
Abstract
Objective:
To assess if the presence of a lower pole stone (LPS) decreases the stone-free (SF) rate following retrograde intrarenal surgery (RIRS). The second purpose was to assess the result of RIRS for LPS and to identify predictors of SF status.
Patients and Methods:
We retrospectively analyzed 205 procedures in 162 patients with renal stones treated by RIRS between January 2010 and January 2013 at a single institute. The SF status was defined as no residual fragments. Independent-sample t-tests and Chi-square tests were used for comparisons of means and proportions, respectively, between patients with or without LPS. Logistic regression models were used to assess prognostic factors influencing SF status in cases of LPS.
Results:
LPS were present in 89 (54.9%) patients. There were no differences between patients with or without LPS regarding the mean operative time (p=0.77), the surgeon's experience (p=0.522), the length of hospital stay (p=0.269), and the SF rate (p=0.224). SF status after RIRS in patients with or without LPS was 74.1% and 78% (p=0.224), respectively. In the case of LPS, the presence of multiple stones and a history of percutaneous nephrolithotomy (PCNL) were predictive factors for occurrence of residual fragments in univariate analysis (p=0.037 and p=0.015). In multivariable analysis, only the presence of multiple stones remained as a predictive factor (p=0.027; HR=3.2), whereas a trend was observed when there was a history of PCNL (p=0.07; HR=3).
Conclusion:
The presence of a LPS does not alter the SF rate of RIRS even in cases of early experience. RIRS for LPS appears to be an effective technique, but special attention should be given to patients with multiple stones and/or a history of PCNL.
Introduction
R
The first objective of this study was to assess if the presence of a LPS decreases the SF rate after f-URS for intrarenal stones. The second purpose of the study was to assess the result of RIRS for LPS and to identify predictors of SF status.
Patients and Methods
We retrospectively analyzed 205 procedures in 162 patients treated by f-URS for intrarenal stones between January 2010 and January 2013 at the Angers University Hospital. All patients with unique radio-opaque stones were previously treated by at least one procedure of ESWL without results. Patients were preoperatively evaluated by computed tomography. A urine culture was performed on each patient before surgery. Patients with urinary infection or bacteriuria confirmed by the urine cultures were treated for at least 5 days with adapted antibiotherapy. The cases were performed by 10 different surgeons from the same institution. The surgeon's experience was assessed according to the number of procedures performed (experienced ≥50; intermediate ≥25; novice <25).
All procedures were done with the patient under general anesthesia in a standard lithotomy position. A 0.035-inch polytetrafluoroethylene coated guide wire was placed in the upper urinary tract through a rigid cystoscope under fluoroscopic guidance. A safety wire was routinely inserted. A ureteral access sheath (exor Ureteral Access Sheath With AQ; Cook Medical, Spencer, IN) insertion was made on an individual basis and was not prospectively specified among surgeons. The flexible ureteroscope (Flex-X2 TM; Karl Storz Endoscopy, Tuttlingen, Germany) was passed into the upper urinary tract in a monorail fashion over the second wire. A holmium-YAG laser was used at an energy setting of 0.6–0.8 J and a rate of 8–10 Hz. A 270- or 400-μm laser fiber was used for delivering laser energy to the stones. Basically, stones were fragmented in situ until it was possible to move them by using a basket (Holmium Lightguide; Dornier Medtech, Wessling, Germany) to an upper pole calyx. If the length of the operation exceeded 120 minutes, the procedures were stopped to reduce the occurrence of perioperative complications. At the end of the procedure, the whole collecting system was inspected for residual stones and a double pigtail ureteric stent or a ureteral stent was left for 3–4 weeks or 1 day, respectively, before being removed.
We recorded patient age, gender, body mass index, number of stones, stone localizations, diameter of the most important stone (cm), cumulative stone diameter (cm), stone compositions, and history of previous PCNL on the same kidney. The perioperative factors analyzed included the duration of operation (minutes), surgeon experience, use of ureteral access sheath, diameter of fiber, placement of the ureteral stent or double pigtail ureteric stent, complications, and length of hospital stay.
