
Abstract
Background and Purpose:
Raising urinary pH and citrate excretion with alkali citrate therapy has been a widely used treatment in calcium nephrolithiasis. Citrate lowers ionized Ca+2 concentrations and inhibits calcium salt precipitation. Conservative alternatives containing citrate such as fruit juices have been investigated and recommended. Any compound that induces systemic alkalosis will increase citraturia. Malate, a polycarboxylic anion like citrate, is a potential candidate for chelating Ca+2 and for inducing systemic alkalinization. We undertook to investigate these possibilities.
Materials and Methods:
Theoretical modeling of malic acid's effects on urinary Ca+2 concentration and supersaturation (SS) of calcium salts was achieved using the speciation program JESS. Malic acid (1200 mg/day) was ingested for 7 days by eight healthy subjects. Urines (24 hours) were collected at baseline and on day 7. They were analyzed for routine lithogenic components, including pH and citrate. Chemical speciation and SS were calculated in both urines.
Results:
Modeling showed that complexation between calcium and malate at physiological concentrations of the latter would have no effect on SS. Administration of the supplement induced statistically significant increases in pH and citraturia. The calculated concentration of Ca+2 and concomitant SS calcium oxalate (CaOx) decreased after supplementation, but these were not statistically significant. SS for the calcium phosphate salts hydroxyapatite and tricalcium phosphate increased significantly as a consequence of the elevation in pH, but values for brushite and octacalcium phosphate did not change significantly.
Conclusions:
We speculate that consumption of malic acid induced systemic alkalinization leading to reduced renal tubular reabsorption and metabolism of citrate, and an increase in excretion of the latter. The decrease in SS(CaOx) was caused by enhanced complexation of Ca+2 by citrate. We conclude that malic acid supplementation may be useful for conservative treatment of calcium renal stone disease by virtue of its capacity to induce these effects.
Introduction
T
There are two possible fates for ingested Cit. When absorbed from the gastrointestinal tract, most of it is oxidized in the liver to form bicarbonate, thereby leading to systemic alkalinization and an increase in the excretion of urinary Cit as mentioned above. 17,25,26 On the other hand, some of the absorbed Cit escapes oxidation and degradation in the liver, also increasing citraturia. 27 These mechanisms depend on the chemical speciation of the ingested Cit. When it is taken as the acid, the effect on acid base status is minimal. 17,25,26 However, when it is ingested as the potassium or sodium salt, oxidation to bicarbonate in the liver leading to alkalinization of the urine, is favored. 17,25,26 It appears that the latter process is more crucial for increasing urinary Cit excretion than the delivery of unmetabolized Cit in the kidney. 28 Hence, most citrate-containing preparations are composed of the potassium or sodium salt, or a mixture of both. Alternative forms of therapy, with an equivalent capacity to raise urinary citrate while delivering an alkali load, have also been sought. Fruit juices have been identified as an excellent prospect and have been investigated in numerous studies. 26,29,30 –41
Owing to the perceived requirement to deliver citrate as the potassium salt rather than the protonated species, research has focused on fruit juices derived from oranges 26,31,35,38 and grapefruit, 33 –35 which contain potassium citrate (KCit), 16,37,38 but others such as lemon, 29,30,32,38,39,41 apple, 35 cranberry, 36,37,42 lime, 26,40 and blackcurrant 42 have also been investigated. The effects of calcium fortified orange juice have also been investigated. 43 Results have been very good for all of the above-mentioned fruit juices with regard to raising urinary citrate excretion, 29,30 –35,38,41,42 but limited with regard to increasing urinary pH. Alarmingly, urinary oxalate increased after fruit juice consumption in several studies involving orange, 31,38 grapefruit, 33 cranberry, 37,42 and blackcurrant. 42 Another unfavorable aspect of fruit juices is that, except for lime or lemon, they are notoriously high in calories. 17 It is therefore apparent that fruit juices, irrespective of whether or not they are rich in potassium, are not ideal alternatives to KCit therapy.
