
Abstract
Objective:
To evaluate the safety, efficacy, and potential advantages of off-clamp partial nephrectomy (OFF-PN) compared with on-clamp partial nephrectomy (ON-PN).
Methods:
Relevant studies comparing the safety and efficacy of OFF-PN to ON-PN were identified through a literature search using MEDLINE, EMBASE, and the Cochrane Library. The outcome measures included baseline characteristics, primary outcomes, and secondary outcomes.
Results:
Ten retrospective studies (728 cases and 1267 controls) were included. No significant differences between the two groups were detected in any of the baseline variables (age: p=0.19; sex: p=0.49; BMI: p=0.29; tumor size: p=0.44, pre-eGFR: p=0.78) except for tumor location (p<0.001). The OFF-PN group had a higher blood transfusion rate (odds ratio [OR] 1.54, 95% confidence interval [CI] 10.7–2.21, p=0.02), a lower postoperative complication rate (OR 0.61, 95% CI 0.44–0.83, p=0.002), and a lower positive margin rate (OR 0.49, 95% CI 0.26–0.90, p=0.02) than ON-PN. OFF-PN offered a better preservation of renal function than ON-PN (p=0.005). No significant differences were detected between the two groups in other outcomes of interest. In sensitivity analysis, there was no change in the significance of any of the outcomes except for postoperative complication rate (OR 0.91, 95% CI 0.53–1.5, p=0.73) and positive margin rate (OR 0.55, 95% CI 0.25–1.23, p=0.15).
Conclusions:
This meta-analysis suggests that with appropriate patient selection, OFF-PN offer comparable perioperative safety, equivalent oncologic outcomes, and superior long-term renal function preservation when compared with ON-PN for renal cell carcinoma. Given the inherent limitations of the included studies, future well-designed randomized controlled trials are required to confirm our findings.
Introduction
R
To provide a bloodless operative field that facilitates tumor excision and renal reconstruction, transient hilar clamping is typically required during PN. However, hilar clamping inevitably results in renal warm ischemia (WI) injury, an important cause of renal failure. Although the effect of WI on renal function is still controversial, recent studies considered 25 minutes as the acceptable safety threshold of WI time during PN and demonstrated that every minute of hilar clamping has a deleterious effect on renal function outcomes. 4,5 Therefore, to completely eliminate WI injury, off-clamp partial nephrectomies (OFF-PN) have been selectively performed in recent years. This innovative technique, in which the renal pedicle is left unclamped, has proven feasible in open and minimally invasive PN. 6 –8
Although several studies comparing OFF-PN to conventional on-clamp PN (ON-PN) have been published, it is still unclear whether OFF-PN can offer a better preservation of renal function without sacrificing patient safety and survival. This confusion may be related to the low incidence (such as positive margin rate: 0%–4.6% 9,10 ) and small sample size 9,11 –13 that prevent statistically significant measurements. Therefore, a systematic review and meta-analysis of the available literature was performed to evaluate the safety and efficacy of OFF-PN compared to ON-PN.
Materials and Methods
Search strategy and study selection
The systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 14 A literature search was performed to identify relevant studies comparing the safety and efficacy of OFF-PN to ON-PN using MEDLINE, EMBASE, and the Cochrane Library from 1998 to August 2013. The search terms were (“partial nephrectomy” OR “nephron sparing surgery” [Title/Abstract]) AND (“off-clamp” OR “unclamped” OR “not to clamp” OR “zero-ischemia” OR “clampless” [Title/Abstract]). No language restriction was applied. The references of retrieved articles were also searched for additional studies.
Studies selected met the following criteria: (1) focused on pure OFF-PN, while those focusing on segmental renal artery clamping were excluded; (2) direct comparative trials, including randomized controlled trials (RCT) and retrospective studies; (3) evaluated at least one of the perioperative complications or renal function changes; (4) provided sufficient original data for comparison; (5) the number of each group ≥10; and (6) for studies focusing on the same population, the study providing more relevant information was included. Case series, animal experimental studies, letters to editors, and reviews were excluded. For data unprovided in relevant studies, a direct communication with the corresponding author was made.
Data extraction and quality score assessment
Data from relevant studies were carefully and independently extracted by two authors (Minfeng Chen, Li Gu). Discrepancies were resolved through discussions with another author (Wentao Liu). For studies that presented continuous data as mean and range values, standard deviations (SDs) were calculated according to statistical algorithms. 15
The methodological quality of included studies was assessed by two authors using the levels of evidence and grades of recommendation 16 and the Downs and Black tool 17 for both RCT and non-RCT. In general, the quality score (Downs and Black tool) was divided into following four levels: <14, 15–19, 20–25, and 26–28.
