impaired sensorium, quadriplegia.
Preoperative systemic inflammatory response syndrome or sepsis.
Transfusion of packed red blood cells up to 72 hours before surgery.
ACS-NSQIP=American College of Surgeons National Surgical Quality Improvement Program; ASA=American Society of Anesthesiologists; ORP=open radical prostatectomy; LRP=laparoscopic radical prostatectomy; PGY=postgraduate year.
In evaluating all cases accrued (10,669 LRP and ORP), 880 (8.2%) experienced a major or minor morbidity and 17 (0.2%) patients died. Thirty-day overall morbidity, serious morbidity, nonserious morbidity, and SSI were all significantly higher in the ORP group versus the LRP group (Table 2). In the trainee involvement data set, overall morbidity, serious morbidity, nonserious morbidity, and SSI were all significantly higher in the ORP versus LRP group. Pneumonia and mortality were slightly higher in the attending without trainee group [p=0.048 and 0.044, respectively (Fig. 1)]. When comparing trainee involvement to attending without trainee, significantly higher rates of overall morbidity and serious morbidity were seen with trainee involvement. Furthermore, this increased morbidity isolated out to ORP involving PGY 6–10 and was primarily due to increased bleeding (30.4% vs. 4.7%, p<0.0001 [PGY 6–10 vs. attending without trainee]) (Fig. 2).
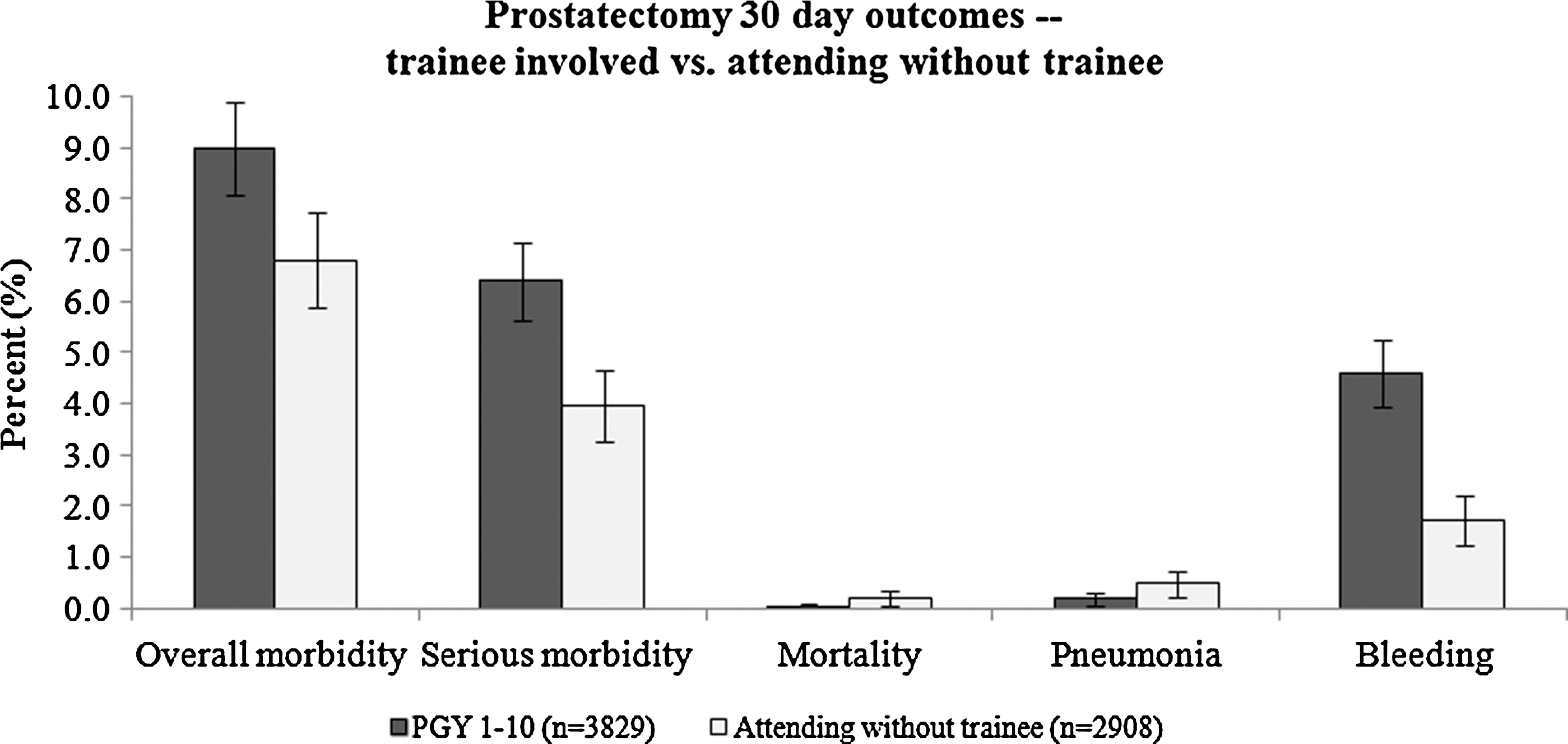
Selected outcomes of 6737 prostatectomies performed from 2005 to 2011 at the American College of Surgeons-National Surgical Quality Improvement Program (ACS-NSQIP) affiliated hospitals (p<0.05 for all comparisons).