The metabolism of organic anions is known to result in an alkalinizing effect. 28 In two recent articles, the point has been made that any compound that induces a systemic alkalosis will increase Cit excretion and that malate (Mal) being a polycarboxylic anion like Cit, is a potential candidate in this regard. 25,26 Whereas Eisner and coworkers merely theoretically predicted such an effect, 25 da Cunha and colleagues empirically demonstrated an increase in urinary pH and Cit excretion in hypocitraturic stone patients after ingestion of melon, a noncitrus source of potassium, Cit, and Mal. 26 Although this latter study was partly motivated by the potential role of malate, the authors did not explore this in their discussion, presumably because they could not directly or indirectly attribute the observed increase in citraturia to Mal per se, since the test substance also contained citric acid and Cit. 26 We share the view of the latter authors that Mal may affect citraturia. As such, we believe that a further, more focused investigation of this potential effect is warranted.
Like citrate, the possibility of urinary Mal arriving unmetabolized in the urine and being a chelator of calcium, is also worthy of investigation. This notion was first raised by Coe and colleagues who cited two studies in which oral doses of this substance reduced experimental urolithiasis in the rat, and used them to motivate the administration of orange juice fortified with a mixed calcium citrate malate salt in nonstone-forming hypercalciuric subjects. 43 Although decreases in urinary Ca and SS(CaOx) did not occur, increases in urinary citrate and pH were observed.
Further recognition of the possibility that malate may form soluble complexes with calcium in urine was indirectly noted by Brown and coworkers, who included equilibrium constants for [CaMal] and [CaHMal]+1 complexes in the database of the most recent version of the well-known and extensively used speciation program EQUIL. 44 We therefore believe that Mal's potential role as a species for complexing ionized calcium in urine also warrants further investigation.
Materials and Methods
Rationale for modeling the effect of Mal concentrations on SS values
The extent to which Ca-to-Mal complexes will form in urine compared to Ca-to-Cit complexes depends on the relative concentrations of the various ligands (Mal−2, HMal−1, Cit−3, HCit−2, H2Cit−1) (which depend in turn on pH and the initial total concentrations of malic and citric acids, respectively), and the relative magnitudes of the formation constants (K) for the various complexes themselves. The urinary concentration of Cit is typically 1.19 mM, 45 while that of Mal is 0.112 mM. 46 Thermodynamic constants for citric and malic acid and their respective Ca complexes are given in Table 1. 44,47
These pKa values differ from those cited by Hamm, 24 but have been verified by the authors using independent sources.
The table shows that pKa1 and pKa2 of both malic acid and citric acid are well below the normal pH of urine. Therefore at urinary pH, malic acid will be fully dissociated. However, pKa3 of citric acid lies within the normal pH range for urine and as such, only about 50% of [HCit]−2 will lose its remaining proton. Nevertheless, log K values show that the [CaCit]−1 species is ∼100-fold more stable than the corresponding [CaMal] complex (Table 1). Thus, notwithstanding that Ca+2 would have to displace a proton from [HCit]−2 to form [CaCit]−1, Mal is unlikely to compete with Cit in reducing ionized Ca+2. Similarly, comparison of the deduced log K values for the coordination of [Ca+2] to [HCit]−2 to form the complex [CaHCit] (i.e., 9.13–6.38=2.75) and for the coordination of [Ca+2] to [HMal]−1 to form the complex [CaHMal]+1 (i.e., 3.02–4.68=−1.66), shows that [CaHCit] is over four orders of magnitude more stable than [CaHMal]+1. Again it can be concluded that formation of [CaHMal]+1 will have a negligible effect on the concentration of ionized Ca+2 relative to [CaHCit].
These arguments indicate that at its physiological concentration in urine, the chelation of Mal−2 with Ca+2 is likely to be negligible. Accordingly, we undertook to test this hypothesis by modeling the effect of malate concentrations on the SS of CaOx monohydrate (COM) and brushite (Bru). In so doing, we noted that Coe and coworkers reported a mean urinary baseline concentration for malic acid of 29 mg/dL. 43 This converts to 2.16 mM, which is nearly 20 times greater than the concentration reported by Zaura and Metcoff. 46 Because of this uncertainty about the urinary concentration of Mal, we ensured that both concentration levels were covered in our modeling calculations.
