
Abstract
Objectives:
To describe a large clinical series of pure laparoscopic radical nephrectomy (LRN) for left renal cell carcinoma (RCC) with differential extensions of level I renal vein (RV) tumor thrombus using a retroperitoneal approach.
Methods:
Ten left RCC patients with RV tumor thrombus underwent pure retroperitoneal LRN. Operation procedures were different for patients with varying length of the RV tumor thrombus. Based on our experience, four grades were defined based on the distal limit of the thrombus. Grade 1: tip of the thrombus was located between the renal sinus and the left gonadal vein (or adrenal vein); Grade 2: tip of the thrombus was located between the left gonadal vein and the abdominal aorta; Grade 3: tip of the thrombus was riding on the abdominal aorta; Grade 4: tip of the thrombus was located in the interaortocaval region. According to this classification, grade 1 in 3 patients, grade 2 in 2, grade 3 in 3, and grade 4 in 2.
Results:
Pure retroperitoneal LRN and thrombectomy were successfully performed for all the patients without requiring open surgery. The mean tumor size for each of the four grades was 5.9, 6.4, 5.8, and 7.6 cm, respectively; the mean thrombus length was 2.1, 3.5, 5.2, and 7.1 cm, respectively; the mean operative time was 85, 103, 137, and 190 minutes, respectively; the average surgical bleeding volume was 67, 110, 143, and 225 mL, respectively. Better procedures are needed to increase the working space for patients with higher grades of thrombus. Surgical margins were negative for all patients. With a mean follow-up of 29 months, two patients developed metastatic disease.
Conclusions:
Despite the technical challenges, pure retroperitoneal LRN for left RCC patients with differential extensions of RV tumor thrombus is safe and feasible in selected patients. However, it is important to note that surgery will be more difficult for patients with higher grades of thrombus.
Introduction
R
Pure or hand-assisted LRN with the management of RV thrombus has been reported over the last decade. Most of these reports were limited because they used the transperitoneal approach, had a small number of patients who underwent the retroperitoneal approach, or patients who had a short RV thrombus. 2 –9 Level I tumor thrombus is more frequently seen in left-sided tumors compared with right-sided tumors. Nearly 50% of the thrombus of left renal tumors is located in the RV at the time of presentation. 10 The left RV is about 6 to 10 cm long, so it is difficult to treat patients who present with varying lengths of left RV thrombus, especially through the retroperitoneal approach, which requires surgeons to work in a narrow space. To the best of our knowledge, when using the retroperitoneal approach, our study includes the largest number of left RCC cases with varying lengths of RV thrombus treated with pure laparoscopic management.
Patients and Methods
We studied ten patients (six males and four females) diagnosed with left renal tumor with RV thrombus between July 2008 and April 2012. The mean age was 64 years (range 41–78 years). The mean body mass index (BMI) was 23 kg/m2 (16.1–31.5 kg/m2). Five patients presented with intermittent or continuous hematuria, four were diagnosed incidentally, and one presented with fever. Blood routine, liver function, renal function, and serum electrolyte tests were within normal limits. Bone scans were normal and chest computed tomography (CT) showed no metastasis. No lymph node involvement was suspicious on abdominal CT imaging.
Preoperatively, Doppler ultrasonography and CT were used to define tumor location and RV extension in all patients. RV filling defects were found in 10 cases and thrombus was located in the left RV and not extended into inferior vena cava (IVC).
We categorized patients with left RV tumor thrombus into four grade groups based on the distal limit of thrombus. Three patients were classified into Grade 1, with the tip of the thrombus located between the left renal sinus and gonadal vein (or adrenal vein) (Figs. 1A and 2A). Two patients were classified into Grade 2, with the tip of the thrombus located between the left gonadal vein (or adrenal vein) and abdominal aorta (Figs. 1B and 2B). Three patients were classified into Grade 3, with the tip of the thrombus riding on the abdominal aorta (Figs. 1C and 2C). Last, two patients were classified into Grade 4, with the tip of the thrombus located in the interaortocaval region (Figs. 1D and 2D).