Outcomes of interest
The baseline characteristics were age, sex, BMI, pre-eGFR, tumor size, and location. Tumor location (exophytic and nonexophytic) was defined based on the proportion of their volume within the renal parenchyma. 18
The primary outcomes were blood transfusion rate, conversion rate, positive margin rate, complication rate, urinary leakage rate, and changes in renal function. Conversions in OFF-PN were defined as “converting to ON-PN” or “open operation.” When sufficient data was available, the overall complications were subdivided into intraoperative and postoperative complications. Postoperative complications were further subdivided into minor and major complications according to the Clavien-Dindo classification system. 19
The secondary outcomes were operating time, estimated blood loss (EBL), and length of hospital stay (LOS).
Statistical analysis
Comparisons of continuous and dichotomous variables were performed using weighted mean difference (WMD) and odds ratio (OR), respectively, along with 95% confidence interval (95% CI). A p-value<0.05 was considered statistically significant. The presence of heterogeneity between studies was calculated by the Chi-square-based Q test and I 2 . A p-value<0.1 was considered heterogeneous and I 2 <50% was considered acceptable heterogeneity. When significant heterogeneity was found (p<0.1), the pooled effect was calculated by a random-effects model (the DerSimonian and Laird method). 20 Otherwise, the fixed effects model (Mantel–Haenszel method) 21 was used. To explore the potential effect of heterogeneity, sensitivity analysis for cohorts with comparable tumor size and location was performed. Begg's funnel plot and the Egger's test were carried out to assess potential publication bias. All the statistical analyses were performed using Review Manager Version 5.0 (The Cochrane Collaboration, Oxford, London, United Kingdom) and STATA software (version 12.0; Stata Corporation, College Station, TX).
Results
Characteristics of studies
A total of 10 studies (728 cases and 1267 controls) were included in our meta-analysis (Fig. 1). 6 –13,22,23 Characteristics and qualities of these included studies are summarized in Table 1. All included studies were retrospective nonrandomized trials, and published within recent 3 years, indicating the increased usage of this technique. As for surgical approaches, four studies were on laparoscopic PN (LPN), four studies were on robot-assisted LPN (RPN), two studies were on open PN (OPN), and one study was on a mixed approach. The mean Downs and Black assessment score of the included studies was 15.5 (SD 1.2, range 14 to 17).

Flowchart of the screening process.
LOE=level of evidence; LPN=laparoscopic partial nephrectomy; NR=not reported; OFF-PN=off-clamp partial nephrectomy; OPN=open partial nephrectomy; R=retrospective; RP=retrospective design, prospective data collection; RPN=robot-assisted laparoscopic partial nephrectomy.
Quantitative synthesis
At baseline (Table 2), no differences were detected between OFF-PN and ON-PN groups in terms of age (WMD: −0.75, 95% CI: −1.88 to 0.37, p=0.19), sex (OR: 0.90, 95% CI: 0.65–1.23, p=0.49), BMI (WMD: −0.13, 95% CI: −0.38 to 0.11, p=0.59), tumor size (WMD: −0.24, 95% CI: −0.85 to 0.37, p=0.44), and pre-eGFR (WMD: 0.82, 95% CI: −4.99 to 6.63, p=0.78). However, tumors in the OFF-PN group were less endophytic (OR: 0.49, 95% CI: 0.36–0.67, p<0.001).
Random-effects model.
Statistically significant values are highlighted in bold.
WMD/OR=weighted mean difference/odds ratio; EBL=estimated blood loss; LOS=length of hospital stay; ON-PN=on-clamp partial nephrectomy; CI=confidence interval.
