
Abstract
Purpose:
To investigate the clinical significance of R.E.N.A.L. nephrometry scoring system in evaluating the complications after laparoscopic radiofrequency ablation (LRFA) of renal tumors.
Patients and Methods:
We conducted a retrospective review of the records of all patients who underwent LRFA of renal tumors from February 2006 to March 2012 in our institution. Tumors were categorized as low (4–6), moderate (7–9), or high complexity (10–12) according to R.E.N.A.L. nephrometry score (NS), which was determined by analyzing preoperative imaging. Perioperative data were analyzed to determine the presence of complications.
Results:
LRFA was performed on 170 tumors in 170 selected patients with preoperative imaging available. Mean patient age was 55.9 years (range 26 to 81), and mean tumor size was 2.8 cm (range 0.9 to 4.9). Mean NS was 6.6 (range 4 to 12). Of the total tumors, 105 (61.7%) were categorized as low-, 46 (27.1%) as moderate-, and 19 (11.2%) as high-complexity lesions. Overall, there were 21 (12.4%) complications, including 6 (3.6%) grade IIIa and 15 (8.8%) grade I–II complications. There was a significant difference in complication rates among the low- (105 patients, 0%), moderate- (46 patients, 4.3%), and high-complexity (19 patients, 100%) groups, respectively (p<0.05). NS was independently associated with a higher risk of postoperative complications (odds ratio 2.87, 95% CI 1.17–3.04, p=0.02) on multivariate analysis.
Conclusions:
The results of patients undergoing LRFA show that the R.E.N.A.L. NS is independently associated with the occurrence of complications. Therefore, the R.E.N.A.L. nephrometry scoring system is useful in predicting the complication risks of patients who undergo LRFA, and may help with surgical decision making.
Introduction
W
Although RFA has a lower complication compared with LPN or OPN because of its minimally invasive feature, it can still lead to a variety of complications during the procedure. 8 The R.E.N.A.L. nephrometry score (NS) is a validated tool that characterizes renal tumors based on several objective anatomical criteria. 9 This scoring system accounts for tumor size, tumor depth, proximity to the collecting system, tumor positioning in the anterior/posterior plane, and tumor location with regard to polarity. Studies of the R.E.N.A.L. nephrometry system show that tumor scores are associated with surgical outcomes and complications. 10 –12
We have used RFA to treat patients with small localized renal masses by means of laparoscopy in our institution since February 2006. The objective of this study was to predict the complications after LRFA using the R.E.N.A.L. nephrometry scoring system.
Materials and Methods
Patients
This study was approved by the institutional review board of our center. We reviewed the records of all the patients who underwent LRFA between February 2006 and March 2012 at our hospital retrospectively. Patients with significant comorbidity, solitary kidney, bilateral renal tumors, familial genetic syndromes, metastatic disease, multiple tumors, and tumors in unresectable locations (in close proximity to vital abdominal structures) were considered for the treatment of LRFA. Patients who could not tolerate the laparoscopic procedure, had earlier renal surgery or history of any inflammatory conditions of the operative kidney were excluded from the LRFA. 7 Overall, 170 selected patients with a single renal mass each underwent the operation of LRFA by one surgeon.
The R.E.N.A.L. nephrometry scoring system was applied retrospectively to all 170 patients who underwent LRFA. Composite R.E.N.A.L. scores were calculated for all patients with available preoperative computed tomography (CT) or magnetic resonance imaging (MRI). Reviewing of images and performance of scores were done by two independent researchers.
Laparoscopic RFA
Our technique of LRFA has been previously described. 7 General anesthesia was applied in all patients. By means of direct vision or ultrasonography via retroperitoneal approach, the tumor was localized after the fat covering the tumor had been removed. A routine tumor biopsy (TruCore, 22-gauge) was done before all LRFA. After the biopsy, the cool-tip system (Radionics, Burlington, MA) was applied when LRFA began. The radiofrequency generator (Radionics) automatically adjusted the output of maximum energy delivery by monitoring tissue impendence. During the RFA, the temperature of the electrode was maintained at 15°C–20°C with the help of internal cooling with chilled water delivered from a peristaltic pump; however, the tumor tissue was heated to a lethal temperature (>60°C). Triple electrode cluster (17-gauge) and single electrode (17-gauge), the maximal ablation diameter of which was 6 and 3 cm, respectively, were used according to lesion sizes. The RFA probe was inserted to the deepest margin of treatment through the abdominal wall or the laparoscopic trocar guided by an ultrasonic device (BK, Herlev, Denmark). On the request of the manufacturer's recommendations, RFA was carried out for a cycle of 12 minutes per lesion. Extra cycles were given if incomplete ablation was judged by the surgeon based on vision. The lesions appeared brown after being ablated, which differed from the normal pink appearance of untreated lesions and the renal cortex. The electrode was withdrawn from the body after the electrode track had been ablated.
