
Abstract
Purpose:
To evaluate the different anatomical properties and determine the risk of visceral organ injury in supine, prone, and prone-flex positions.
Materials and Methods:
A total of 30 patients with renal stones >2 cm were included. A dose reduced abdominopelvic tomography in a supine, prone, and 30° prone-flex position was performed. The access tract length, subcutaneous tissue length, nearest organ distance, maximum access angle, access field, and the degree of renal displacement were measured in axial and coronal images. The parameters were analyzed by the paired t-test and Wilcoxon signed test according to normalcy analysis.
Results:
The mean tract lengths and the subcutaneous fat tissue lengths in the lower, middle, and upper poles of kidney were significantly longer in the supine position. The significance of access tract lengths had disappeared when we subtracted the subcutaneous fat tissue length from the whole tract length, exhibiting that the main determinant of tract length was subcutaneous tissue thickness. The maximum access angles were 96.7±22.0°, 94.2±23.6°, and 89.1±23.9° in the supine, prone, and prone-flex position, respectively (p>0.05). The access field was shorter in the supine (80.8±13.3 mm) than prone (86.3±15.0 mm) and prone-flex (86.7±18.4 mm) position (p<0.001). The nearest organ distance to access tract was similar between the supine and prone position in every pole of kidney.
Conclusions:
The anatomical changes related to supine positioning does not increase the risk of percutaneous nephrolithotomy (PCNL) complications. Although supine PCNL may have some benefits over prone PCNL, there will also be some technical difficulties related to the surgeon's manipulations, which are related with the longer access tract and more limited access field.
Introduction
F
As its safety was documented in several studies, PCNL has been performed in a prone position for several years. This position was supposed to provide a larger area for renal access and a wider space for instrumentation and was proved to be safe for the risk of splanchnic injury. On the other hand, prone positioning had also some disadvantages, including positional discomfort, possible ocular, spinal, or peripheral nerve injuries, as well as ventilation and circulation problems especially in morbidly obese patients. 3,4 Repositioning the patients after ureteral catheterization was also a challenging and time consuming issue for prone PCNL.
To overcome these possible problems and simplify the surgery, Valdivia et al. described the supine PCNL technique in 1998. 5 Possible risks related to the prone position seemed to be decreased with the supine position and the surgeons were able to perform retrograde ureteral manipulations during surgery. Nevertheless, the supine position leads to a more lateral displacement of the renal access site that may compromise the safety with possible related organ injury and significant vessel trauma. Proponents of supine position claimed that, displacement of colon posteriorly might increase the risk of colon perforation. Although the colon perforation rate was less than 1% in supine PCNL series, majority of urologists still have the fear of this undesired complication. 3
Whether there are numerous well-documented advantages of supine PCNL, the prone position has still been the preferred technique for many urologists. This may be related to lack of scientific data, the surgeon's habitual practice, or the fear of organ injury. To resolve these prejudgments and understand for possible complications, urologists must be aware of anatomical variations related to the supine position. In this study, we aimed to evaluate the different variables of anatomical properties in the supine, prone, and prone-flex positions and determine the risk of visceral organ injury.