Axial CT image for Grade 1 to Grade 4 thrombus tip of the thrombus (arrow):
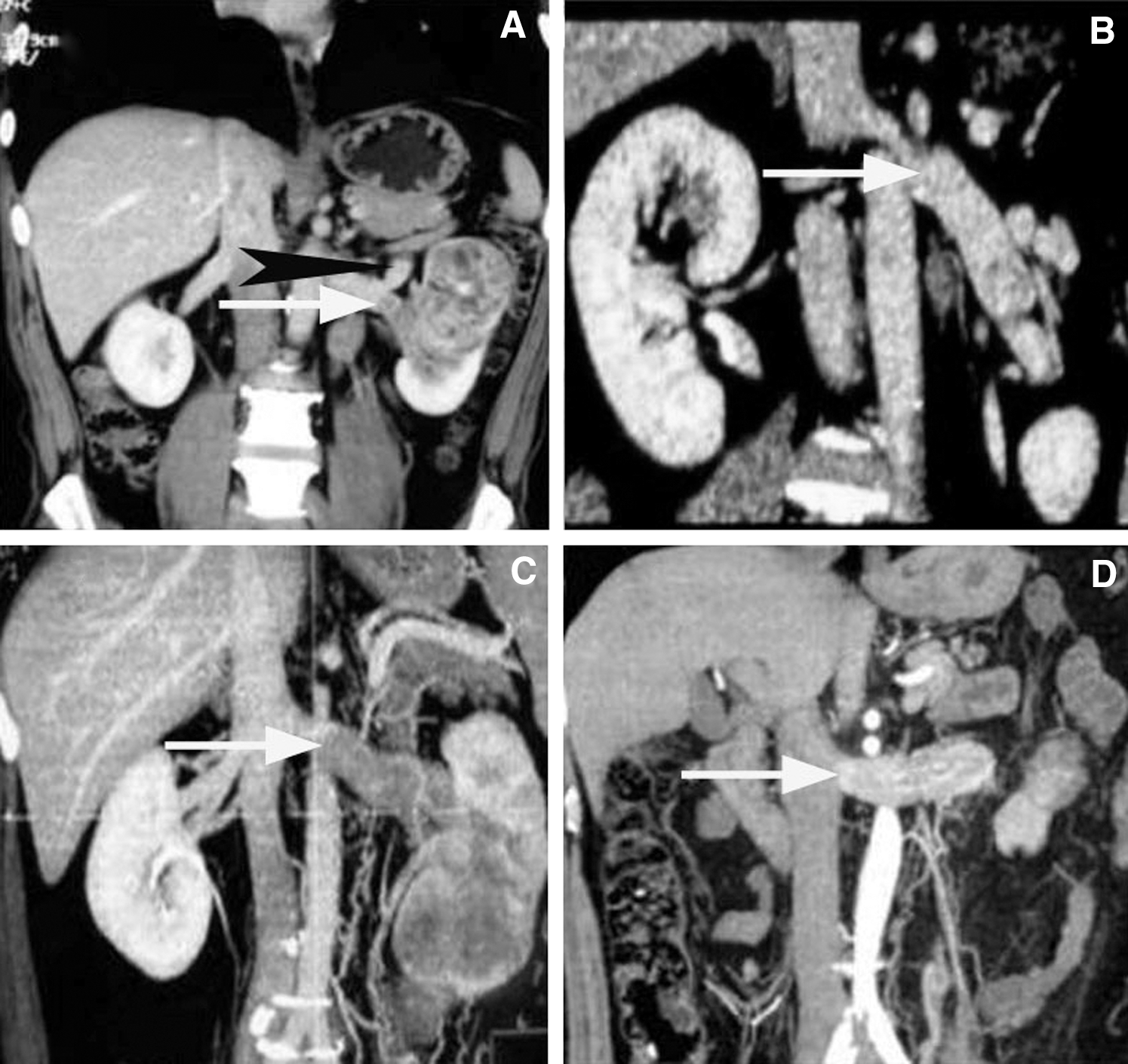
Coronal CT image for Grade 1 to Grade 4 thrombus:
General anesthesia was administered by tracheal cannulation. The patients were placed in an extended flank position, and the four-trocar system was used, including two 10-mm ports and two 5-mm ports. All nephrectomy procedures were conducted with the pure retroperitoneal laparoscopic approach. The renal artery was exposed and ligated with four Hem-o-lok clips, the left RV collapsed, and the distal limit of thrombus could be verified. A laparoscopic ultrasound probe was used to identify the tip of the RV thrombus if it could not be verified visually. The procedures were successful and completely transected proximally to the thrombus using Hem-o-lok clips, three on the tumor side. In cases in which there was not adequate RV length to place the Hem-o-lok clips, milking the thrombus distal toward the kidney can be done using an atraumatic grasper. At the time of surgery, the left renal hilar lymphatic tissue will be removed, and the lymphatic tissue adjacent to the abdominal aorta will be excised in patients with Grade 2, 3, and 4 thrombus, lymphatic tissue adjacent to the superior mesenteric artery will be excised in patients with Grade 3 and 4 thrombus, and lymphatic tissue adjacent to the IVC will be excised in patients with Grade 4 thrombus. The ureter was identified and ligated. The whole kidney together with the Gerota's fascia, perirenal fat with or without the adrenal gland was mobilized en bloc. The specimen was entrapped and removed intact using an Endo catch bag. We calculate the operative time from the first skin incision to application of final dressing. Intraoperative assessment of blood loss is based on the blood volume collected in the suction device bottles and swab weight (if used).