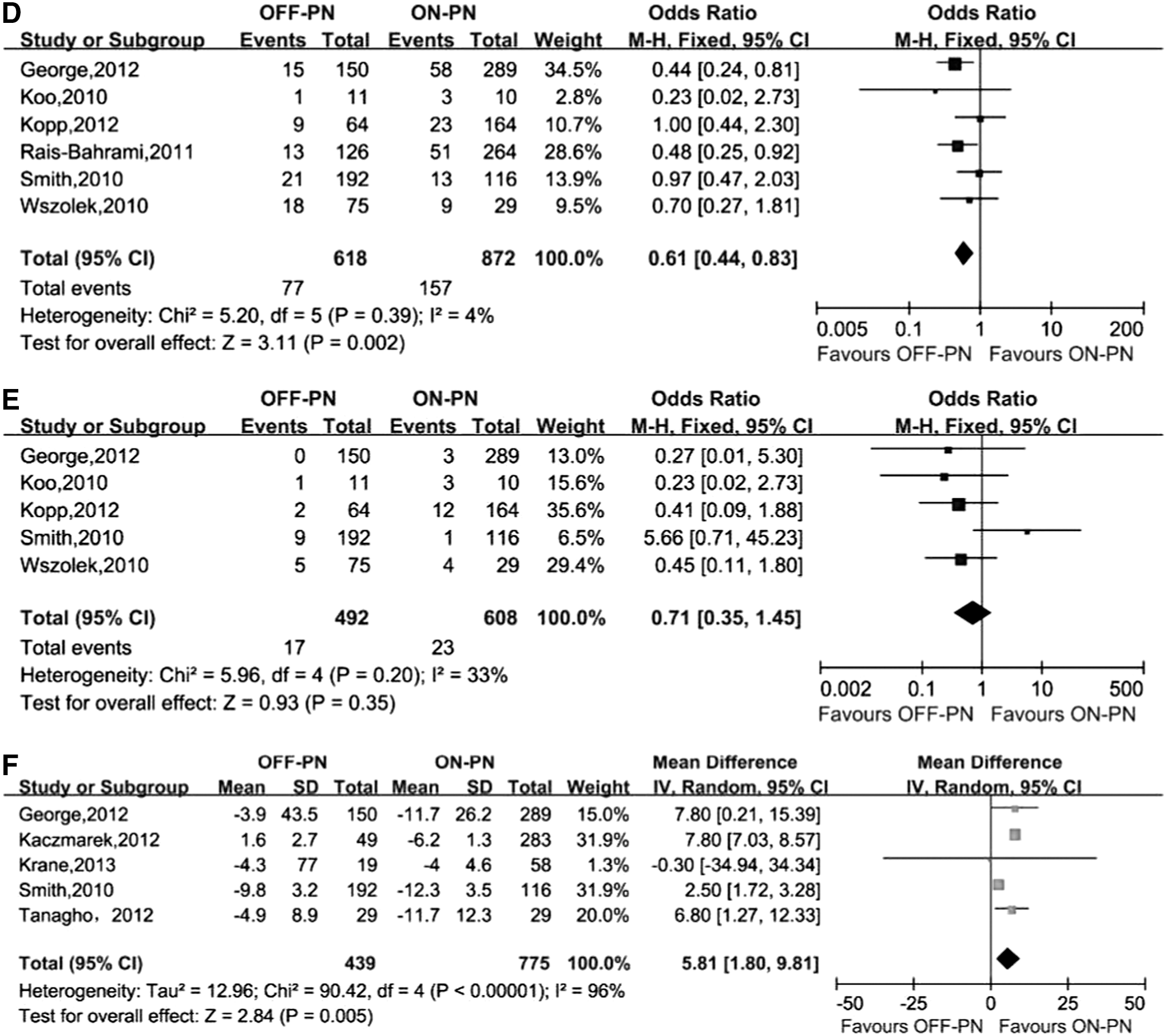
With regard to primary outcomes, only one study 6 reported intraoperative complications, and six studies 6,8 –11,22 reported postoperative complications (two of those studies applied the Clavien classification system 6,9 ). Therefore, we only compared the postoperative complications between the two groups. The postoperative complication rate was significantly lower in OFF-PN than ON-PN (12.5% vs 18%, p=0.002) (Fig. 2) and the positive margin rate was also significantly lower in OFF-PN than ON-PN (2.4% vs 3.2%, p=0.02) (Fig. 2). In contrast, the blood transfusion rate was significantly higher in OFF-PN than ON-PN (15.3% vs 6.3%, p=0.02) (Fig. 2). The conversion rate and urinary leakage rate were similar in the groups (conversion: 1.7% vs 1.7%, p=0.93; urinary leakage: 3.5% vs 3.8%, p=0.35) (Fig. 2). The pooled data from five trials that reported eGFR 6,7,10,12,13 showed a better renal function preservation in OFF-PN than ON-PN (decreased eGFR: WMD: 5.81, 95% CI: 1.80–9.81, p=0.005) (Fig. 2).