The SF status was defined as no residual fragments either after basket extraction without lithotripsy of a unique stone or 1–2 months after the last f-URS session by noncontrast computer tomodensitometry. Another procedure was performed in cases where the diameter of the residual largest stone was superior to 5 mm or in cases of symptomatic stones.
Independent-sample t-tests and Chi-square tests were used for comparisons of means and proportions, respectively, between patients with or without LPS. Univariate and multivariate regression models were used to assess prognostic factors influencing the SF rate in cases of LPS. p<0.05 was considered statistically significant. Only factors that were significant in univariate analysis were considered for multivariate analysis. All tests were done using the SPSS® software package (SPSS, Chicago, IL).
Results
Patient and stone characteristics
Between January 2010 and January 2013, 162 patients presenting with renal calculi and treated with f-URS were included. LPS were present in 89 (54.9%) patients. Patients with LPS had more multiple stones (p=0.003), less preoperative ESWL (p=0.01), more diagnosis by following urolithiasis (p=0.006), less diagnosis by chronic urinary infection (p=0.039), and fewer preoperative stents (p=0.018) than patients with nonlower pole calculi. A comparison of patient and stone characteristics between cases with or without LPS is described in Table 1.
BMI=body mass index; ESWL=extracorporeal shockwave lithotripsy; PCNL=percutaneous nephrolithotomy.
Perioperative data
Patients were treated by one procedure, two procedures, or more than two procedures in 143 (88.2%), 14 (8.6%), and 5 (3.1%) cases, respectively. After one or multiple RIRS, 110 (67.9%) and 123 (75.9%) patients were SF, respectively. Stones were inaccessible in 7 (7.8%) and 2 (2.7%) cases, for patients with or without LPS (p=0.204), respectively. Perioperative complications occurred in 16 (9.8%) patients (5 pyelonephritis, 3 macroscopic hematuria, 6 pains with the necessity of grade II analgesia, and 1 urinoma). There were no differences between patients with or without LPS regarding the mean operative time (p=0.77), the surgeon's experience (p=0.522), the length of hospital stay (p=0.269), and the SF rate (p=0.224). Comparisons of perioperative data between cases with or without LPS are described in Table 2.
SF=stone free.
Predictive factors of SF rates in cases of lower pole calculi
In the case of LPS, 55 (61.8%) and 67 (75.3%) patients were SF after one or multiple RIRS, respectively. The presence of multiple stones and a history of PCNL were predictive factors for occurrence of residual fragments in univariate analysis (p=0.037 and p=0.015). In multivariable analysis, only the presence of multiple stones remained as a predictive factor (p=0.027; HR=3.2), whereas a trend was observed for a history of PCNL (p=0.07; HR=3). Univariable and multivariable Cox regression analysis assessing the association between predictor variables and SF rate in cases of LPS are described in Table 3.
CI=confidence interval; PCNL=percutaneous nephrolithotomy; BMI=body mass index.
Cases with unique lower pole calculi
A unique lower pole calculus was present in 60 patients with a mean diameter of 11.7±4.3 cm. In those cases, the mean operative time was 87.4±32.2 minutes. About 44 (73.3%), 13 (21.7%), and 3 (5%) patients had one, two, or three procedures, respectively. At the end of the follow-up, 50 (83.3%) patients were SF.
Results in cases of LPS regarding the number of procedures and calculi are summarized in Figure 1.
