
Abstract
Objective:
To evaluate the feasibility and safety of retroperitoneal laparoendoscopic single-site adrenalectomy for pheochromocytoma (LESS-PHEO) and summarize our initial experience.
Patients and Methods:
Between June 2009 and June 2013, 21 patients with adrenal pheochromocytoma underwent adrenalectomy by means of LESS-PHEO in our department. Fifty-three patients with pheochromocytoma underwent conventional retrolaparoscopic adrenalectomy (RLAP-PHEO) between March 2001 and June 2013, of whom 42 were selected as a control group for a retrospective serial case–control analysis (1:2 matched-pair cohort). In the operation, the retroperitoneal space was created and dilated by blunt finger dissection and the pneumoperitoneal pressure was maintained below 10 mm Hg. As the first step, ligation of the adrenal central vein was performed. Intraoperative hemodynamic parameters, operating time, estimated blood loss, transfusion requirement, incidence of perioperative complications, visual analog pain scale (VAPS) score, time to resumption of oral intake and ambulation, and postoperative hospitalization were compared between the groups.
Results:
All the operations were technically successful, without reoperations or conversion to open procedures. The 24-hour postoperative VAPS score was lower in the LESS-PHEO group than in the control group (5 vs 7; p<0.001). Despite a longer median operative time (167.4 minutes vs 125.5 minutes; p<0.001), the patients in the LESS-PHEO group resumed oral intake sooner (1 day vs 2 days; p<0.001), ambulated sooner (1 day vs 2 days; p<0.001), and were discharged earlier (4 days vs 7 days; p<0.001). No perioperative complications occurred in both the groups. No statistically significant differences in hemodynamic parameters or estimated blood loss were found between the groups.
Conclusion:
Although more training and practice are needed to shorten its operative time, LESS-PHEO, as performed by an experienced laparoscopic urologist, is a feasible and safe procedure associated with less postoperative pain and faster recovery.
Introduction
S
Although there have been great expectations for this procedure based on the clinical trials and assessments, most reported cases have been for primary aldosteronism, Cushing syndrome, and nonfunctional tumors; only a few of these reports referred to or focused on adrenal pheochromocytoma. From March 2001 to June 2013, members of our department performed adrenalectomy on 74 patients with adrenal pheochromocytoma. Conventional retrolaparoscopic adrenalectomy for pheochromocytoma (RLAP-PHEO) was used for 53 patients, and laparoendoscopic single-site adrenalectomy for pheochromocytoma (LESS-PHEO) was used for the other 21 in the recent 4 years (between June 2009 and June 2013). We performed a retrospective case–control analysis by designing 1:2 matched-pair cohorts to investigate whether the patients benefitted more from one type of procedure.
Patients and Methods
General patient data
Between March 2001 and June 2013, 53 patients with pheochromocytoma underwent laparoscopic adrenalectomy in our department by RLAP-PHEO. Between June 2009 and June 2013, 21 patients diagnosed as adrenal pheochromocytoma received LESS-PHEO after acquiring informed consent to choose LESS-PHEO as their first surgical option and conversion to RLAP or open way if necessary intraoperatively. The clinical diagnoses of pheochromocytoma were based on symptoms and on biochemical and radiological evaluations before the operation. The postoperative pathological diagnoses of all the enrolled patients were pheochromocytoma and were identical to the preoperative clinical diagnoses. We designed a retrospective series of case–control study by selecting 42 patients of the 53 who underwent RLAP-PHEO to serve as a control group. In addition, we set the exclusion criteria as below: patients with bilateral pheochromocytomas or who had a history of retroperitoneal laparoendoscopic surgery. The 42 patients were matched to the patients who underwent LESS-PHEO in a 2:1 ratio on the characteristics of sex, age, body mass index, tumor size, tumor laterality, and American Society of Anesthesiologists grade, respectively. Rigorous case-by-case matching was performed to ensure that the control subjects matched the cases as closely as possible with regard to numerous factors other than outcome measures. No consideration or analysis of surgical parameters and outcomes was made until this control group had been selected based only on preoperative variables. This study was approved by the institutional review board of our hospital. The detailed demographic data of the patients are listed in Table 1.
LESS-PHEO=laparoendoscopic single-site adrenalectomy for pheochromocytoma; RLAP-PHEO=retrolaparoscopic adrenalectomy for pheochromocytoma; BMI=body mass index; ASA=American Society of Anesthesiologists.
Preoperative preparation and anesthesia
All the 63 patients received an alpha-adrenergic blocker (doxazosin, 4 mg/day) and a beta blocker (metoprolol, 12.5 mg/day) orally for 2 weeks preoperatively to maintain a stable blood pressure (BP) and heart rate (HR). A calcium channel blocker (nifedipine, 10 mg/day) and an angiotensin-converting enzyme inhibitor (captopril, 10 mg/day) were added if hypertension persisted. We provided adequate vascular volume expansion for 3 to 5 days after the patients met the following criteria: BP <140/90 mm Hg, HR <100/min, hematocrit level <0.45%, and warm fingertips for 1 week. As a routine, general anesthesia was induced and tracheal intubation was performed by an experienced team of anesthetists.