Effect of malic acid supplementation on urinary Cit and pH
Study design
Eight healthy white males (aged 18–20 years) with no history of kidney stone disease were recruited for the study. They were instructed to drink at least 1.5 L of Cape Town tap water (Ca: 13 ppm, Mg: 1 ppm), 48 for 3 days preceding collection of the first urine sample (baseline) as well as on each day of the study period. This was in accordance with our in-house procedure in all investigations to ensure adequate urine outputs. All participants were advised to avoid or limit their daily intake of foods that were rich in calcium, oxalate, Cit, and/or Mal during the entire period of investigation. Twenty-four-hour food diaries were recorded at baseline and on the final day of the test period to assess whether any dietary conflicts had occurred. Daily nutrient intakes were computed from these diaries using the Foodfinder™ software program. 49
Each subject provided a 24-hour urine before commencement of the malic acid ingestion period. These were used as baseline samples. Supplementation commenced thereafter. A malic acid health supplement (Malic Acid Extra Strength; Ampiro, Johannesburg, South Africa) was administered each day for 7 days. Participants ingested two tablets at breakfast and two tablets at dinner. Two tablets delivered 600 mg of malic acid (Table 2). In addition to baseline urine samples, subjects provided 24-hour urine collections on the final day of supplementation.
Urine treatment
Urines were tested for the presence of blood and infection (Combur 10 test strip; Boehringer Mannheim, Mannheim, Germany) and were discarded if the test was positive. Each urine was filtered through a 0.75-μm prefilter and a 0.45-μm cellulose nitrate filter before analysis to remove cellular debris and proteinaceous material. They were then analyzed routinely for pH, Cit, oxalate, Ca, Mg, Na, K, creatinine, phosphate, urate, and chloride as described elsewhere. 50
Theoretical modeling of the effect of urinary malate
Urine composition data obtained for the baseline urines were used as the input model for the speciation program JESS. 51,52 This model was then altered to include Mal at its physiologically reported concentration of 0.112 mM. 46 The scan option in JESS was then invoked to determine the concentration of the species Ca+2 and concomitant SS values as a function of Mal concentrations over a range of 1–100× its physiological concentration. All other parameters in the baseline model were left unchanged.
Calculation of speciation concentrations and SS values before and after malic acid consumption
JESS was also used to calculate the concentrations of calcium and phosphate speciation and SS values for COM and several CaP salts—Bru, hydroxyapatite (HAP), octacalcium phosphate (OCP), and tricalcium phosphate (triCaP)—in the unaltered baseline samples and in samples obtained after 7 days of malic acid supplementation.
Statistical analysis
Statistical analyses were conducted using GraphPad InStat 3.06 (GraphPad Software, Inc., La Jolla, CA). Mean values and standard errors of the mean are reported for the urine data. Significant differences were assessed using a t-test and p-values less than 0.05 were regarded as significant.
Results
Theoretical modeling
The variation in SS(COM) and SS(Bru) as a function of urinary malic acid concentration in the range 1–100× its physiological level, is shown in Figure 1. The concomitant concentrations of the various Ca species at selected concentrations within the same range are shown in Figure 2.