Follow-up
Contrast-enhanced CT is the most effective follow-up method for renal tumors treated by RFA. In our institution, contrast-enhanced CT assessment was made at 7 days, 3 months, 6 months, and every 6 months after RFA sequentially. Patients who had renal insufficiency or contrast agent allergy were followed up using enhanced MRI. The ablation was considered successful when the lesion showed less than 10 HU of contrast medium enhancement on CT or no qualitative evidence of enhancement on enhanced MRI. 13 Any new enhancement (>10 HU) after a nonenhancing scan was defined as recurrence. 14 A serum creatinine measurement with every CT examination was made to each patient, and the GFR was calculated using the modified Modification of Diet in Renal Disease (MDRD) equation 15 :
GFR=175×(serum creatinine)−11.54×(age)−0.203×(0.742 if female)×(1.210 if black)
Statistical analysis
Demographics as well as perioperative and postoperative data were analyzed to determine the presence of complications. The distribution of surgical outcomes and NS categories was compared using the chi-square and Student's t-test, as appropriate. Logistic regression was performed to test the association between NS and complication rates. Receiver operating characteristic (ROC) plots for patients with complications versus those without complications were used to define the detection cutoff or threshold score reflecting optimal sensitivity and specificity. All statistical analyses were performed using SPSS vol. 17.0 (SPSS, Chicago, IL) with a p-value<0.05 considered statistically significant.
Results
A total of 170 patients were treated with LRFA for a single renal mass during this period. Patient demographics and clinical characteristics are listed in Table 1. Of these patients, 117 were men and 53 were women, with a mean age of 55.9 years (SD 14.9). Mean tumor size was 2.8 cm (SD 0.8). Mean body mass index was 27.5 kg/m2 (SD 1.6). There were 72 patients with an American Society of Anesthesiologists (ASA) score below III and 98 patients with an ASA score of III. There were 72 tumors located on the left side and 98 on the right side. Stratified by NS classification, 105 (61.7%), 46 (27.1%), and 19 (11.2%) underwent LRFA for a low-, moderate-, or high-complexity lesion, respectively. No differences were observed with regard to age, gender, ASA score, BMI, tumor sides, GFR (pre- and post-RFA), and duration of follow up between groups. When considering procedural variables, although operative duration, mean hospital stay, and biopsy data were similar regardless of anatomic complexity, both preoperative tumor size and blood loss demonstrated a significant variation (p<0.05) between groups with the highest values observed in complex lesions.
LRFA=laparoscopic radiofrequency ablation; PRFA=percutaneous radiofrequency ablation; ASA=American Society of Anesthesiologists; BMI=body mass index; GFR=glomerular filtration rate; MDRD=Modification of Diet in Renal Disease.
The postoperative complications that were classified according to the modified Clavien system were evaluated. 16 Overall, 21 (12.4%) complications occurred in the patients undergoing LRFA, including 15 (8.8%) grade I–II complications (Grade I: 10; Grade II: 5) and 6 (3.6%) grade IIIa complications. Classification and details are listed in Tables 2A and 2B. There was a significant difference in the observed complication rates among the low- (0%), moderate- (4.3%), and high-complexity (100%) groups (p<0.05). Multivariate logistic regression showed that NS was independently associated with a higher risk of postoperative complications (odds ratio [OR] 2.87, 95% CI 1.17–3.04, p=0.02, Table 3A). When analyzing the individual components of the R.E.N.A.L. NS in multivariate logistic regression, we found that the only component significant was the “N” nearness to the collecting system, and tumor <4 mm from the collecting system was significantly associated with postoperative complications (OR 5.76, p=0.03, Table 3B). All patients with an NS of more than nine had a complication, and patients with a score of less than 8 did not have any complications.
NS=nephrometry score.
OR=odds ratio.