Operative methods
All the operations were performed in the Department of Urology, First Hospital of Shanxi Medical University, and all the surgical procedures were performed by a single experienced laparoscopic surgeon as the main operator.
LESS adrenalectomy
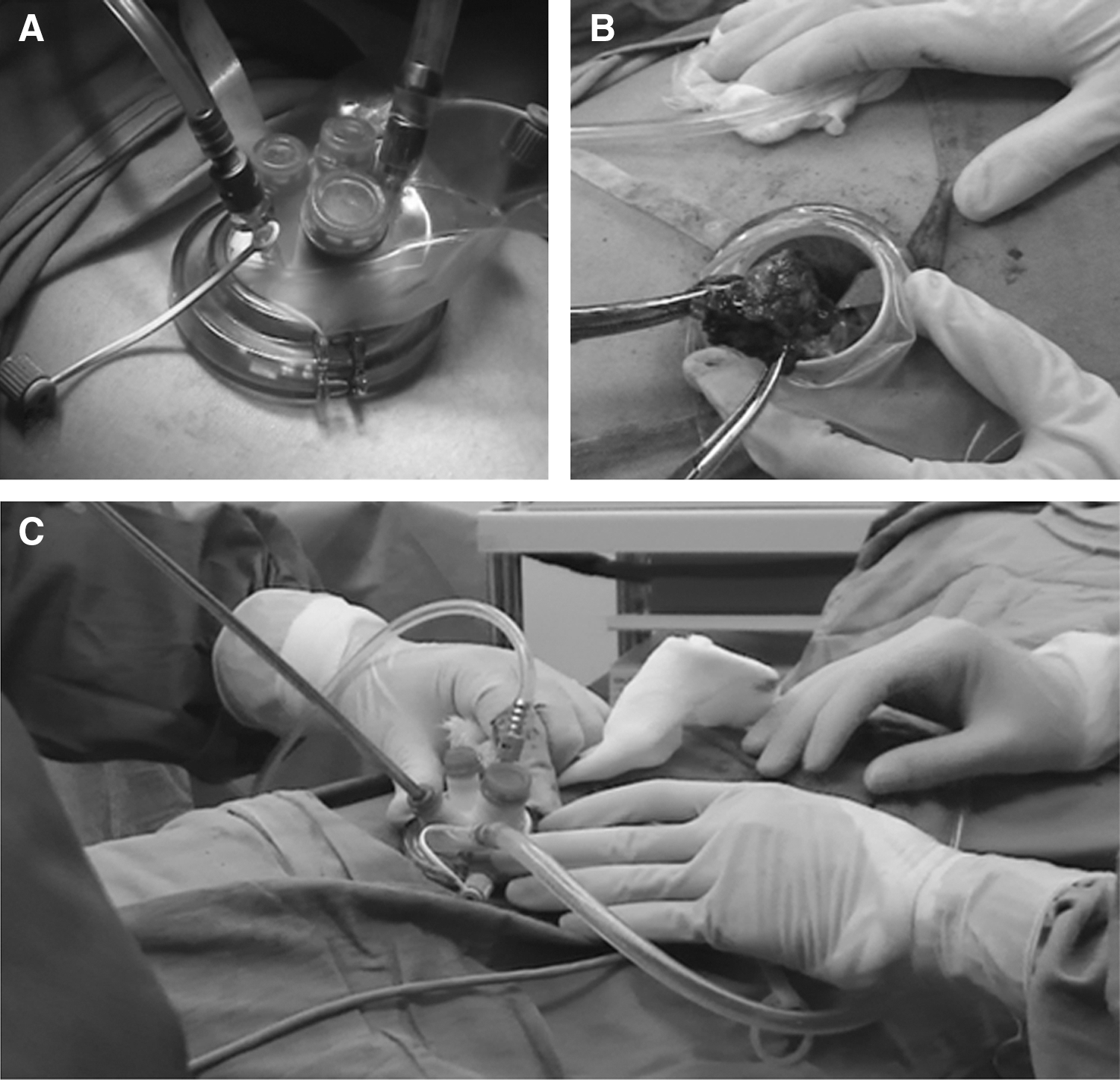
The patient was placed on the operating table in the lateral decubitus position with the affected side upward. All pressure points were padded with beanbags, and secure tapes were used to fix the posture firmly with the optimal table flexion. A longitudinal 2.5- to 3.0-cm incision was made in the axillary midline below the 12th rib, a finger was inserted, and then the retroperitoneal space was carefully dilated and bluntly dissected. A TriPort was inserted after the finger was retracted (Fig. 1). A pneumoperitoneum was established by insufflating carbon dioxide at a pressure of 10 mm Hg. The instruments used were an articulating laparoscopic grasper, a 5-mm harmonic scalpel, a 5-mm rigid laparoscope, and other conventional laparoscopic tools. With the Gerota fascia incised and surrounding fat tissues removed, the first goal was to expose the adrenal central vein and to ligate it using 5-mm Hem-o-lok clips. Then, the tumor was dissociated, and the other adrenal vessels, including the adrenal arteries, were ligated and cut. After careful hemostasis was achieved under a retroperitoneal pressure of 5 mm Hg, the adrenal tumor specimen was removed using the TriPort. When dealing with the tumor that had a diameter longer than 4.0 cm, we will carefully capture and pack the tumor specimen into a homemade laparoscopic pouch with a pulling string, then retrieve the Triport and pouch simultaneously. Even though the tumor diameter is longer than the incision, the successful extraction always can be achieved due to the vigorous dragging by holding the pulling string and the natural elasticity of muscle and skin. Nevertheless, the relatively large tumors can only be extracted with the necessary incision extension. Finally, the incision was carefully closed and a rubber drainage catheter placed through the incision was left in situ when necessary. A video demonstrating this LESS procedure accompanies this article.
