
Abstract
Objectives:
Given the high recurrence rate of cystine urolithiasis, understanding of the radiographic stone characteristics is important in following cystine stone formers over their lifetime. However, due to their infrequent incidence, in vivo radiographic properties of cystine stones have not been well characterized. The purpose of our study is to characterize the in vivo radiographic properties of cystine urolithiasis.
Methods:
Patients with a cystine stone analysis and noncontrast computed tomography (NCCT) were extracted from our stone clinic database. Stone attenuation in Hounsfield units (HU) was measured for each stone and plain abdominal films (kidney, ureter, and bladder radiograph [KUB]) within 30 days of the NCCT prior to any intervention were reviewed by a blinded radiologist to assess whether urolithiasis could be visualized.
Results:
Twenty patients met our study inclusion criteria. When plotted by attenuation, two distinct groups of stone attenuation were noted for cystine stone formers (p<0.001). The largest group (n=16) had an attenuation of <550 HU (424±106 HU), while a distinct second group (n=4) was >850 HU (972±134 HU). Sixteen patients had a KUB, with 88% of the stones being visualized by a blinded radiologist. Stone size and attenuation were not significantly different between visualized and nonvisualized stones via KUB, however, the body mass index was significantly higher in the nonvisualized group (34.4 vs 26.9 kg/m2, p=0.03).
Conclusions:
Cystine stones were visualized by KUB, which has implications in post-treatment follow-up imaging. Though most cystine stones had an attenuation of <550 HU, a second distinct group of cystine stones were noted to have a high attenuation of >850 HU. HU measurements alone are not sufficient to differentiate cystine stones from other stone compositions.
Introduction
C
Cystine calculi have long been considered resistant to shockwave lithotripsy (SWL). 4,5 However, in vitro studies have suggested that cystine calculi exhibit two different morphologies, “smooth” and “rough.” 6,7 Rough cystine stones are darker calculi with large, block crystals at the surface. The rough morphology has been shown to be more fragile than the smooth stones. 7 Kim et al. demonstrated rough cystine stones to possess void regions within them, making them heterogeneous and thus distinctive from their smooth, homogenous counterparts by helical noncontrast computed tomography (NCCT). 8 Their in vitro study of cystine stones showed that lower average stone attenuation required less shockwaves for comminution than did the higher attenuation calculi. 9 Given that in vitro studies were performed with smaller computed tomography (CT) collimation and are less likely to have volume partial averaging, in vivo studies examining the radiographic characteristics of cystine stones are needed. The purpose of our study was to characterize the in vivo radiographic properties of cystine urolithiasis by NCCT and kidney, ureter, and bladder radiograph (KUB).
Materials and Methods
Our retrospective study was approved by the institutional review board. All cystine stone formers were extracted from our metabolic stone clinic database. Patient demographic data was obtained from electronic medical records. Patients with a documented cystine stone analysis and an NCCT were included in the study. NCCT were performed using GE LightSpeed series multidetector CT scanners (120 kVp, variable mA, 5 mm image reconstruction at 3 mm intervals; GE Healthcare, Madison, WI). Magnified bone window settings were used to visualize all stones in the study on NCCT scan. The transverse diameter of the stone on each slice was measured in millimeters on a CT workstation. Slices containing the two largest transverse diameters of the stone were then identified. The mean attenuation value for each stone was calculated from two nonoverlapping regions of interest (ROI) for each stone. Stone attenuation in Hounsfield units (HU) was calculated using the average of two ROI for each stone. 10 The largest diameter in any dimension was recorded as maximal stone size. All calculi were either passed spontaneously or retrieved after endoscopic intervention. Stone analysis was performed via X-ray diffraction and Fourier transform infrared spectroscopy. All of the cystine stones recovered had no calcium component on analysis.
Plain abdominal films (KUB) within 30 days of the CT prior to any intervention were also examined. A single, blinded radiologist (M.G.L.), unaware of the corresponding CT scan, reviewed all KUB's to determine whether urolithiasis could be visualized.
Descriptive statistics including mean and standard deviation for HU attenuation were calculated. Unpaired t-test was used to perform comparisons of the mean HU, stone size, and body mass index (BMI) between the two different cystine groups and between visualized and nonvisualized cystine stones on KUB. The level of significance was set at p<0.05.
Results
Of the 28 cystine stone formers seen in our metabolic stone clinic, 20 had a NCCT performed at our institution. Fifteen of the cystine stone formers were female and five were male. Mean age of patient was 46.9 years (range 22–69 years). Mean BMI was 28.6±4.7 kg/m2 (Range: 21.5–46.2 kg/m2).