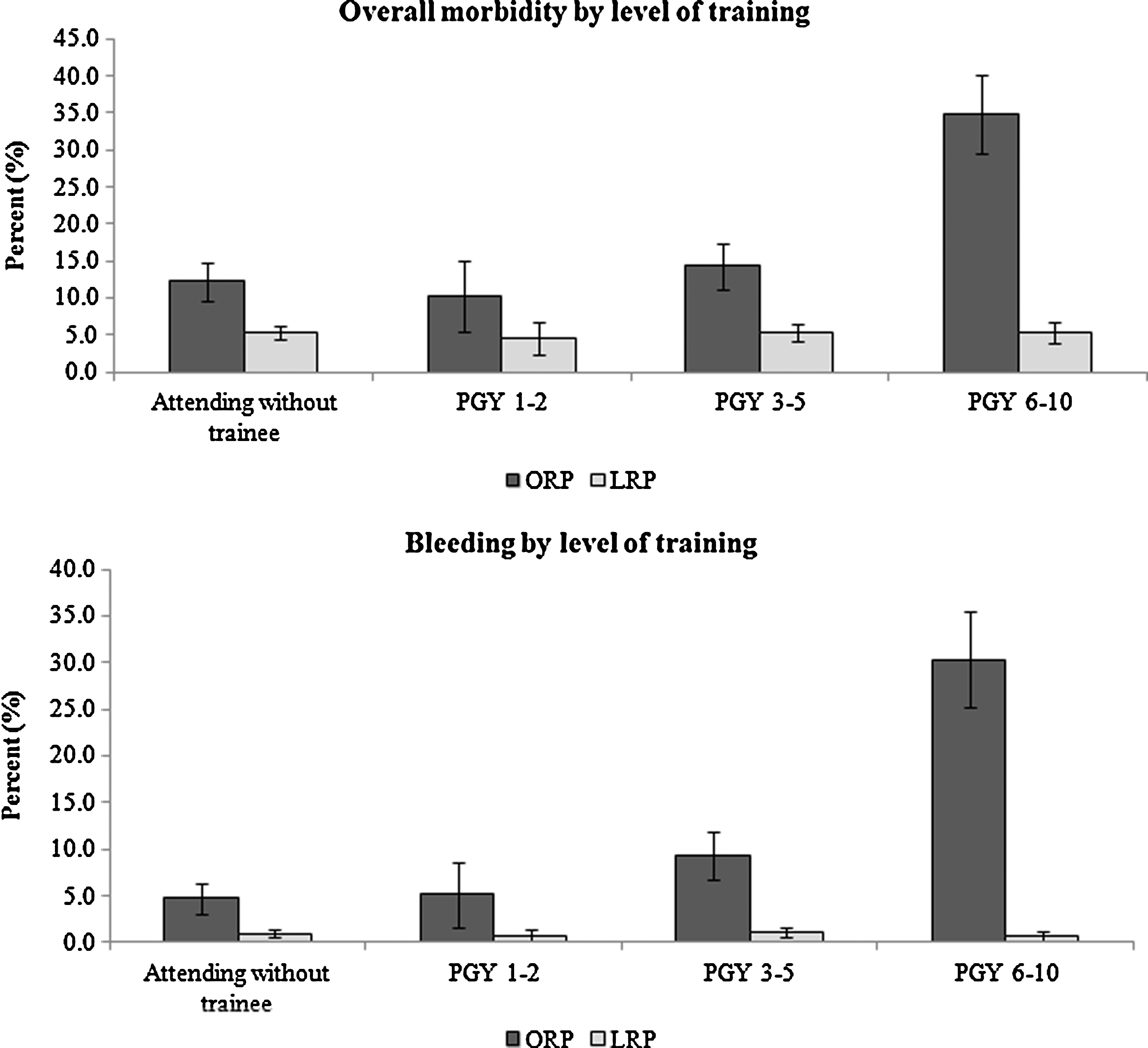
Thirty-day overall morbidity and bleeding stratified by laparoscopic radical prostatectomy (LRP) versus open radical prostatectomy (ORP) and postgraduate year (PGY) experience. Limited to data set containing PGY status, attending variable (n=6737 [ORP=1580 LRP=5157]). PGY 6–10 involved with ORP higher morbidity and bleeding compared with all other groups (p<0.001). LRP shows no difference between any experience group in morbidity or bleeding (p=0.933 and 0.661, respectively).