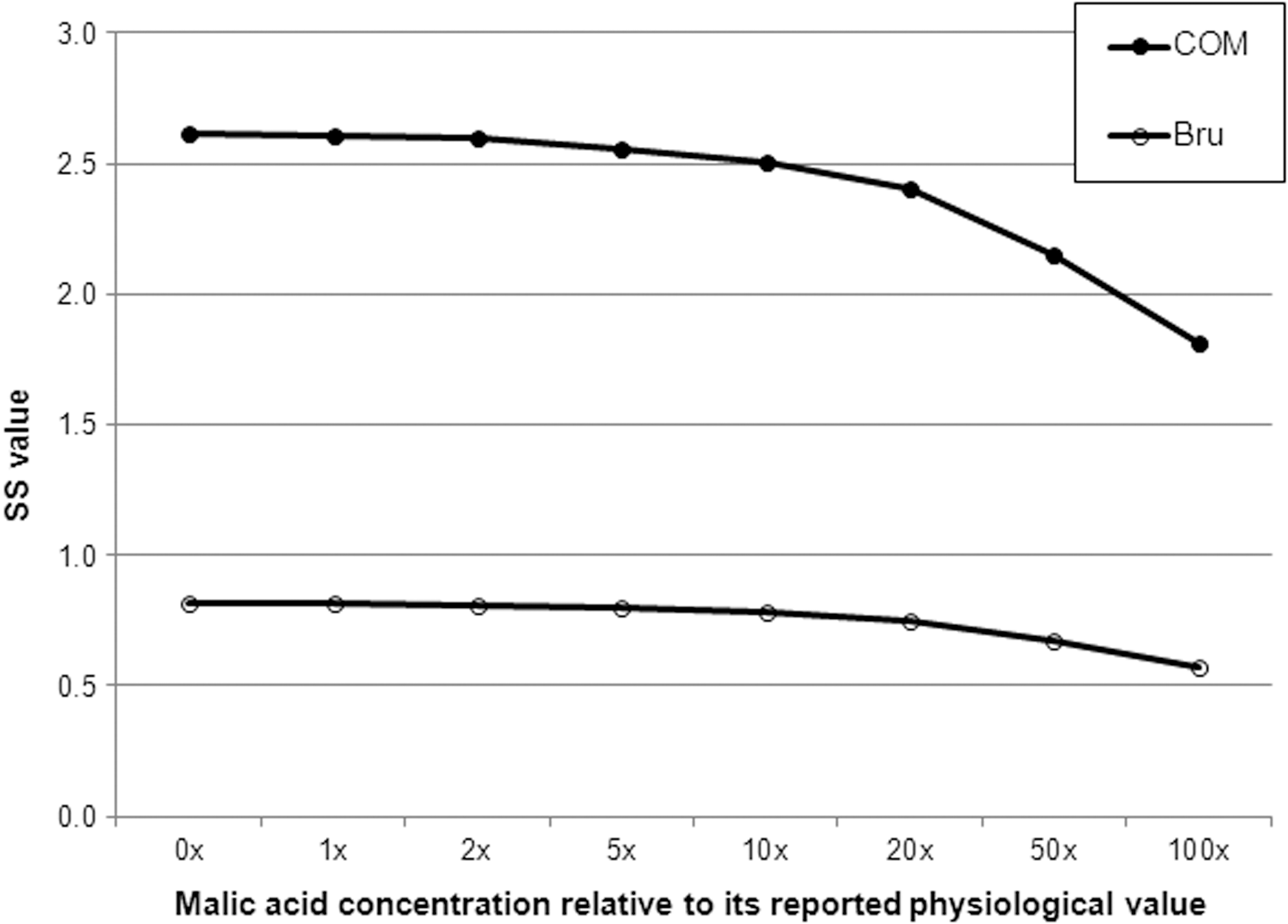
Computer modeling of SS(CaOx monohydrate [COM]) and SS(brushite [Bru]) as a function of urinary malic acid concentration.