The ROC plots for patients with complications versus those without complications were used to define the detection cutoff or threshold score reflecting the optimal sensitivity and specificity (Fig. 1). The area under curve (AUC) of NS was 0.944, and the AUC of tumor size was 0.578; thus, the accuracy of NS in predicting complications was significantly superior to that of tumor size (p=0.001). When Youden index of ROC curve reached the maximum, we got the threshold NS of 9, which reflected the optimal sensitivity and specificity. A composite R.E.N.A.L. score of 9 yielded a sensitivity of 87.5%, a specificity of 100%, and a diagnostic accuracy of 98.2%. Thus, patients undergoing LRFA with R.E.N.A.L. scores greater than 9 were most likely to have surgical complications compared to those with scores less than 9.
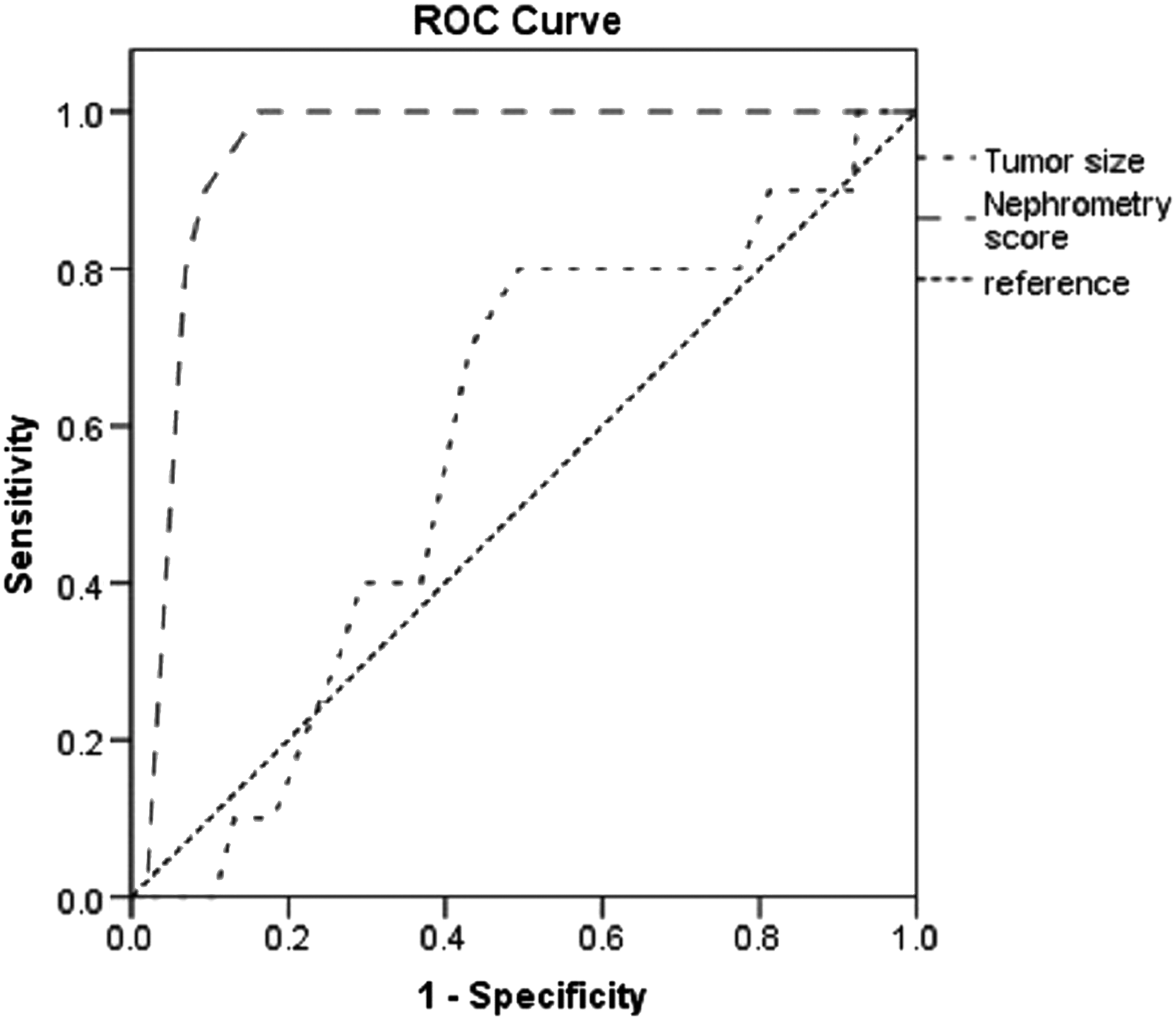
Receiver operating characteristic (ROC) curve of R.E.N.A.L. nephrometry score and tumor size.