Statistically significant.
Stroke or cerebrovascular accident, coma lasting >24 hours, or peripheral neurological deficit.
Bleeding requiring transfusion from surgical start time to 72 hours postoperatively.
CPR=cardiopulmonary resuscitation; DVT=deep vein thrombosis; SSI=surgical site infection.
Utilizing risk-adjusted models, patients undergoing LRP were significantly less likely to suffer overall morbidity (OR: 0.28, 95% CI: 0.23, 0.33) (Table 3). Demographics and other risk factors were evaluated and noted significantly increased risk of morbidity of either procedure with increasing age, dyspnea at rest, dyspnea on moderate exertion, poor functional status, renal failure, prior sepsis, alcohol use, and tobacco use. When isolated to the trainee involvement data set, the LRP versus ORP risk-adjustment analysis for overall morbidity favored LRP versus ORP although failed to reach statistical significance in the PGY 1–2 group (OR: 0.11–0.41, 95% lower bound [LB]: 0.07–0.3, upper bound [UB]: 0.15–0.86, p<0.001–0.018). When isolated by surgery, there was no difference in morbidity among PGY 1–10 versus attending without trainee in LRP (OR: 0.83–0.99, LB: 0.48–0.75, UB: 1.31–1.44, p=0.512–0.937). In the ORP group, there was a significantly higher risk of morbidity in the PGY 6–10 group versus attending without trainee (OR: 3.85, CI: 2.75, 5.38, p<0.0001). PGY 1–2 versus attending without trainee, and PGY 3–5 versus attending without trainee showed no significant increased risk of morbidity (OR: 0.82 and 1.2, CI: 0.47, 1.46, and 0.85–1.7, p=0.5 and 0.29, respectively). See Table 3 for summary of risk-adjusted analysis.
Interaction p-value =<0.001. Interaction model limited to data set with included PGY/attending variable completed.
Statistically significant.
CI=confidence interval; OR=odds ratio.
Mean operative times were significantly shorter in the ORP versus LRP group, and attending without trainee cases were faster than any cases involving trainees. Operative times for ORP ranged from 158 to 189 minutes (attending without trainee 158±68 minutes, PGY 1–5 189±88 minutes p<0.05). Operative times for LRP ranged from 200 to 222 minutes (attending without trainee 200±73 minutes, PGY 1–5 222±73 minutes p<0.05). With increasing experience, operative times decreased between PGY 1–2, 3–5, and 6–10, respectively, for both LRP and ORP (Fig. 3). LOS data were evaluated as well. Mean LOS was significantly shorter for LRP versus ORP for all experience groups (1.8±1.9 vs. 3.0±3.3 days [mean±standard deviation]; p<0.001).

Proportion of cases completed within specified time intervals showing a significant difference in mean operative times utilizing ACS-NSQIP, 2005–2011. ANOVA p-value<0.001 for both LRP and ORP.
Discussion
This study examined the incidence of morbidity and mortality as well as underlying risk factors of patients undergoing LRP or ORP at ACS-NSQIP participating hospitals. We evaluated the association of trainee involvement with these outcomes. We also examined operative times as well as LOS associated with LRP and ORP and how this related to resident and fellow involvement in the case.