The retroperitoneal space was limited and operation procedures were more complex with higher grades of tumor thrombus. Better procedures are needed to expand the working space. The operative procedure for nephrectomy was not different from the standard LRN for Grade 1 thrombus, we usually do not have to mobilize or dissect the gonadal, adrenal, or lumbar vein, it is optional for dissecting these veins (Fig. 3A). Mobilizing part of the abdominal aorta was needed for Grade 2 thrombus, branches of the left RV are needed to be mobilized and dissected (Fig. 3B). Mobilizing part of the superior mesenteric artery was needed for Grade 3 thrombus, and the residual renal artery stump was sutured to the psoas major muscle (Fig. 3C). The abdominal aorta, superior mesenteric artery, and part of the IVC needed to be mobilized for Grade 4 thrombus, so the thrombus was easily visualized at the junction of the RV and IVC (Fig. 3D) (Supplementary video is available online at
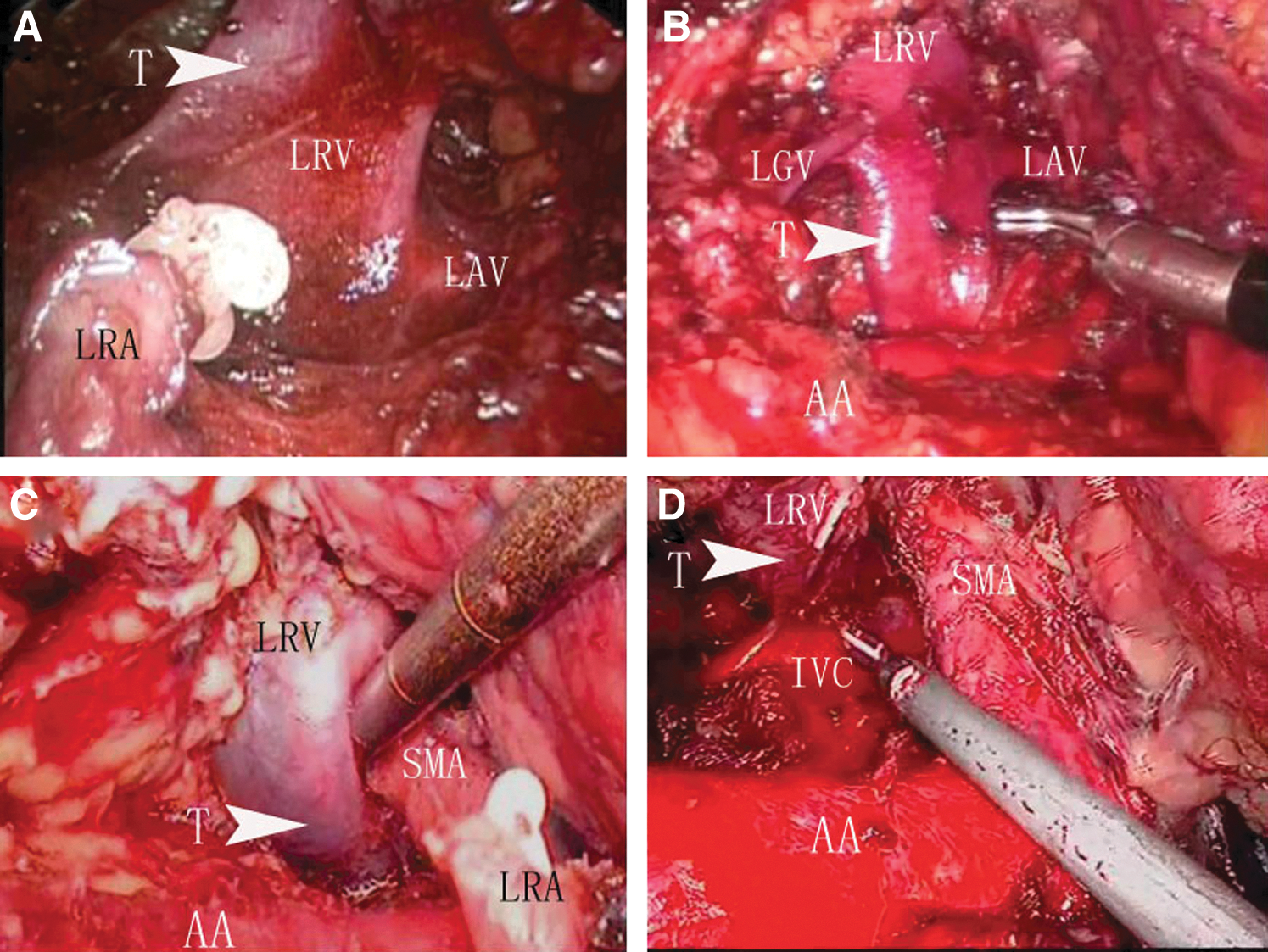
Intraoperative images for Grade 1 to Grade 4 tumor thrombus:
Follow-up measures after LRN at our institute include physical examination, history, laboratory test, chest X-ray, abdominal and pelvic ultrasound every 3 months for the first year and every 6 months for the second year after surgery, and then annually thereafter. CT was performed every 6–12 months for 3 years after surgery or on patients with abnormal findings on laboratory test, chest X-ray, or ultrasound.
Results