Conventional retrolaparoscopic adrenalectomy
The patient's position was the same as that used for LESS-PHEO. A longitudinal 1.5- to 2.0-cm incision was made in the axillary midline below the 12th rib, followed by finger insertion and gentle dilation of the retroperitoneal space with blunt dissection. Under protection of a finger in the cavity, another subcostal 5-mm trocar was placed, along with a 10-mm trocar above the anterior superior iliac spine. After a pneumoperitoneum was established by insufflating carbon dioxide at a pressure of 10 mm Hg and after retracting the finger, insertion of the 10-mm trocar was completed under laparoscopic guidance. The surgical strategy was similar to that used for LESS-PHEO.
Observed and compared items
Data were collected for operating time, estimated blood loss, transfusion requirement, incidence of perioperative complications, 24-hour postoperative visual analog pain scale (VAPS) score, time to resumption of oral intake and ambulation, and length of hospitalization and were compared between the groups.
Moreover, to evaluate the hemodynamic changes during the course of the operation, we defined significant fluctuation as systolic BP higher than 180 mm Hg or lower than 80 mm Hg or as a diastolic BP higher than 120 mm Hg or lower than 40 mm Hg. We defined tachycardia as a HR faster than 120 bpm and bradycardia as a HR slower than 50 bpm.
Statistical methods
The data were compared between the groups using the chi-square tests and Mann–Whitney U tests for categorical and continuous variables, respectively. Statistical significance was set at p<0.05, and all the reported p-values were two sided. The statistical analysis was accomplished with SPSS 18.0.
Results
No significant statistical differences in the patients' demographic data were found between the groups. All the 63 operations were technically successful, without any case requiring reoperation or conversion to open procedures. The median operating time for the LESS-PHEO group was longer than that for the RLAP-PHEO group (167.4 minutes vs 125.5 minutes; p<0.001). The median estimated blood loss did not differ significantly between the groups (121.5 mL vs 118.0 mL; p=0.361), and no blood transfusions were required. No perioperative complications occurred in both groups. At 24 hours after each operation, we used a questionnaire to assess each patient's VAPS score. The median score of the LESS-PHEO group was lower compared with the RLAP-PHEO group (5 vs 7; p<0.001). The median time for resumption of oral food intake (1 day vs 2 days; p<0.001) and ambulation (1 day vs 2 days; p<0.001), and the length of postoperative hospitalization (4 days vs 7 days; p<0.001) were shorter in the LESS-PHEO group. The intraoperative and postoperative data of the two groups are listed in Table 2.
RLAP-PHEO=retrolaparoscopic adrenalectomy for pheochromocytoma; LESS-PHEO=laparoendoscopic singe-site adrenalectomy for pheochromocytoma; OT=operative time; EBL=estimated blood loss; VAPS=visual analog pain scale.
With regard to intraoperative hemodynamic fluctuation, the data are shown in Table 3. Intraoperative surveillance showed an insignificant difference in the incidence of significant hemodynamic fluctuation between the groups (40.5% vs 28.6%; p=0.355). No significant difference was also found in the incidence of tachycardia between the groups (21.4% vs 28.6%; p=0.530) or bradycardia (7.1% vs 4.8%; p=1.000).
RLAP-PHEO=retrolaparoscopic adrenalectomy for pheochromocytoma; LESS-PHEO=laparoendoscopic singe-site adrenalectomy for pheochromocytoma; SBP=systolic blood pressure; DBP=diastolic blood pressure; HR=heart rate.