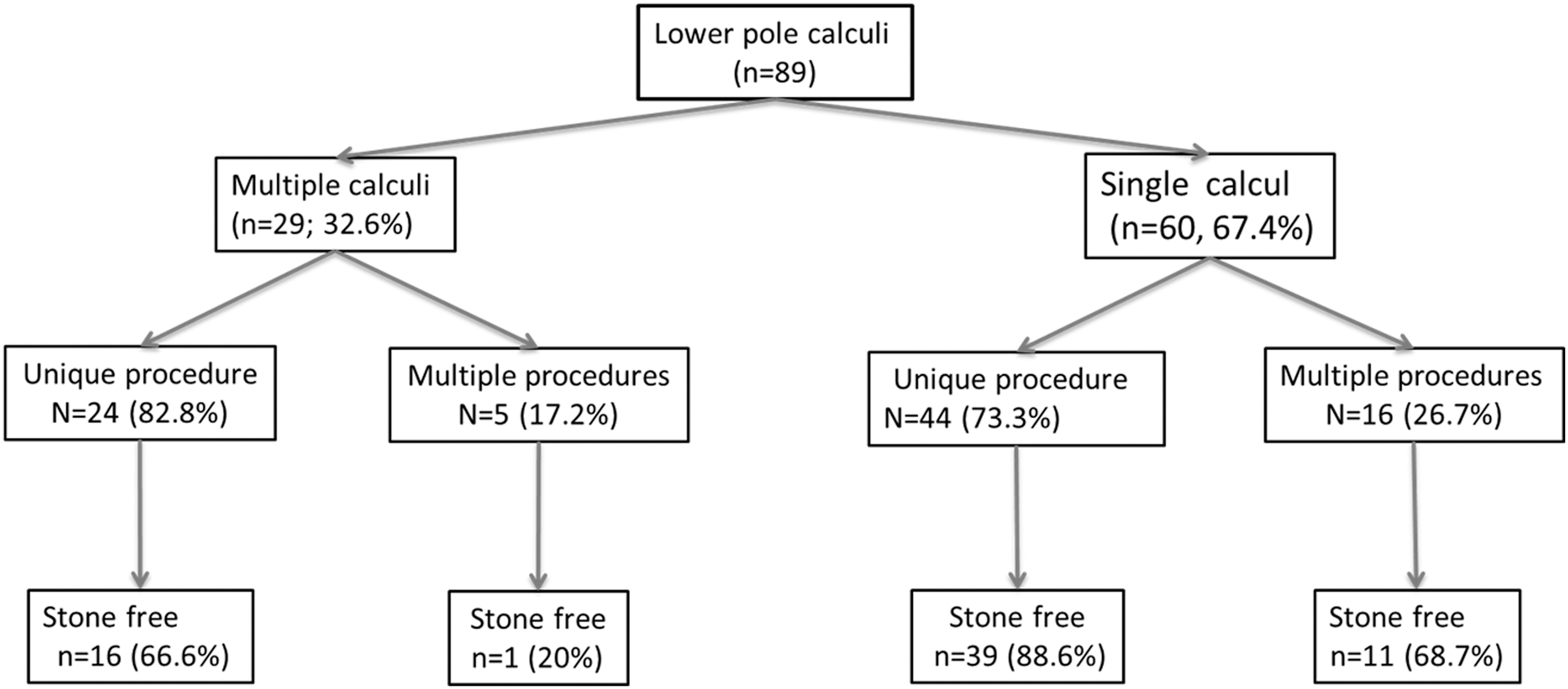
Results in cases of lower pole stones regarding the number of procedures and calculi.
Discussion
The use of the flexible ureteroscope and the improvement of working instruments, such as the holmium:YAG laser or tipless nitinol baskets, have enhanced the ability to successfully treat LPS by RIRS. 12,13 This study supports the finding that the presence of LPS does not modify the success rate of RIRS even in case of early experience.
To our knowledge, only Ito et al. have identified LPS as a predictive factor of stone persistence after RIRS. However, this association was found only in univariate analysis and groups with or without LPS were not described. 14 On the other hand, Perlmutter et al. have evaluated the impact of the stone localization on 86 kidney stones treated by RIRS and found that the stone location does not significantly affect the stone clearance rate. However, the mean size of the stones, surgeon skill level, and operative time were not detailed with regard to stone localization. 10 In our study, patients with LPS had more multiple stones, more diagnosis by following urolithiasis, less diagnosis by chronic urinary infection, less preoperative ESWL, and fewer preoperative stents than patients with nonlower pole calculi. However, the groups were comparable in terms of surgeon experience and stone sizes. Moreover, LPS were not associated with a lower SF rate, higher operative time, longer hospital stay, or postoperative complications. Indeed, the presence of a LPS does not seem to be associated with indirect factors of operating difficulties.