Materials and Methods
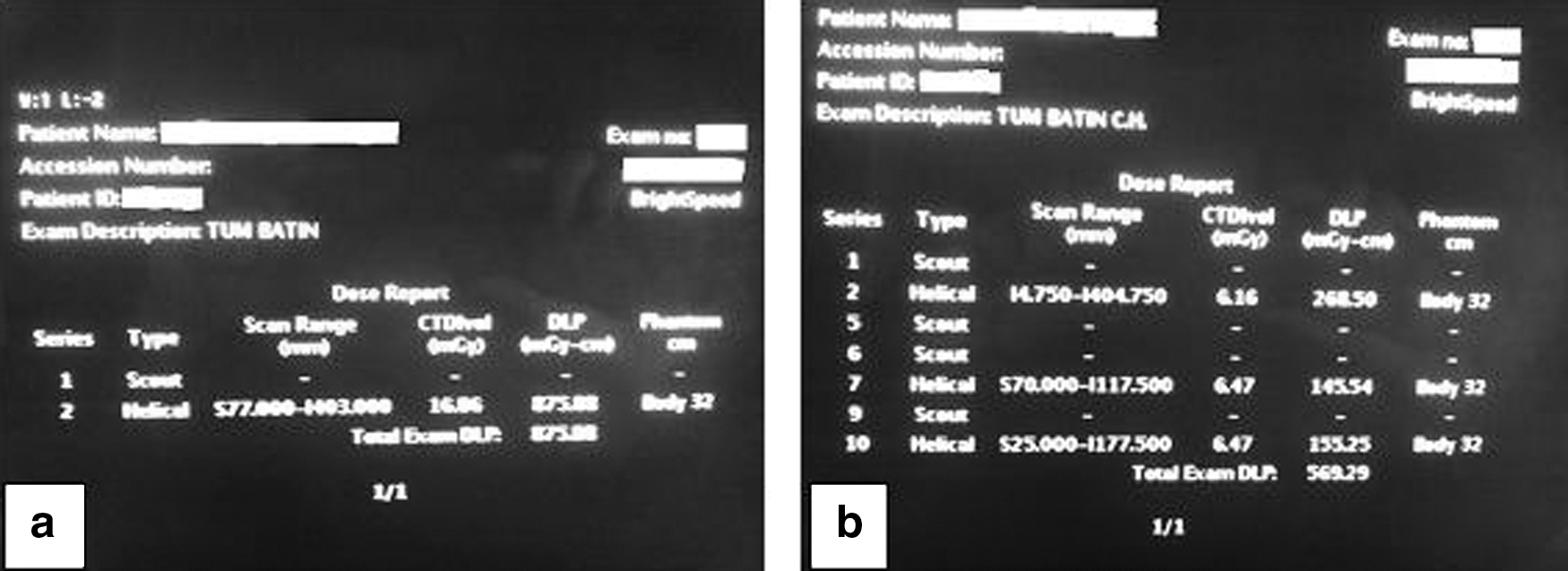
This prospective study was approved by our institutional review board and a written informed consent was obtained from all patients. We enrolled a total of 30 patients with >2 cm calyseal or renal pelvis stones with a decision of PCNL. In our clinic, a standard noncontrast supine abdominopelvic computed tomography (APCT) is a routine procedure before PCNL. Distinctly to our standard procedure, noncontrast APCTs in prone and prone-flex positions were also obtained. A 30° prone-flex position was given to patients by placing a standard surgical pillow at the level of umbilicus. To spare the patients from extra radiation, the radiologist performed a low-dose CT protocol with high quality images with a 16-slice CT scanner (LightSpeed-16; General Electric [GE]). With this protocol, we were able to perform three CT imaging with a radiation dose much lower than a standard APCT evaluation. The mean total radiation dose was 543.26±36.32 Gy, which was ∼60% of a standard APCT (Fig. 1).
The access tract length, subcutaneous tissue length, nearest organ distance to access tract, maximum access angle, access field, renal hilum distance to midaxial line, and lateral kidney distance to midaxial line were measured in axial and coronal images. The access tract length and the subcutaneous tissue length were measured in lower, middle, and upper calyces of kidney. As contrast material was not injected due to ethical issues, the calyceal system was depicted by obtaining multiplanar images in the axial, coronal, and sagittal planes. A constant localization was marked at the papilla of posteroinferior, middle posterior, and upper posterior calyces and these markers were used for the measurement of access tract. On the same access line, we measured the distance from the skin to the outer surface of external oblique muscle for the evaluation of subcutaneous tissue distance. The nearest organ distance to the access tract in each pole of kidney was measured to identify the risk of organ injury (Fig. 2).