All operations were completed laparoscopically without major or minor complications. We did not encounter any intraoperative or postoperative complications, such as superior mesenteric artery and IVC injury, pulmonary embolism, intestinal ischemia, postoperative bleeding, pneumonia, or wound infection. The mean thrombus length for all ten patients was 4.3 cm (range 2.0–7.5 cm). None of the cases required open surgery. The mean operative time was 125 minutes (range 55–220 minutes) and the mean estimated blood loss was 130 mL (range 30–300 mL). None of the patients required a transfusion. The mean tumor size was 6.3 cm (range 5.0–8.5 cm). Pathologically, tumors were confirmed to be clear cell carcinoma in nine patients and chromophobe carcinoma in one patient, with a mean Fuhrman grade of 1.9 (range 1–3). RCC with evidence of perinephric fat invasion was observed in two patients. None of the ten patients had histological evidence of lymph node involvement. All the thrombi were floating intraluminally. The RV vascular margin of the transected vein was negative for cancer in all ten patients. The average hospital stay was 5.4 days (range 4–7 days). With a mean follow-up of 29 months (12–50 months), one patient had contralateral adrenal metastasis 14 months after surgery, and the metastatic tumor was resected. We also observed that one patient had lung metastasis 3 years after surgery. No tumor recurrence or metastasis occurred for any other patients. Patients with higher grades of thrombus experienced longer operative times and more blood loss. Data of clinical characteristics, perioperative variables, and outcomes for patients with Grade 1 to Grade 4 thrombus were noted (Table 1).