Initially, SWL constituted the recommended therapy for patients with small to moderate sized LPS. However, the SF rate after SWL for LPS is reported to be between 25% and 85%. 8,15,16 Therefore, with regard to the poor efficacy of SWL on LPS, endourological procedures are currently recommended as the first line of treatment by the EAU guidelines for LPS between 10 and 20 mm in case of negative predictors for SWL (steep infundibular-pelvic angle, long calyx, or narrow infundibulum). 17 Indeed, PCNL has proven to be highly successful for the management of LPS. 6,17 –19 In the first Lower Pole Study, the SF rates after PCNL were 100%, 93%, and 86% for LPS smaller than 1, 1–2, and larger than 2 cm, respectively. However, PCNL was associated with greater morbidity than SWL. 19 Although with regard to its morbidity, PCNL is controversial especially in cases of small LPS where active monitoring could also be a therapeutic option. 20 On the other hand, concerning stones between 2 and 3 cm, Hyams and Shah demonstrated that the estimated cost of PCNL was significantly greater than RIRS. 21 In this context, RIRS could be the preferential endourological procedure of a LPS. Several studies have already reported a significantly higher SF rate and a lower retreatment rate for RIRS compared with ESWL for LPS. 7 –9 In the same way, comparable results between RIRS and PCNL for the treatment of lower caliceal stones were reported. 6 In their multicenter prospective study, Pearle et al. reported a SFR for LPS of 50% after one procedure. 7 Our higher success rate could confirm the improvement of material quality and technique over the last 10 years. However, we report a SF rate in the lower range of the other retrospective published series. For example, Hollenbeck et al. found a SF rate for the treatment of inferior caliceal stones of 79% after the first RIRS and 88% after two procedures. 4 Our results can be explained, in part, by the fact that we chose to include all patients treated during this period independently of the size and/or the number of stones. Another possible reason for our SF rate could be the definition and the means used to determine the SF status. In this study, we used a noninjected computer tomodensitometry for all patients who had a holmium laser lithotripsy and have considered the absence of residual fragments to establish patients in the SF group. In fact, it is possible that direct visual assessment, assessment by ultrasound, or standard X-ray, which are used in other studies, could lead to an underestimation of residual stones. 3 –9
In case of LPS, we have identified the presence of multiple stones as a risk factor for stone persistence after ureteroscopy in univariate and multivariate analyses. Personal history of PCNL was also associated with residual fragments in univariate analysis. One of the possible explanations is that lower calyx access is normally used preferentially during PCNL. This calyx puncture could conduct to some anatomical modifications like scares or calyx distension, which could complicate access to the stone. In our series, of the seven patients with nonaccessible LPS, three had a previous PCNL. A specific study in this population of patients with a history of PCNL could be conducted to confirm these results and to establish the potential anatomical calices changes after PCNL. Finally, in contrary to what we might have thought, the experience of the surgeon does not affect the SF rate of RIRS for lower pole calculi. However, in our department, physicians with limited experience were shadowed by an experienced surgeon during the procedure.
There are several limitations to this study. This is a retrospective review from a single institution. The results are based on a relatively small sample size and we decided not to perform a matched study to conserve all the patients. However, this is the initial experience by a single institution with multiple surgeons. We think that the uniformity of the material and the procedures allowed us to obtain homogeneous results. Finally, with the decreasing size of ureteroscopes and the improvement of the technique, we believe that the lower pole localization does not modify the successful treatment of intrarenal lithiasis with RIRS.
Conclusion
The presence of LPS does not alter the SF rate of RIRS even in cases of early experiences. For patients with LPS, the SF rates were 67.9% and 75.9% after one or multiple RIRS, respectively. Finally, RIRS for LPS appears to be an effective technique, but special attention should be given to patients with multiple stones and/or a history of PCNL.
Footnotes
Acknowledgment
The authors thank Timothy Myers for proofreading the manuscript.
Disclosure Statement
No competing financial interests exist.