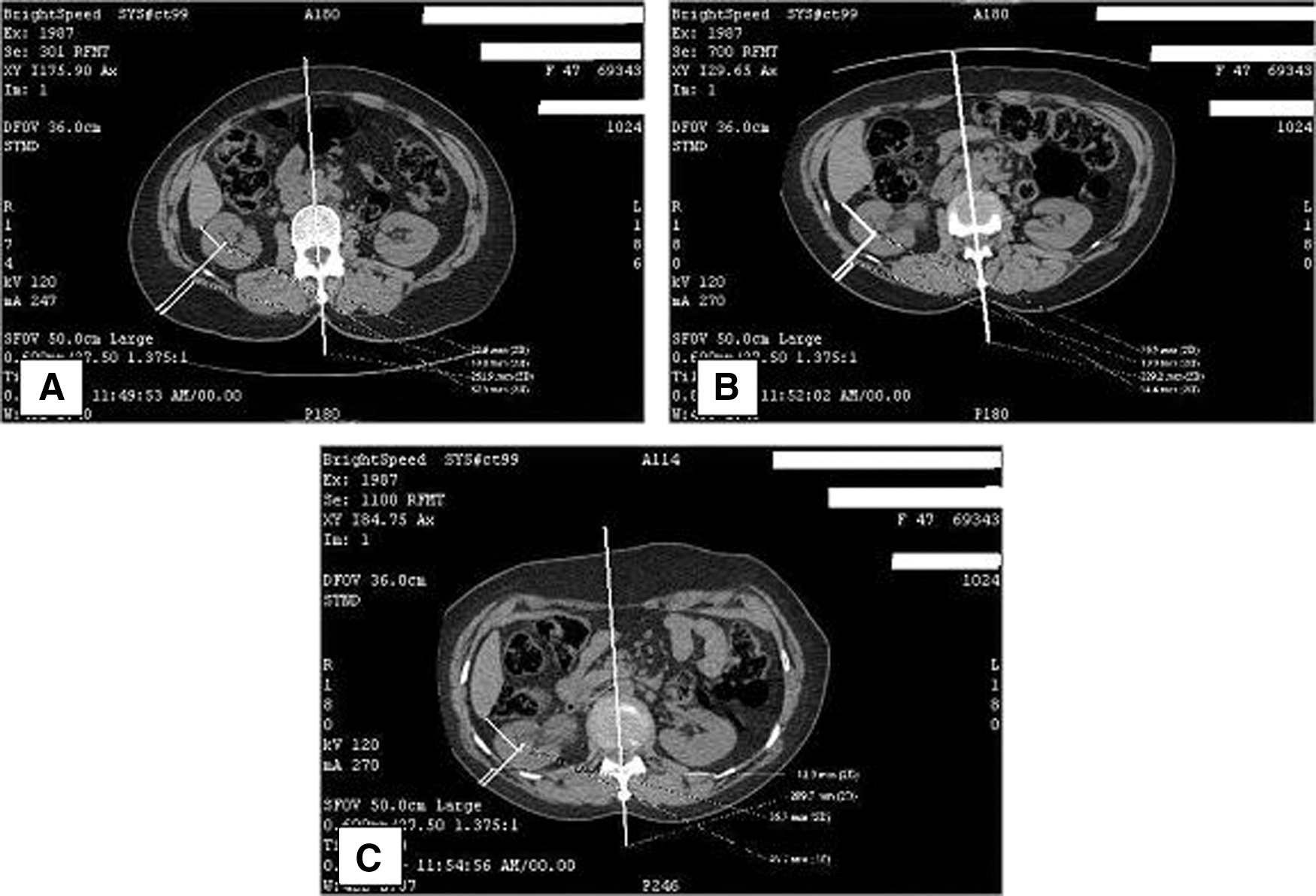
The measurements of access tract length, subcutaneous tissue length, and nearest organ distance.
The maximum access angle was established in axial images by measuring the angle between the lateral margin of the paraspinous muscle and the distant posterior aspect of the liver, spleen, or colon at the level of renal pelvis. Additionally, the access field was determined by measuring the distance between the tip of the 12th rib and superior edge of iliac crest in coronal images. Renal displacement of kidney in variable positions was evaluated with both the inner and outer distance of kidney to the midpoint of the lumbar vertebra. We used the most inferomedial renal parenchyma of kidney at the hilar level to measure the inner distance and most lateral border of kidney at the same level for the measurement of outer distance (Fig. 3).