Discussion
RCC with RV tumor thrombus is a relatively common malignant disorder in adults. The standard treatment for these patients is radical nephrectomy with thrombectomy and lymph node dissection. The laparoscopic technique has been considered as a less invasive alternative to open surgery; the feasibility, safety, and adequate oncological outcome of pure LRN for patients with RV thrombus have been demonstrated by several groups. 2 –5 In 1996, McDougall et al. 3 reported the first successful case using a purely laparoscopic approach for RV thrombus, but the thrombus was diagnosed postoperatively. Salvage et al. 4 reported a LRN in a RCC patient with level I RV thrombus, and the thrombus was located in the left RV, proximal to left gonadal vein. Desai et al. 5 further reported the initial series of LRN for microscopic and gross level I thrombus, involving a case of Grade 4 thrombus according to our classification through the transperitoneal approach. To date, RCC with RV involvement has not been regarded as contraindications using a minimally invasive technique, but most of these reports have been limited to transperitoneal access or small series of patients with retroperitoneal access or patients with short RV thrombus. 2 –9
As we know, right-sided tumors have very short RV, so the thrombus is easy to extend beyond the RV and into the IVC; left-sided tumors typically have longer RV and influence of abdominal aortic pulsation, nearly 50% of thrombus is located in the left RV at the time of presentation. 10 So, it is difficult to deal with left RCC with varying lengths of thrombus. To our knowledge, this is the first report to discuss the feasibility and technical requirements of pure LRN for left RCC with varying lengths of RV thrombus using a retroperitoneal approach.
Both retro- and transperitoneal approaches can be used, however, we prefer using the retroperitoneal approach because it provides direct, quick access to the hilum and allows early control of the renal artery. In addition, this approach may save the total operative time, prevent tumor spillage and seeding into the peritoneum. 11 Technical challenges are likely to occur during the resection of RCC for the identification of the RV thrombus. 11 It is especially necessary to identify the distal limit of the thrombus before stapling the RV. If the thrombus is located in the interaortocaval region, such as in the case of Grade 4 thrombus, a retroperitoneal approach is strongly recommended. Because it can provide easier access to the left RV without needing to mobilize the colon, and offer excellent exposure of the surgical field, the thrombus can be fully milked back to the kidney more conveniently. 11 In addition, from a technical standpoint, the renal artery can be controlled with less contact with the thrombus bearing RV through the retroperitoneal approach than the transperitoneal approach. 2 –5 Prior abdominal surgery and adhesion will not cause problems in the retroperitoneal route. 11 However, it was more difficult to operate on cases that had larger tumor sizes (generally ≥8 cm) or higher BMI (>30). Steinnerd et al. 9 excluded primary tumors of more than 10 cm so that pure LRN could be safely performed for patients with RV thrombus. So considering the feasibility and safety of the operation, especially for patients with Grade 3 and Grade 4 thrombus, we prefer using this technique in patients with the tumor not exceeding 8–10 cm in diameter, at the same time, metastatic disease, IVC, or perinephric visceral involvement and bulky lymphadenopathy should be absent.
Early arterial division and milking of the thrombus back to the kidney may facilitate laparoscopic surgery. 6,7 All of our patients benefitted from early management of the renal artery, which helped to decrease the intravenous pressure and retracted the thrombus enough to allow more room for Hem-o-lok clips across the vein. Branches of the left RV, such as the lumbar, gonadal, and adrenal veins, should be mobilized and dissected. The dilated portion of the RV with the thrombus was visualized transected proximally to the thrombus with Hem-o-lok clips and not with an endoscopic gastrointestinal anastomosis vessel stapler for short uninvolved veins, especially for Grade 3 and 4 thrombus. Milking the thrombus away from the IVC also helps to ensure its complete incorporation into the pathologic specimen. All tumors can be handled with careful dissection; milking of the thrombus is optional for Grade 1 and 2 thrombus, but Grade 3 and 4 thrombus require milking of the thrombus back to the kidney to ensure negative margins. A frozen-section evaluation should be performed to ensure a tumor-free margin.