The mean stone size was 11.1±4.7 mm (Range: 5.1–21.3 mm). Stone attenuation ranged from 235 to 1101 HU. Overall mean stone attenuation was 532±250 HU. When plotted by attenuation (Fig. 1), two distinct groups of stone attenuation were noted (p<0.001). The largest group (n=16) had a stone attenuation of <550 HU, with a mean attenuation of 424±106 HU. The second group had a significantly higher stone attenuation of >850 HU, (n=4) with a mean attenuation of 972±134 HU. There was no significant difference in stone size between the <550 HU and >850 HU groups (11.4±5.1 vs 11.7±2.8 mm, p=0.84).
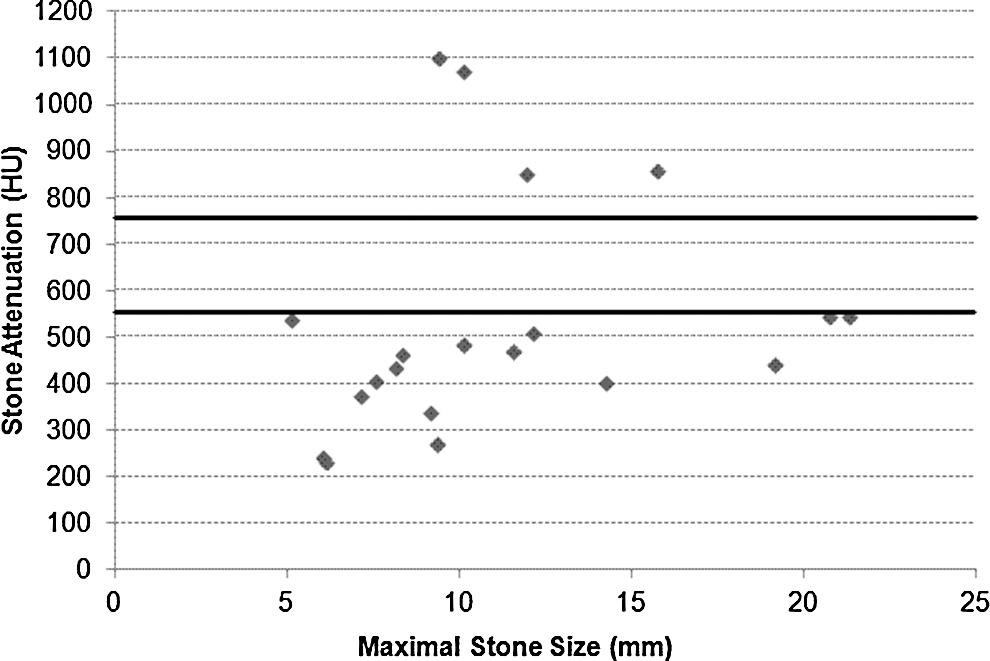
Cystine Stone Attenuation on NCCT (HU) plotted against Maximal Stone Size (mm). The largest group had an attenuation of <550 HU, while a distinct second group was >850 HU (solid horizontal lines).
Sixteen patients had a KUB within 30 days of their noncontrast CT scan. With a single, blinded radiologist reviewing each KUB, 88% (14/16) of the stones were visualized. There was no significant difference in the stone size between the visualized and nonvisualized stones (11.0 vs 15.3 mm, p=0.28). Similarly, there was no significant difference in stone attenuation (554±255 HU vs 357±116 HU, p=0.30). However, the nonvisualized group had a significantly higher average BMI (34.4±1.8 kg/m2) than the visualized group (26.9±4.1 kg/m2) (p=0.03). The presence of the stone on KUB was not related to the HU attenuation of the stone. There was not a statistically significant difference in the HU attenuation between those stone seen on KUB versus those not seen on KUB (550.9±272.0 vs 455.7±123.2, p=0.51).