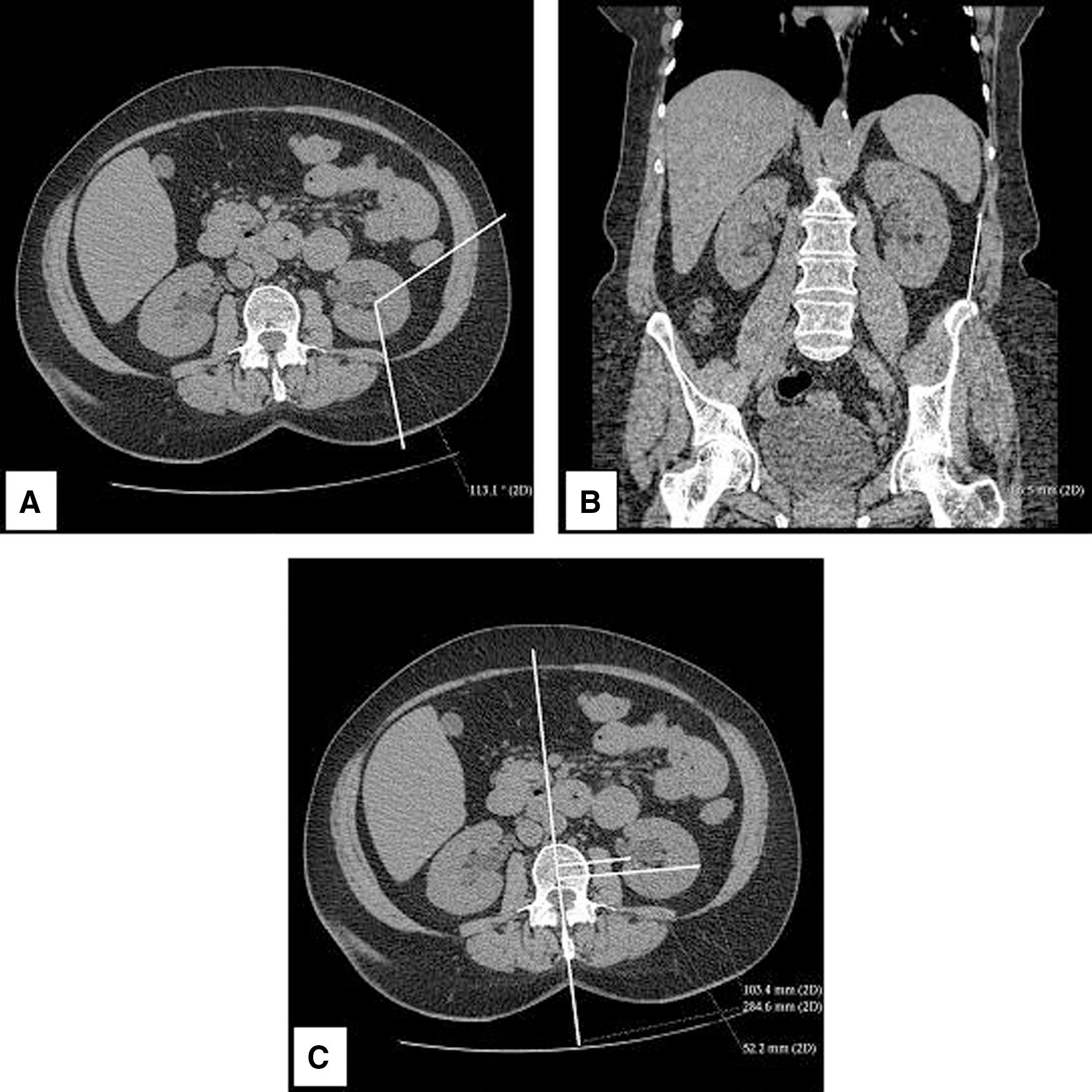
The measurements of study variables.
The data were analyzed by using SPSS 16.0 version. We performed normality analysis using the Kolmogorov–Smirnov test. The paired t-test and Wilcoxon signed test were run for normally and non-normally distributed data, respectively.
Results
The mean age of the study population was 48.1 years, ranging between 36 and 62 years. There were 21 (70%) female and 9 (30%) male patients. Half of the patients had right and the other half had left renal stone disease. None of the patients had cortical or collecting system masses that may lead to miscalculation.
The mean access tract lengths of lower, middle, and upper calyces were significantly longer in the supine position in each pole (Table 1). The access tract lengths shortened as the patients were flexed 30° from the umbilicus. A similar relation was also observed in subcutaneous tissue thickness, as it was significantly longer in the supine position. This thickness also shortened as the patient was bent to the prone-flex position. When the subcutaneous tissue length was subtracted from the whole tract length, the significance of difference between the positions had disappeared (Table 1). The subcutaneous tissue length seemed to be the main determinant of different tract lengths in different positions.
Net tract length=access tract length−subcutaneous tissue length. The parameters in the table were analyzed by the paired t-test.
p Indicates the statistical analysis between groups of supine and prone positions.
p Indicates the statistical analysis between groups of supine and prone-flex positions.
p Indicates the statistical analysis between groups of prone and prone-flex positions.