As reported in other studies, LRP was associated with decreased morbidity (particularly bleeding), decreased LOS, and longer operating times. 6,8,9,16 –19 Previously, resident involvement has been evaluated in ORP using the Veterans Affairs-NSQIP data from 2001 to 2004 by Ku et al. At that time, the authors noted increased operative times, but no difference in transfusion rates between academic and nonacademic centers (academic centers defined as >50% of ORPs having resident involvement). Furthermore, data collection at that time period did not allow in-depth analysis of PGY status as the more recent ACS-NSQIP data collection allows. 13 To our knowledge, our study represents the first to specifically evaluate the safety of both ORP and LRP as it relates to trainee involvement. In reviewing two of the largest relevant studies on this topic, representing 19,462 and 286,876 patients respectively, perioperative complication rates for ORP ranged from 11.1% to 17.9%, and LRP ranged from 7.8% to 11.1%. 8,9 Our analysis demonstrated 18.7% and 5.4% overall morbidity of ORP and LRP, respectively. Stratified by experience levels, PGY 1–2, 3–5, 6–10, and attending alone performing ORP demonstrated complications at a rate of 10.3%, 14.3%, 34.8%, and 12.2%, respectively (p<0.0001). For LRP, these rates were much lower at 4.5%, 5.3%, 5.3%, and 5.4%, respectively (p=0.933). With the exception of senior residents and fellows involved in ORP, all cases that involved trainee participation were associated with equivalent or less morbidity than that reported in other studies. 8,9,20 –22 In ORP cases, this increased morbidity was driven by bleeding rates in the PGY 6–10 group (30.4% vs. 4.7% for attending without trainee). Increased morbidity in cases involving resident surgeons has been demonstrated previously in the general surgical literature, 23,24 and increased morbidity with senior residents, as compared with junior, has further been demonstrated in the vascular surgical literature. 25 We speculate that increased morbidity in the PGY 6–10 group performing ORP is likely attributable to increased trainee participation in critical parts of these difficult cases. It is intuitive that perioperative morbidity may be higher, that is, bleeding. However, this was not seen in the LRP group, even as resident and fellow experience increased. We think that this represents one of the two scenarios. Either trainees are not participating to the same extent in LRP versus ORP, or LRP is in fact a safer surgery, even when surgical trainees are involved. As stated above, ACS-NSQIP does not record the level to which a trainee participated in the case. This variable was present in an earlier version of the NSQIP database, however, was not recorded during the timeframe of our study. 13 Several studies have evaluated the increased usage of LRP over ORP in the past decade, 9,10,26 and this was further reflected in our study, with LRP accounting for 78.6% of the total prostatectomies over the 6-year timeframe, and of these, residents and fellows participated in 2864. Whereas speculative, it is possible that we are seeing the effect of decreased exposure of trainees to ORP, as compared with Ku et al.'s series, 13 and thus, more morbidity when the cases do occur. Whereas LRP has been shown safe and efficacious, 3 –10 most would agree that a surgeon should be facile and confident in performing an ORP before they can safely perform LRP.
Our analysis included operative times, and as expected, the operative times were faster with further experience. However, operative times by PGY grouping did not correlate with risk of morbidity. In the LRP group, the 22 minutes separating the attending without trainee group from the PGY 1–5 group did not change the morbidity. In the ORP group, the PGY 6–10 group averaged 16 minutes faster than the PGY 1–5 group, although it had significantly more morbidity. This is in contrast to previously reported surgical literature. 24,25
Limitations
One of the strengths of the ACS-NSQIP is its standardized variable collection system. However, in this database, we lose the ability to evaluate disease-specific variables of interest, that is, tumor stage, erectile function, continence rates, and margin status. In addition, it does not objectively quantify the extent of trainee involvement, it only records the most senior trainee involved in the case. In the timeframe of our study, there was no CPT code or modifier to reliably distinguish robotic-assisted laparoscopic prostatectomy (RALP) from pure laparoscopic prostatectomy and as such, all LRP in our study are not differentiated. However, the national trend has been abandonment of the pure laparoscopic prostatectomy in favor of the RALP. Trinh et al. reported in an analysis of a similar database, the Nationwide Inpatient Sample, that by 2009, only 0.9% of all LRP were performed without robotic assistance. 9 It is reasonable to infer that the ACS-NSQIP accrual represented similar procedure demographics. The robust sample size of the ACS-NSQIP database certainly adds power to the study, although it has the potential for over interpretation, lending statistical significance to findings that may not be clinically significant. Therefore, subtle differences that are found need to be evaluated with a certain level of discernment.
Conclusions
Using a high quality, nationally validated, risk-adjusted database of surgical clinical variables, we have evaluated the 30-day outcomes of over 10,000 patients undergoing prostatectomy from 2005 to 2011. We have specifically analyzed how these outcomes are impacted by the involvement of surgical residents and fellows. To our knowledge, this represents the first usage of the ACS-NSQIP database to evaluate resident and fellow involvement relating to the ORP and LRP, and we have concluded that LRP appears to be a safer procedure, regardless of resident or fellow involvement with the case. The increased complications in ORP with trainee and particularly senior resident and fellow involvement cannot be ignored, nor can the participation of senior resident and fellows in ORP be curtailed, as active participation is essential for surgical training. Mitigating risk to patients, while maximizing effective training, will remain a challenge to the medical field as we move forward. Future morbidity may be diminished with increased awareness, competency assessment, and strong mentorship from experienced attending surgeons.
LRP demonstrates less morbidity than ORP: an analysis of the ACS-NSQIP database with a focus on surgical trainee involvement.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.