Discussion
NCCT is the standard imaging modality for patients with urolithiasis. 11 As CT has evolved, attenuation on NCCT, as measured in HU, has been used to differentiate stone composition in both in vitro and in vivo studies. 12 –17 HU measurement on NCCT has also been used to provide insight into stone fragility and SWL success. 18,19
The low incidence of cystine stones have led to a dearth of in vivo studies regarding their radiographic characteristics (Table 1). Several in vitro studies have examined cystine stone attenuation in various media, with mean attenuation ranging from 540–711 HU. 16,20 –22 Hassani et al. compared 12 cystine stones to 24 uric acid stones and found a statistically significant difference in mean HU of cystine versus uric acid stones in an in vitro study. 22 Despite the mean HU for uric acid stones at 505±128 HU (Range: 208–760) being lower than the mean HU for the cystine stones at 783±163 HU (Range: 360–960), there was a significant overlap in the range of HU attenuation between both stone compositions. Mostafavi et al. performed an in vitro study comparing HU attenuation via NCCT at 120 kV versus a dual energy CT. 16 They found the mean HU of 14 cystine stones to be 711±228, which could not be accurately distinguished from struvite stones (666±87 HU). However, dual energy CT did allow cystine stones to be distinguished from struvite, uric acid, and calcium oxalate stones. Though dual energy CT has been shown in the literature to accurately differentiate between various stone compositions, they are generally not found in most hospitals or used in an acute care setting, such as the emergency room, and would thus would not be utilized in the general clinical setting. 16 While in vitro studies have been able to distinguish cystine stones from other stone compositions, the results may not be applicable to in vivo situations. To reduce noise and improve accuracy of HU measurement, most NCCT protocols for in vitro stones are frequently performed at a higher voltage. Further, smaller NCCT collimation is used in many in vitro studies than is normally used in the clinical setting, to reduce partial volume averaging. The higher voltage and smaller collimation generally do not reflect the scanning parameters used in a clinical setting and is contrary to the current clinical ideology of reducing patient radiation exposure.
HU=Hounsfield units.
Characterizing cystine stone attenuation from previous patient NCCT scans provides more clinically relevant data. In our in vivo study, overall mean stone attenuation was 532±250 HU, with a range of 235–1101 HU. Two distinct groups of stone attenuation were noted, <550 HU and >850 HU (p<0.001). This finding is important that it shows that there is a significant overlap in HU attenuation between cystine stones and uric acid stones (overlap with the <550 HU group) or calcium stones (overlap with >850 HU group) depending on the cystine stone group. Kim et al., in an in vitro study, demonstrated cystine stones with lower attenuation required a reduced number of shockwaves for comminution. 9 Our finding suggests that a number of cystine stones have a lower attenuation, and thus NCCT may lend itself to the evaluation of cystine calculi for treatment with SWL. However, further in vivo studies are needed to determine clinical SWL feasibility within the lower HU group, as Kim et al. 2007 used smaller stones (4–7 mm) than the stones in our current study (5–21 mm). 9 Additionally, in vitro stones are not surrounded by soft tissue that may reduce shockwave efficacy.
Our study shows that cystine stones are well visualized by KUB. Even stones in the <550 HU group, which would be similar stone attenuation to uric acid calculi that can be radiolucent on KUB, were easily visualized. The reason why cystine stones with HU <550 are visible by KUB but not UA stones is likely related to the density of the sulfur atoms. 24 The visualization of cystine stones on KUB carries implications for post-treatment follow up of cystine stone formers. The effective radiation dose (mSv) for a renal ultrasound, KUB, and CT-scan of the abdomen and pelvis are 0, 1.7, and 20 mSv respectively. 25 Given that cystine stones can be visualized by KUB, we would recommend using KUB or renal ultrasound (US) for surveillance. CT is still a useful imaging modality, especially at initial diagnosis, given its high diagnostic sensitivity and specificity and its accuracy in assessing stone burden. However, due to its significantly higher effective radiation dose compared with KUB and renal US, it must be used judiciously. Thus, KUB offers a cost-effective imaging modality with reduced radiation exposure to a population of patients who are frequently imaged given their rate of stone formation. In our study, stone size and attenuation did not affect the radiologist's ability to visualize the stone. However, elevated BMI was associated with difficulty in visualizing cystine stones.
Limitations of our study include the retrospective nature of our study. Though a blinded radiologist was able to detect 16 of the 20 stones on KUB, the current study is not designed to accurately describe the positive and negative predictive value of KUB for the detection of cystine stones. Though the number of cystine stones in our study would be considered small in comparison to other stone compositions, our study is the largest in vivo study describing the radiographic characteristics of cystine urolithiasis to date.
Conclusion
An understanding of the radiographic characteristics of cystine urolithiasis is important due to the high recurrence rate of cystine stones and to aid in future follow-up. Most cystine stones were visible on KUB, which should reduce radiation exposure and cost of post-treatment imaging. In our study, most cystine stones had an attenuation of <550 HU, yet a second distinct group of cystine stones were noted to have a high attenuation of >850 HU. The large range on HU attenuation leads to overlap when comparing cystine stones to the attenuation of other stone compositions and thus makes it difficult to diagnosis cystine urolithiasis solely based on HU attenuation. Further studies are needed to explore in vivo stone fragility of cystine stones with attenuation <550 HU.
Footnotes
Disclosure Statement
No competing financial interests exist.