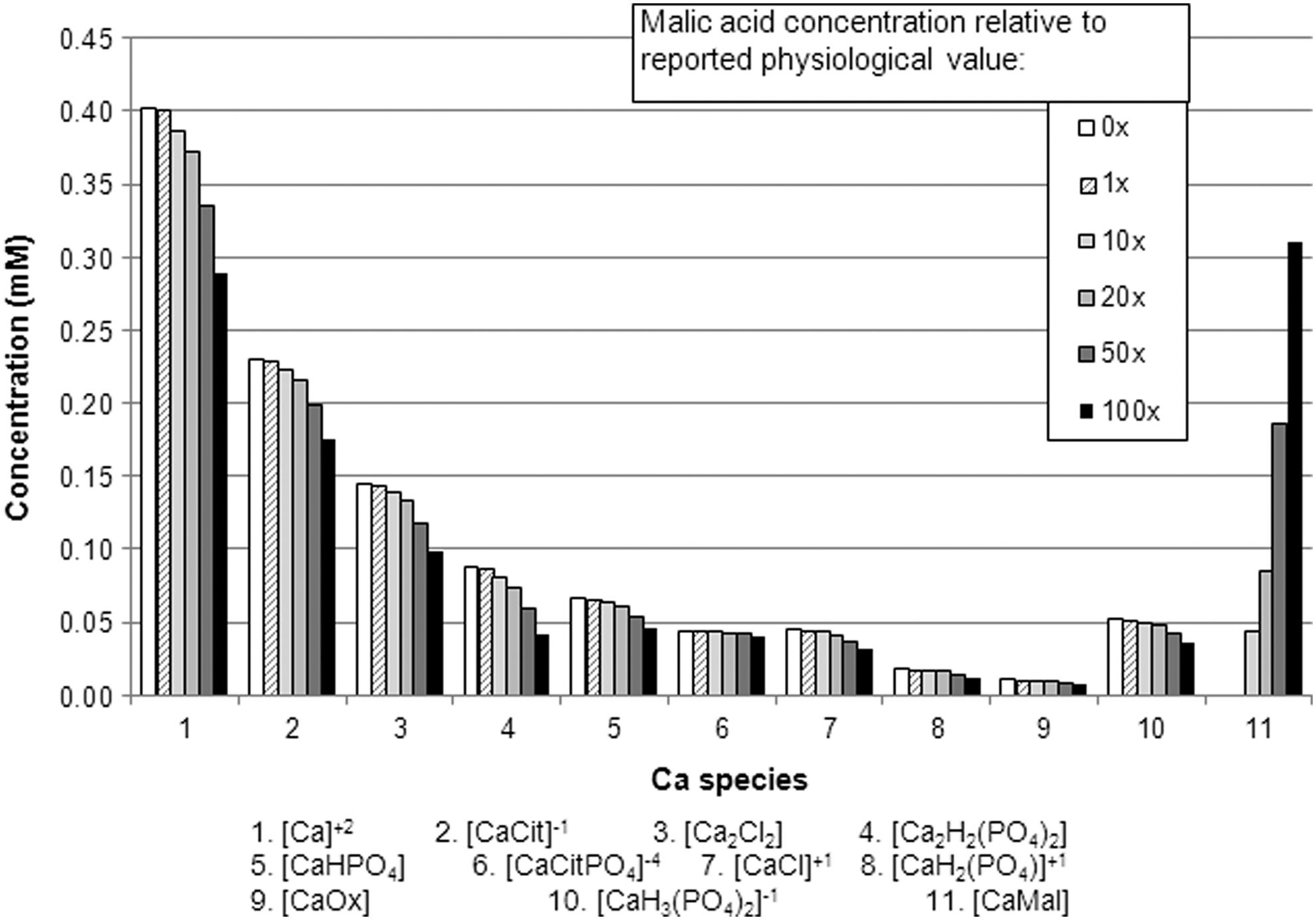
Computer modeling of the concentration of Ca speciation as a function of urinary malic acid concentration.
Figure 1 shows that malic acid has no effect on SS values at its physiological concentration, as predicted by our physicochemical arguments presented in the Materials and Methods section above. Effects on SS(COM) and SS(Bru) become relevant only when the concentrations of malic acid reach 50× and 100× its normal level, respectively. This can be accounted for by the progressive decrease in the concentrations of [Ca+2] with increasing malic acid concentrations (Fig. 2). The decrease in the concentration of [Ca+2] is itself explained by utilization of Ca+2 in the formation of the [CaMal] complex (species 11, Fig. 2). Not unexpectedly, the concentrations of all Ca species decrease as the concentration of malic acid increases because of the increasing utilization of Ca+2 (Fig. 2). Interestingly, it is only when the concentration of malic acid is at 50× its physiological level, that the concentration of [CaMal] (0.18 mM; species 11, Fig. 2) becomes approximately equal to that of [CaCit]−1 (0.20 mM; species 2, Fig. 2), again confirming our earlier prediction that [CaMal] would not be able to compete with [CaCit]−1 at physiological concentrations.