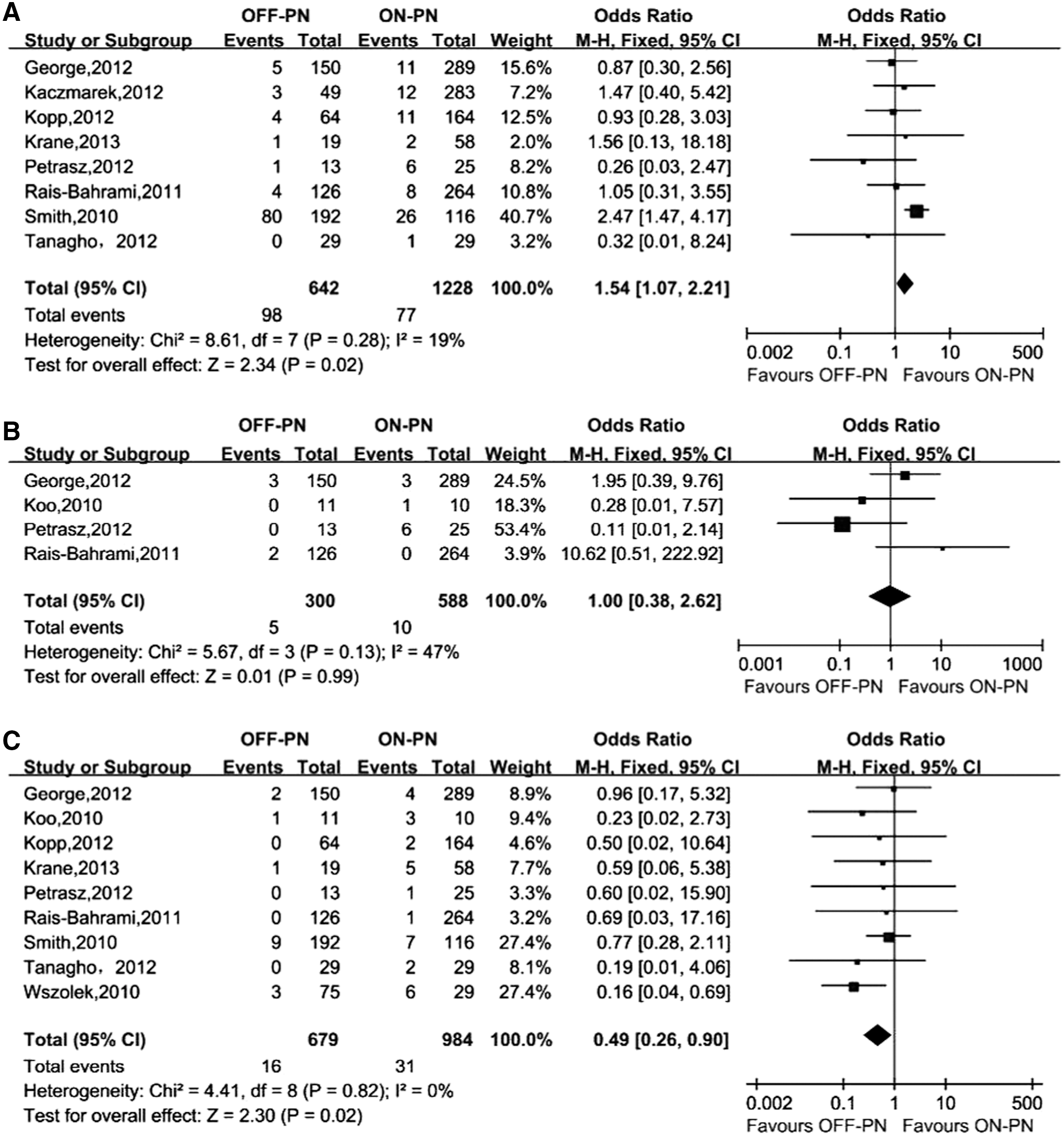
Forest plot of primary outcomes:
With regard to secondary outcomes, there were no significant differences in operating time, EBL, and LOS between the groups (operating time: WMD: −10.02, 95% CI: −37.43 to 17.39, p=0.44; EBL: WMD: 60.74, 95% CI: −5.84 to 127.33, p=0.07; LOS: WMD: 0.37, 95% CI: −0.78 to 1.51, p=0.53) (Table 2).