The maximum access angle and the distance between the 12th rib and iliac crest were used to evaluate the access availability of the supine, prone, and prone-flex positions. There was no significant difference between positions in terms of access angle. However, the distance between the 12th rib and iliac crest was significantly shorter in the supine position (Table 2). The inner (hilar) distance of the kidney was shorter in the supine position indicating that the kidney was more medial in the supine position, but this difference was not significant. When the patient was given the prone-flex position, the inner distance became shorter placing the kidney more medially (Table 2). With the outer distance measurements, we observed that the kidney was located more medially in the prone-flex position, then, after comes the supine position. The kidney was more laterally located in the prone position and the differences of outer distances were significant between all positions.
The analysis of access field and renal position inner distance was performed by the Wilcoxon signed test. The other parameters were analyzed by the paired t-test.
p Indicates the statistical analysis between groups of supine and prone positions.
p Indicates the statistical analysis between groups of supine and prone-flex positions.
p Indicates the statistical analysis between groups of prone and prone-flex positions.
To determine the possible organ damage, we evaluated the nearest organ distance to the access tracts of each pole. The only significant difference was observed between the supine and prone-flex position through the lower pole access and the nearest organ distance was significantly longer in the supine position. Although it was not statistically significant, the supine position has also a longer organ distance than the prone position in lower calyx accesses. For both middle and upper pole accesses, the mean nearest organ distance to access tracts was similar in each position (Table 2).
During the lower pole access, no possible organ damage was detected. In middle pole access, one patient had possible liver puncture in prone and one patient had possible colon puncture in prone-flex position. There was no possible organ puncture during the middle pole access in the supine position. For the upper pole puncture, three patients had possible risk of organ damage in the supine position (two liver and one spleen), two patients in the prone position (one liver and one spleen), and one patient in the prone-flex position (liver). The organ distances of those patients in different positions are shown in Table 3.
Discussion
PCNL is the gold standard surgical technique for large stones, staghorn calculi, stones that are resistant to fragmentation, and kidney stones with abnormal anatomies. 6 The safety and affectivity of this procedure has been documented for more than 30 years. Since the introduction of first cases by Alken et al., the prone position had been the only surgical position for PCNL. 2 It provided several advantages like larger surface for kidney puncture, wider space for instrument manipulation, higher possibility for multiple accesses, and lower probability for organ injury. It was crucial that there were also some disadvantages like discomfort for both the patient and surgeon, the need for repositioning the patient, anesthesiological difficulties, and probable risks of circulatory and ventilatory complications. 7 To overcome these disadvantages, Valdivia et al. described a new position for PCNL. With their series of more than 500 patients, they described the supine positioning PCNL and advocated several benefits of this technique especially in patients with high risk of anesthesiology. 5 They also proposed that, this technique may decrease the surgical time. After the description of this technique, several studies had been performed to compare supine PCNL and prone PCNL. 3,4,7 –9 In most of these studies, supine PCNL seems to be feasible with similar stone-free rates and shorter operation time. Although the safety and feasibility of the technique was shown, most of the urologists regret to use this technique in their daily practice. One of the main reasons of this regression may be the adaptation. Most of the surgeons may feel more comfortable with the technique that they were educated with and used to perform. The knowledge of anatomical changes in supine position may be helpful to make this adaptation easier. For this reason, it is important to determine the anatomical alterations in the supine position and clarify their affect on possible complications related with the positional change.
The access tract length is an important variable of PCNL. A longer track length may decrease the maneuvering ability of surgeons and affect the surgical success and complication rates. The tract lengths in our study were significantly longer in the supine position and the difference was more distinct in lower pole accesses. Our results were similar with the study of Duty et al. 10 They also demonstrated that the tract distance was longer in the supine position. An interesting issue about tract distance was, when we subtracted the subcutaneous tissue distance from the whole tract distance, the significance between the positions had disappeared. For this reason, we proposed that the main determinant creating the tract distance differences was the subcutaneous tissue thickness. It is well known that one of the indications for supine PCNL is a morbidly obese patient. Morbid obesity can be a reason for cardiopulmonary complication during the prone position and supine PCNL may decrease the risks of these patients. On the other hand, the subcutaneous fat tissue will also be thick and will be displaced with the gravity making the access tract length much longer for morbidly obese patients. As the tract distance increases, the surgeon may need longer access sheaths, which may be hard to manipulate. For this reason, morbid obesity, which is one of the main indications for supine PCNL, can also lead to some technical problems that the surgeon has to deal with.