In addition, for patients with Grade 3 and 4 thrombus, the dissection of left RV was challenging because it was partially located between the superior mesenteric artery and the abdominal aorta. We sutured the residual renal artery stump to the psoas major muscle to reduce the influence of abdominal aortic pulsation on operative dissection. We also recommend that the superior mesenteric artery be mobilized as long as possible, and at the same time, great caution should be taken to avoid injury of this artery. For patients with Grade 4 thrombus, part of the IVC should be mobilized so that the tip of the thrombus can be visualized clearly. An extensive posterior mobilization aids in quicker hilar exposure, 12 but we also believe that different degrees of posterior dissection for patients with varying lengths of thrombus will facilitate hilar exposure, saving operation time and also avoiding some unnecessary injuries.
Most RCC patients with RV thrombus do not have specific symptoms. Imaging investigations are especially important for accurate preoperative diagnosis. An insufficient knowledge of grading for RV thrombus is the primary cause for surgical mishaps. Preoperative CT with three-dimensional reconstruction or MR angiography reconstruction should be performed to aid in surgical planning. 8 In the present study, the extent of the thrombus was revealed using the CT scan with three-dimensional reconstruction. A laparoscopic ultrasound probe can be used to characterize the distal extent of the thrombus or if there is suspicion of venous involvement intraoperatively. 5,8,9
Early open conversion or a hand-assisted approach should be strongly considered in cases involving extensive inflammatory hilar anatomy, vascular invasion, positive margin, and vascular injury. 2,8 It is impossible to deal with level II thrombus using the retroperitoneal approach for left RCC given its limited access to the IVC. 13 A few cases have been reported to open conversion in the literature, Guzzo et al. 2 reported one conversion for difficult laparoscopic dissection, and Kapoor et al. 8 reported two conversions for hilar adenopathy and level II thrombus, respectively. Despite the technical challenges, especially for patients with Grades 3 and 4 thrombus, no conversions to open surgery were required in our groups.
Henderson et al. 14 reported results for 12 patients, with a median follow-up of 31 months, who underwent hand-assisted LRN; three patients developed metastatic disease. Martin et al. 15 reported 14 patients with a mean follow-up of 32 months; two patients developed metastatic disease. After more than two years of mean follow-up, two patients in our group were found to have contralateral adrenal and lung metastasis separately; longer term follow-up data are needed for ultimate validation of the efficacy of this cancer treatment. This report shows that pure retroperitoneal LRN is safe and feasible for the treatment of left RCC with varying lengths of RV thrombus, with the advantage of being a less invasive procedure. However, we only confirmed the feasibility of this technique and not to prove that it should be done, especially for the Grade 3 and Grade 4 thrombus; patients with larger tumors, higher BMI, and a higher grade of thrombus will experience longer operative times; experience and patience are critical.
LRN has been widely accepted as an option for RCC patients with venous thrombus. With the expanding use of robotic technology, robotic heminephrectomy for RCC in a horseshoe kidney with RV thrombus has been performed first by Rogers et al. 16 in 2008, in addition, robotic surgery has been successfully used by Abaza 17 in RCC patients with IVC thrombus, the authors indicated a potential benefit in such scenarios of robotic instrumentation. Robotic nephrectomy and thrombectomy is feasible in well-selected patients, but this technique requires a skilled laparoscopist with extensive experiences.
Our classification has its limitations. First, it is a classification dependent on the relative length of RV, the actual left RV length is from 6 to 10 cm, the surgical difficulty may be varying for patients with the same grade of thrombus; Second, there are some vascular variations, including IVC, left RV and its branch variations. The percentages of retroaortic left RV, circumaortic left RV, and duplicate IVC were 3.1%, 2.1%, and 0.2%, respectively, 18 and the anatomic relationship between the left RV, gonadal vein, and adrenal vein is different for each individual. The position of the gonadal vein junction to the RV may introduce variations in grading the thrombus involvement, but the relative gonadal vein position does not affect our classification system. In our opinion, this classification may still be helpful for surgeons to know what needs to be done and how to complete this procedure using the retroperitoneal approach.
Conclusions
We first discuss the safety and feasibility of left RCC with differential extensions of RV tumor thrombus receiving pure LRN through the retroperitoneal approach in detail. It is safe and feasible for selected patients. However, better operation procedures are needed and the surgical difficulty will increase with higher grades of thrombus.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.