Sensitivity analysis
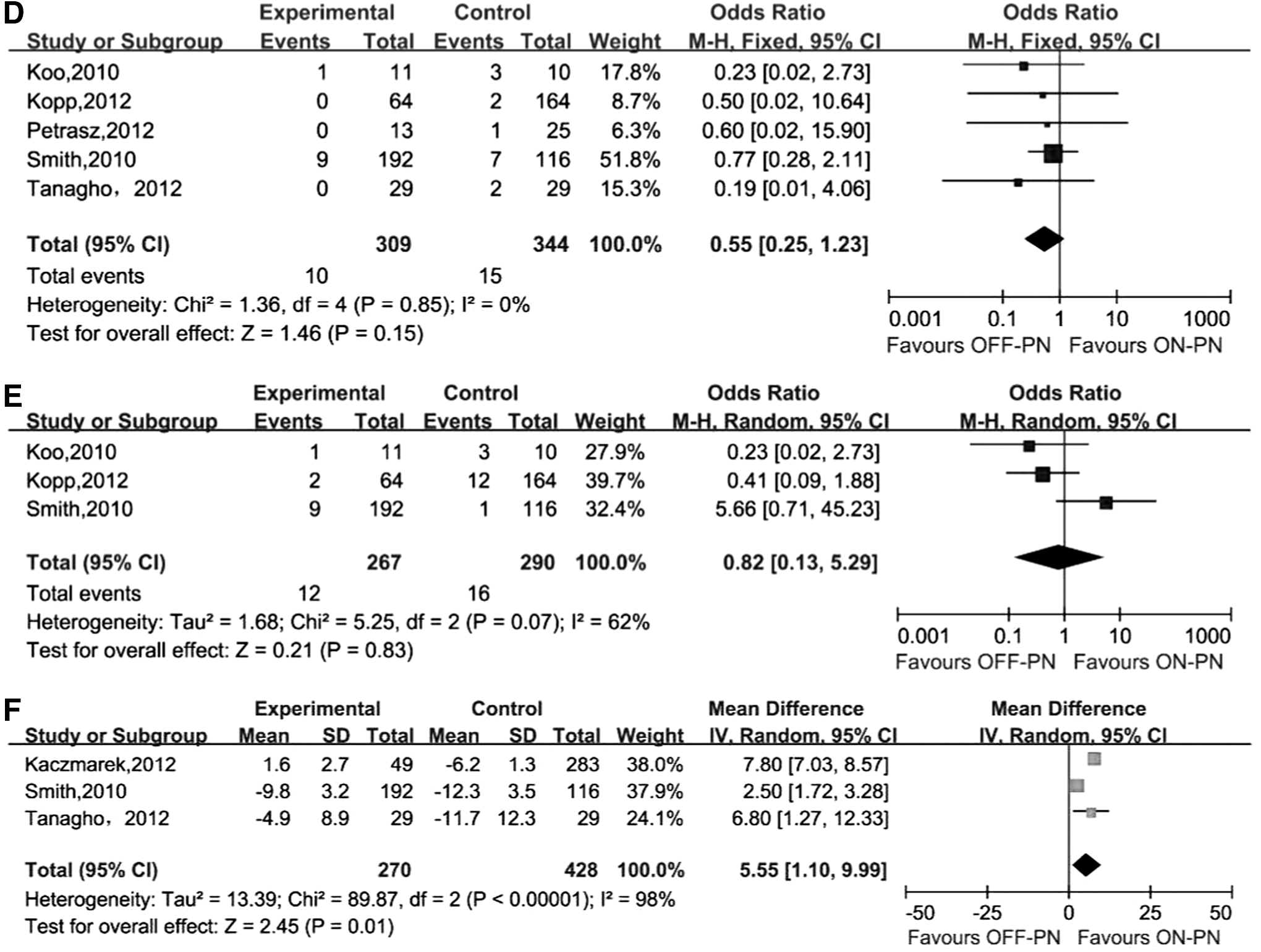
When cohorts with incomparable tumor sizes and locations were removed, there were still no differences between groups in terms of operating time, EBL, LOS, conversion rate, and urinary leakage rate (Table 3). However, the OFF-PN group still had a significantly higher blood transfusion rate (OR: 1.76, 95% CI: 1.16–2.66, p=0.008) and better renal function preservation (WMD: 5.55, 95% CI: 1.10–9.99, p=0.44) than the ON-PN group (Fig. 3). It should be noted that there were no statistical differences in positive margin rate (OR: 0.55, 95% CI: 0.25–1.23, p=0.15) (Fig. 3), and postoperative complication rate (OR: 0.91, 95% CI: 0.53–1.55, p=0.73) (Fig. 3). Heterogeneity between the studies was not reduced in the sensitivity analysis (Tables 2 and 3).