Comment
The RFA has been successfully applied in the treatment of liver, bone, and breast tumors. 17 –19 PN is regarded as the gold standard treatment for SRMs, and RFA is considered an option for patients with high surgical risk. 20,21 More and more recent literature reported long-term oncologic outcomes for those that mirror extirpative surgery. 7,22
The RFA can be applied by various means: open, laparoscopic, and percutaneous approaches. Open RFA is seldom used nowadays. Although percutaneous RFA is preferred in literature, the laparoscopic approach enables aggressive mobilization of renal tumors and placement of the probe under direct vision, and the laparoscopic approach makes access to anteriorly based tumors possible, which may be difficult in the percutaneous approach. Besides, hemostasis can be obtained directly via the LRFA approach. 23 Yang et al. 24 performed a retrospective review of 51 patients with unilateral T1b renal tumors who underwent laparoscopic RFA with a mean follow up of 31.5 months. They concluded that their initial experience with intraoperative contrast-enhanced ultrasonography in T1b renal tumors was favorable with good renal function preservation and oncologic outcomes. Although RFA is a safe technique, it can still bring about certain complications during the operation. There may be additional complications seen with the laparoscopic technique itself. It is important to have experience with laparoscopy procedures for preventing and managing these complications. 25 In the present study, 21 patients out of 170 had complications, and the overall complication rate of LRFA was 12.4%. Bensalah et al. 26 reported their outcomes of 38 patients who were treated for a renal tumor by LRFA. Their overall complication rate was 7.9%, including one ureteric stricture requiring a nephrectomy for a nonfunctioning kidney at 1 year, an isolated hydrocalyx, and persistent pain at the puncture site. Their results were approximately the same in accordance with ours.
Bruner et al. 12 explored the relationship between anatomic complexity and urine leak in patients undergoing PN from a matched cohort analysis. They drew the conclusion that the risk of postoperative urine leak increased by 35% with each unit increase in total NS. White et al. 27 applied R.E.N.A.L. NS in evaluating the safety and feasibility of robotic PN for patients with complex renal masses, and they reached the conclusion that the warm ischemia time, blood loss, and complications were increased with highly complex masses. However, the R.E.N.A.L. NS system has not been evaluated in patients undergoing LRFA.
It is helpful in relating anatomic complexity to surgical outcome using a standardized methodology for preoperative counseling, and it enables patients to make clinical trade-off decisions confidently. In our series, there was a significant relationship between anatomical complexity and postoperative complications. Further multivariate analysis showed that increasing “N” nearness to the collecting system was significantly correlated with postoperative complications. All patients with NS of 9 or greater had a complication and had a higher risk of postoperative complications. Our results suggest that appropriate counseling and care should be taken when applying LRFA in highly complex tumors. These findings are consistent with previous studies that described the increased risk of specific complications after PN for complex tumors. A report by Rosevear et al. 10 showed that surgeon operative preference and risk of complications for patients undergoing PN were accurately revealed by the R.E.N.A.L. system, and it was more likely for patients with higher scores to undergo RN than PN. Satasivam et al. 28 reported that significantly larger lesions of predominantly moderate and high complexity were performed with RN, and nephron-sparing surgery was mainly applied in low-complexity lesions in their study. Sisul et al. 29 suggested that the post-procedure complications after renal cryotherapy developed with an increase in the R.E.N.A.L. score. Therefore, a threshold NS should be established so that the benefit of patients who undergo LRFA can be guaranteed. We suggest that the cutoff should be a score of 9 according to our results and ROC analysis. Sisul et al. 29 demonstrated that the score of “N”nearness was correlated with postoperative complications of cryoablation of renal masses independently, which could also be concluded from our research.
Admittedly, several limitations were involved in our study, with the retrospective analyses and lack of comparative outcomes of percutaneous RFA included. We did not bring anterior or posterior and hilar location into consideration during analyzing the postoperative complications. Simultaneously, the sample size of our study was relatively small, as with most other retrospective analyses, there was inherent bias, including selecting bias.
Conclusion
The LRFA is a safe and effective choice for patients with SRMs. The R.E.N.A.L. nephrometry scoring system is useful in predicting the complication risks of patients undergoing LRFA. Higher NS are significantly associated with major complications during this procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.