Dietary analysis
Mean dietary intake values at baseline and on the final day of malic acid supplementation are given in Table 3 (ingestion of the supplement itself is not reflected in the table). No statistically significant differences were observed, indicating the absence of any conflicting dietary factors. Any changes in urine composition observed after completion of the test period can therefore be attributed to ingestion of the supplement.
Malic acid supplementation
Mean values (and standard errors) for measured and calculated urinary parameters at baseline and after supplementation with malic acid are reported in Table 4. Urinary pH and excretion of Cit and Mg increased significantly after ingestion of the malic acid supplement. SS(HAP) and SS(triCaP) also increased significantly. None of the other urinary parameters changed significantly after supplementation. The concentrations of several relevant calcium and phosphate species before and after Mal supplementation are shown in Figures 3 and 4, respectively.

Calculated concentrations of calcium speciation before and after malic acid supplementation.

Calculated concentrations of phosphate speciation before and after malic acid supplementation.
Significant difference relative to baseline: p<0.05.
Ox=oxalate; Creat=creatinine; SS=supersaturation; COM=CaOx monohydrate; Bru=brushite; HAP=hydroxyapatite; OCP=octacalcium phosphate; triCaP=tricalcium phosphate.
Discussion
Our modeling exercises have indicated that the possibility of malate playing a protective role in calcium urolithiasis by virtue of its capacity to bind Ca+2 and thereby reduce SS(CaOx) and SS(Bru), is remote. Its concentration in urine is far too low for it to have such an effect. Elevating its concentration to levels at which it would be effective in this regard is unlikely to be feasible clinically.
However, although our results exclude Mal as a possible chelator of Ca in urine, they have shown that it has the potential to play a protective role in another context, namely, as a conservative therapy for increasing urinary pH and Cit. The mechanism by which this may have occurred deserves interrogation. The liver is the major site for metabolism of organic anions such as citrate and malate. 28 Irrespective of the pathways involved, the carbon atoms in these species are finally oxidized to CO2 in equilibrium with circulating HCO3 −2 in extracellular fluids. 28 Current thinking on the metabolism and urinary handling of citrate dictates that its urinary excretion is determined by total acid-base balance. 23 –26 Citraturia is raised when alkalosis occurs because it reduces renal tubular reabsorption and metabolism of citrate. 23,26 The acid-base balance can be influenced by the ingestion of citrus juices, but depends on the alkali load that they are able to deliver, that is, it depends on the speciation of the Cit in the juices themselves. 25,26 If the ingested juice contains the protonated form, that is, the pure acid, the bicarbonate, which is formed during metabolism in the liver, is neutralized by H+ ions; there is no effect on acid-base status and the citraturic response is minimal. 17,25 However, if the administered Cit speciation is in the form of the potassium salt, virtually all of it is converted to alkali, leading to an increase in urinary pH and a concomitant increase in Cit excretion. 17,25,26 Our results show that a statistically significant increase in pH occurred, despite our test substance being in the protonated form. This is contrary to the previously expounded hypothesis described above. It is not obvious to us how this may have occurred, but we note that Penniston and coworkers found an increase in urinary pH after the administration of lemon juice, 29 which is also contrary to the hypothesis, since lemon juice contains citric acid (as opposed to KCit). 38 These authors did not offer an explanation for their unexpected result. 29 However, irrespective of the mechanism by which pH increased in that study or in the present one, several workers have stated that any compound that causes systemic alkalosis will cause an increase in Cit excretion. 25,26,28 Indeed, this is what has occurred in our study. We therefore conclude that consumption of malic acid induced systemic alkalinization leading to reduced renal tubular reabsorption and metabolism of Cit and an increase in the excretion of the latter.