Discussion
Because of the excess secretion of catecholamines, which can lead to a lethal disturbance of hemodynamics, operating on pheochromocytomas has been considered to be one of the most challenging tasks that urologic surgeons face. Even after universal acknowledgment that the laparoscopic approach to adrenalectomy is superior, many urologists still instinctively hold cautious opinions on the surgical approach to pheochromocytoma. Improvements in endo-operative and anesthetic techniques, together with the findings of evidence-based medicine, have supported the feasibility and safety of RLAP-PHEO, 13 –20 but those of LESS-PHEO remain to be clarified.
Despite the prominent merits of LESS adrenalectomy, when it comes to LESS-PHEO, most existing studies dispersed these special cases with other adrenal lesions, 8 –10,12 and few reports choose this issue as their specialized focus. To our best knowledge, there is only one published article that of Hattori et al. 21 in October 2012 that describes a clinical trial comparing intraperitoneal LESS-PHEO with laparoscopic adrenalectomy for pheochromocytoma (LAP-PHEO). They collected the perioperative data of 50 patients with pheochromocytoma who underwent adrenalectomy (20 intraperitoneal LESS-PHEO and 30 LAP-PHEO) in their institution. After statistical comparison and analysis between intraperitoneal LESS-PHEO and LAP-PHEO with respect to hemodynamic parameters and surgical outcomes, they found no significant difference between the two groups in terms of operation time, total fluids during the operation, estimated blood loss, resumption of oral feeding, postoperative intensive care unit stay, or postoperative hospital stay. Based on these results, they concluded that intraperitoneal LESS-PHEO is as safe as LAP-PHEO. Likewise, the present study describes our single-institution outcomes and experiences. However, our study differed from their study in that both our LESS-PHEO and control groups underwent operation by the retroperitoneal approach because of the obvious advantages such as less disruption to abdominal organs, lower incidence of intraperitoneal infections, and faster recovery of bowel function. 22
Pacak et al. 23 stressed the importance of appropriate preoperative management to the success of treatment of pheochromocytoma. In our preparation, we set strict standards and a plan for intravascular volume expansion to load adequate fluid into the circulation to buffer the negative effects of possible intraoperative hemodynamic upheavals.
In our research, two important manipulations were made in all operations to decrease the chance of irritating the tumor: blunt finger dissection of the retroperitoneal space instead of balloon dilation and use of pneumoperitoneal pressure below 10 mm Hg. To minimize catecholamine release into the circulation, which can lead to a sudden surge in BP and HR, our first goal was to ligate the adrenal central vein rather than dissociate the tumor. Meanwhile, the increased risk of complications while straight exposing the adrenal central vein should not be neglected. 24 Sometimes, the hemodynamic fluctuations will not completely cease even after perfect ligation of the adrenal central vein because of catecholamine secretion through accessory adrenal veins. 17 A timely pause in operation and administration of a suitable vasoactive agent are essential. Therefore, the best guarantee of success in this operation is an experienced laparoscopic surgeon working with a skilled anesthesiology team. 25
We found that LESS-PHEO required a longer operative time than RLAP-PHEO, which is different from the finding of Hattori et al. The operative time can be affected by many factors. We speculate that the dominant reason for the prolongation of the LESS-PHEO procedure can be attributed to unfamiliarity with the unique devices and special topesthesia of LESS. The inevitable learning curve is the only way to gain expertise in the LESS technique and shorten the operative time, even for the experienced laparoscopic surgeon.
Based on our present study, no higher incidence of intraoperative hemodynamic fluctuation, including hypertension, hypotension, tachycardia, or bradycardia, occurred in the LESS-PHEO group, indicating that LESS-PHEO and RLAP-PHEO have an equivalent effect on hemodynamic stability. The increasing risk of intraoperative hemodynamic fluctuations as a result of the prolonged LESS operative time can be avoided effectively by a full preoperative preparation with vascular volume expansion and intensive intraoperative coordination with the anesthetist.
According to our outcomes, the LESS-PHEO group had a lower median VAPS score and shorter postoperative recovery time (days to resumption of oral intake and ambulation, length of postoperative hospitalization), both of which, to some degree, represent higher postoperative satisfaction. Less skin damage and fewer perforations because of use of a single port may be the most important reason for these favorable outcomes.
The retrospective basis of the evaluation and lack of randomization is the main limiting factor of our study and may engender selection bias. A prospective, randomized, controlled trial would be the optimal design for comparing LESS-PHEO and RLAP-PHEO. In the absence of such a trial, comparative studies with larger case numbers would still have a considerable value.
Conclusions
Although more training and practice are needed to shorten its operative time, LESS-PHEO, as performed by an experienced laparoscopic urologist, is a feasible and safe procedure associated with less postoperative pain and faster recovery.
Footnotes
Disclosure Statement
No competing financial interests exist.