The access area is also important in PCNL. Duty et al. reported that, the distance between the 12th rib and superior edge of iliac crest was greater in the prone position. 11 This finding was also identical to our study. The distance between the 12th rib and the superior edge of the iliac crest decreased significantly, with a mean of 6 cm, as the patient was positioned from prone to supine. This decrease in the access area may lead to a limitation for manipulations and may interfere with the application of multiple accesses during surgery. Another way of demonstrating the access field was the measurement of maximum access angle. Duty et al. evaluated the maximum access angles in every pole of the left and right kidneys and found that, the overall mean angles in both the left and right side were significantly wider in the prone position. However, when they evaluated the angles according to poles, the significant differences were found only in the upper pole of left kidney and lower and upper pole of right kidney. There was no significant difference at the midpole region. We also evaluated the maximum access angle at the midpole region and found no difference between the supine and prone position. As a result, the maximum access angle did not change at the level of midpole, but access field became limited in the supine position.
There are several debates about the risk of splanchnic injury during supine PCNL. Fear of organ injury caused hesitancy among urologists to adapt this technique. Most of the studies comparing prone and supine PCNL demonstrated the safety of the supine position. In a systemic review analysis, Basiri and Mohammadi Sichani evaluated a total of 1459 supine PCNLs and reported no colon injury. 9 On the other hand, de la Rosette et al. pointed out to the fact that, in most studies, supine PCNL was performed for uncomplicated renal stones, which may cause bias to evaluate the feasibility of supine PCNL. 4 In another review, Lashay et al. also evaluated two randomized and two case–control studies and reported that there was no organ injury. 12 –16 They also concluded that these results may not be enough to prove the safety of supine PCNL because very few complex stones (staghorn stones, stones in more than one calyx) were included in the studies. 12 For this reason, anatomical variations that occur in the supine position must be well understood to estimate possible organ injury. We did not observe any possible colon injury during lower pole access in the supine, prone, or prone-flex position, which was eligible with clinical studies. The comparison studies of supine PCNL had mostly lower pole accesses and supine PCNL was found to be a safe technique for splanchnic injury. We found that the access tract of lower pole in a supine position is safe and had a 2 cm longer distance to the colon compared with the prone position. This was also true for middle calyx accesses that none of the patients in the supine position had a risk of splanchnic injury. However, the safety of the procedure became questionable for the upper calyx accesses. There were three patients with a risk of liver or spleen injury in the supine position. However, the same risk was also found in the prone position that two patients had risk of organ injury. As a result, supine positioning did not increase the risk of splanchnic injury in lower, middle, or upper calyx accesses. Beside this, lower pole accesses seemed to be safer in the supine position.
Renal displacement in the supine position is another issue of debate. Duty et al. evaluated the anterior displacement of kidney in prone and supine position and reported no difference between these positions. 10 We evaluated the medial displacement of kidney in the supine, prone, and prone-flex position. The hilum of kidney was located more medially in the supine position, but the difference was not significant. On the other hand, medial displacement of kidney was more pronounced at the outer limit of kidney and the difference was statistically significant. This may be related with the anatomical property of kidney. The kidney has a fixed hilum with great vessels and lymphatic, which may explain the minimal displacement in the hilar level, whereas the displacement became more significant in the floater lateral surface of the kidney. When the patient was given a 30° prone-flex position, the kidney moved more medially.
Our study had some limitations. First of all, this was not a clinical study as we did not perform supine PCNL to our patients. For this reason, we are not able to compare our preclinical data with real-time clinical results. Our study was designed as a simulation of a surgery, so we are only able to define the possible problems that may be seen during the surgery. The second limitation was about the study design. Due to ethical limitations, we were not able to use contrast material, which would be very helpful to identify a specific point for measurements. To eliminate this problem, we used multiplanar views to identify a constant point as a marker for measurements in each position of the patients.
Conclusions
The supine position causes significantly longer tract length for percutaneous access that may be a disadvantage for the surgical maneuverability of a surgeon. Subcutaneous tissue thickness is the main determinant of access tract and morbidly obese patients may need longer access sheaths. The access field is more limited in the supine position that may be a trouble for complex surgeries, but the risk of splanchnic injury in the supine position is similar to the prone position.
Footnotes
Disclosure Statement
The authors do not have any conflict of interests and no competing financial interests exist.