We are unable to compare our results with those of others since there is no other study dedicated to investigating the effects of ingesting malic acid, either in the protonated or alkali salt form, on urinary alkalinization and citraturia. However, da Cunha and coworkers investigated the effects of consuming melon juice containing relatively high levels of malate. 26 In their study, 331 mg of malate was delivered in a single dose (compared with 1200 mg of malic acid per day for 7 days in our study) and the acute effects were measured in urine fractions collected at 2-hour intervals for 6 hours after consumption (compared with 24-hour urines collected on day 7 in our study). They recorded an increase in urinary pH from 6.16 to 6.72 (compared with an increase from 6.13 to 6.48 in our study) and an increase in citraturia from 0.22 to 0.35 mg/mg creatinine (compared with 0.19–0.28 mg/mg creatinine in our study). Recognizing that the melon used in the study by da Cunha and colleagues also contained 894 mg KCit and 408 mg citric acid, our results for malic acid alone are noteworthy.
In general, significant increases in urinary Cit excretion and urinary pH as observed in the present study would be expected to cause decreases in the concentration of ionized Ca+2, with a concomitant decrease in SS(COM). Inspection of the concentrations of various calcium species before and after ingestion of malic acid (Fig. 3) shows that those of the Cit-containing complexes [CaCit]−1 and [CaCitPO4]−4 increase in the postmalic acid urines as a consequence of the increased excretion of Cit. The concentrations of [Ca2H2(PO4)2] and [CaHPO4] also increase (Fig. 3), but these do so as a consequence of the increased pH. The raised concentrations of all of these complexes utilize more of the available calcium, thereby causing a decrease in the concentration of ionized [Ca+2] (Table 4, Fig. 3). However, notwithstanding this decrease, the concomitant decrease in SS(COM) was not statistically significant (Table 4). Nevertheless, these results are promising. Perhaps, larger doses of malic acid in future studies and/or a longer duration for ingestion might induce larger increases in Cit excretion and urinary pH ultimately leading to statistically significant decreases in SS(COM).
The SS of two CaP salts (HAP and triCaP) increased significantly after malic acid ingestion (Table 4). We attribute this effect to increased dissociation of phosphate at the elevated pH. 31 Our speciation calculations using the urinary data of the present study demonstrate that the offensive species is [HPO4]−2 (Fig. 4, species 2), in which the increase in its concentration tends toward statistical significance (Table 4). This arises because [H2PO4]−1 (Fig. 4, species 1) loses a proton at the elevated pH. [The concentrations of the corresponding Na complexes (Fig. 4, species 4 and 5, respectively) change accordingly]. Since [HPO4]−2 is a precursor in the formation of urinary CaP salts, 53 increases in the SS of some of these salts may occur. Indeed, increases in SS(Bru) have been previously reported following the ingestion of fruit juice. 31,35,38,43 In one of these studies, an increase in SS(HAP) was also reported. 43 As far as we are aware, the latter study is the only one in which SS(HAP) has been reported, irrespective of whether it increased or not, while SS(triCaP) has not been reported in any such study, so we are not able to compare our findings with those of others. The possible implications of the observed increase in SS(Bru) was ignored by all authors 31,35,38 except by Coe and colleagues who suggested that the increases in SS(Bru) and SS(HAP), which they observed would have little clinical relevance since calcium phosphate stones are extremely rare. 43 Despite this reassurance, increases in the SS values of CaP salts observed by ourselves and others are worth noting.
Our observed decreasing trend in the concentration of [Ca+2] following malic acid ingestion is paradoxical in that, the original speculation was that this effect would indeed occur, but as a result of the formation of soluble [CaMal] complexes. 45 Our modeling showed that this is highly unlikely. Instead, the decrease in the concentration of [Ca+2] occurred because of the formation of [CaCit] complexes, which arose from the increased citrate excretion caused by the systemic alkalinization following malic acid ingestion. Therefore, the latter compound did indeed cause a decrease in the concentration of [Ca+2], but through an indirect route.
The statistically significant increase in the concentration of Mg following malic acid ingestion is due to its presence at a relatively high level in the supplement itself (Table 3). The raised concentration of urinary Mg competes with Ca for binding with oxalate and citrate. Indeed, the concentration of [MgOx] increased from 0.0185 to 0.0288 mM and that of [MgCit]−1 increased from 0.181 to 0.400 mM (not shown in the presented data). However, the additional utilization of oxalate in the formation of [MgOx] was not large enough to cause a statistically significant decrease in the concentration of [Ox]−2 (Table 4), nor was the additional utilization of citrate in the formation of [MgCit]−1 large enough to cause a statistically significant increase in the concentration of [Ca+2] (Table 4). Thus variations, if any, in the SS values for CaOx and CaP salts cannot be attributed to the elevated urinary magnesium.
Our test substance also contained vitamin B6 (Table 2), which is a cofactor in the oxalate metabolic pathway. 54 Supplementation with pyridoxine is known to reduce hyperoxaluria in stone patients. 54,55 It has also been reported in one study as reducing calcium excretion through an unknown mechanism in healthy males. 56 However, no such effects were observed in the present study. Therefore, its presence in the formulation of the test substance does not represent a conflicting factor.
As with most studies, ours has some limitations. Our study group is relatively small (n=8) and did not include stone formers. Whereas it is reasonable to expect that similar effects would be observed in a group of stone formers, future studies involving patients are warranted.
We did not determine malate in our urine samples since methods previously used for such analyses—gas liquid chromatography 46 and a coupled enzyme system— 43 have not demonstrated their reliability compellingly. Development and validation of a selective assay for this purpose was beyond the scope of the present project. Accordingly, we undertook to utilize computer modeling, which we knew would allow us to calculate the effects of a wide range of urinary malate concentrations, including those that might be expected at baseline and after supplementation. Nevertheless, we recognize that determination of urinary malate would have added value to the theoretical speciation modeling and would have shed some light on the different values reported by Zaura and Metcoff 46 and Coe. 43 It would also have allowed us to compare ingested and excreted amounts to evaluate the extent of unmetabolized malic acid reaching the urine.
The results of our study are important for several reasons. First, ours is the first study in which malic acid (or a malate salt) has been administered in the absence of accompanying competing species such as citric acid and/or Cit and the first in which it has been administered in the absence of complex chemical species, which occur in the matrices of fruit juices. We are therefore able to attribute our findings to the action of malic acid unequivocally. Secondly, the effects that we observed were relatively long term over a period of 7 days and occurred in 24-hour urines, as opposed to acute effects observed in fractionally collected samples used in the da Cunha Baia's study, which is the only other study involving (indirect) consumption of malate. 26 Since excretion of urinary lithogenic and antilithogenic substances varies during each 24-hour period, our detection of increases in citraturia and pH over the entire period is encouraging. Third, our results are of interest because they have demonstrated alkalinization and citraturic effects arising from ingestion of a polycarboxylic acid in the protonated state as opposed to the salt form. Indeed, we intend to investigate the effects of potassium malate ingestion in a future study. In this context, the three commonly consumed diet sodas identified by Eisner et al. as having relatively high concentrations of malate as alkali 25 are worth exploring in clinical trials. Finally, our findings are important because they present a new option, deserving of further investigation, for the conservative treatment of calcium nephrolithiasis, by virtue of malic acid's ability to favorably alter urinary pH and citraturia, both of which are key risk factors for this disease. Such investigations should involve stone patients rather than healthy subjects. If malic acid's potential as a therapeutic agent is realized, it would offer advantages over KCit in terms of lower costs and no side effects.
Conclusions
Malic acid administered as a supplement may be useful for the conservative treatment of calcium renal stone disease. This is by virtue of its capacity for inducing systemic alkalization leading to an increase in urinary Cit excretion.
Footnotes
Acknowledgments
The authors thank the South African National Research Foundation, the South African Medical Research Council, and the University of Cape Town for financial support.
Disclosure Statement
No competing financial interests exist.