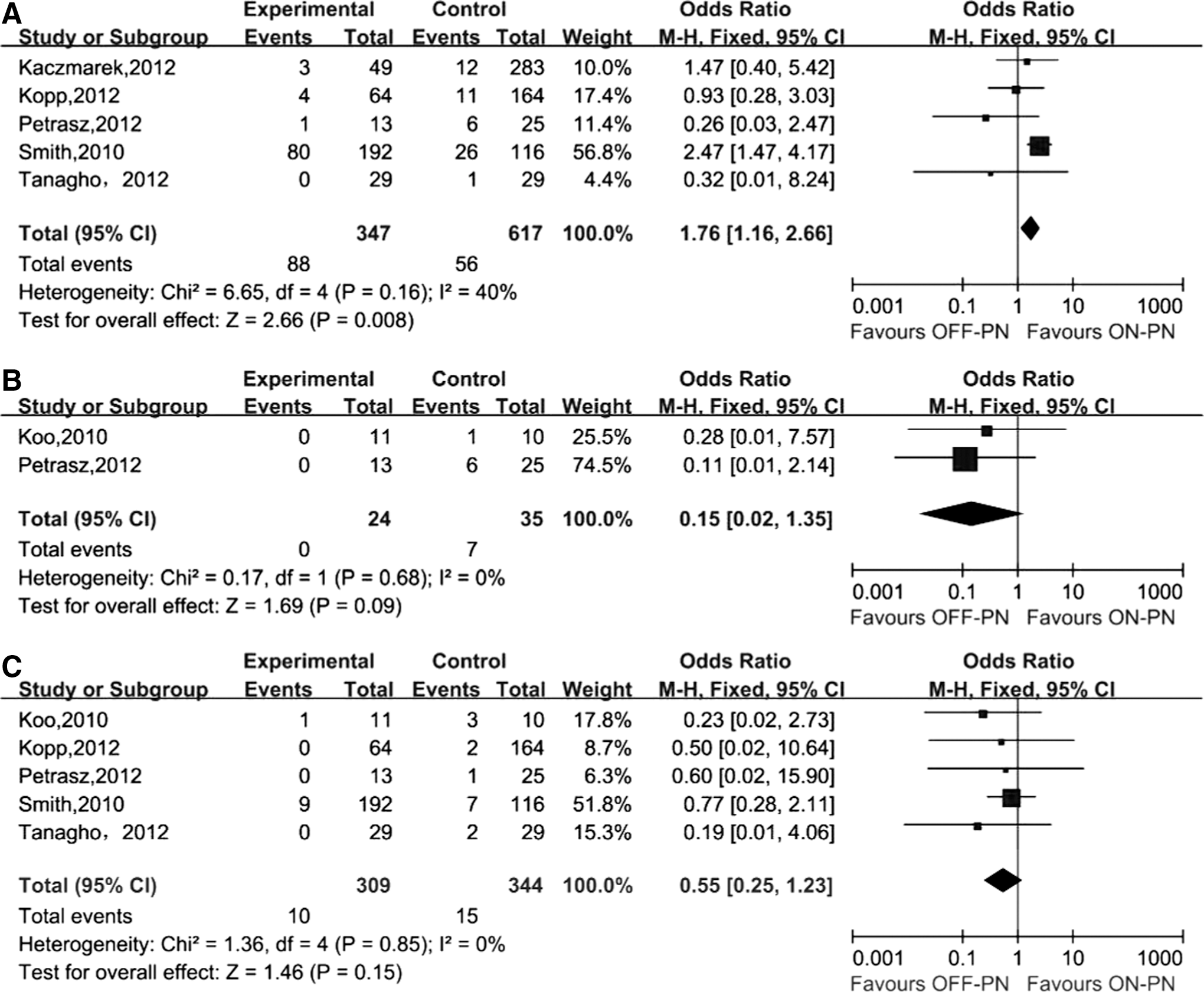
Forest plot of sensitivity analysis of primary outcomes:
Random-effects model.
Statistically significant values are highlighted in bold.
Publication bias
The Begg's funnel plot of blood transfusion showed an apparent asymmetric (Fig. 4). Moreover, p-values of the Begg's test and Egger's test were 0.902 and 0.013, respectively, also indicating significant publication bias. No publication bias was found in other outcomes of interest.
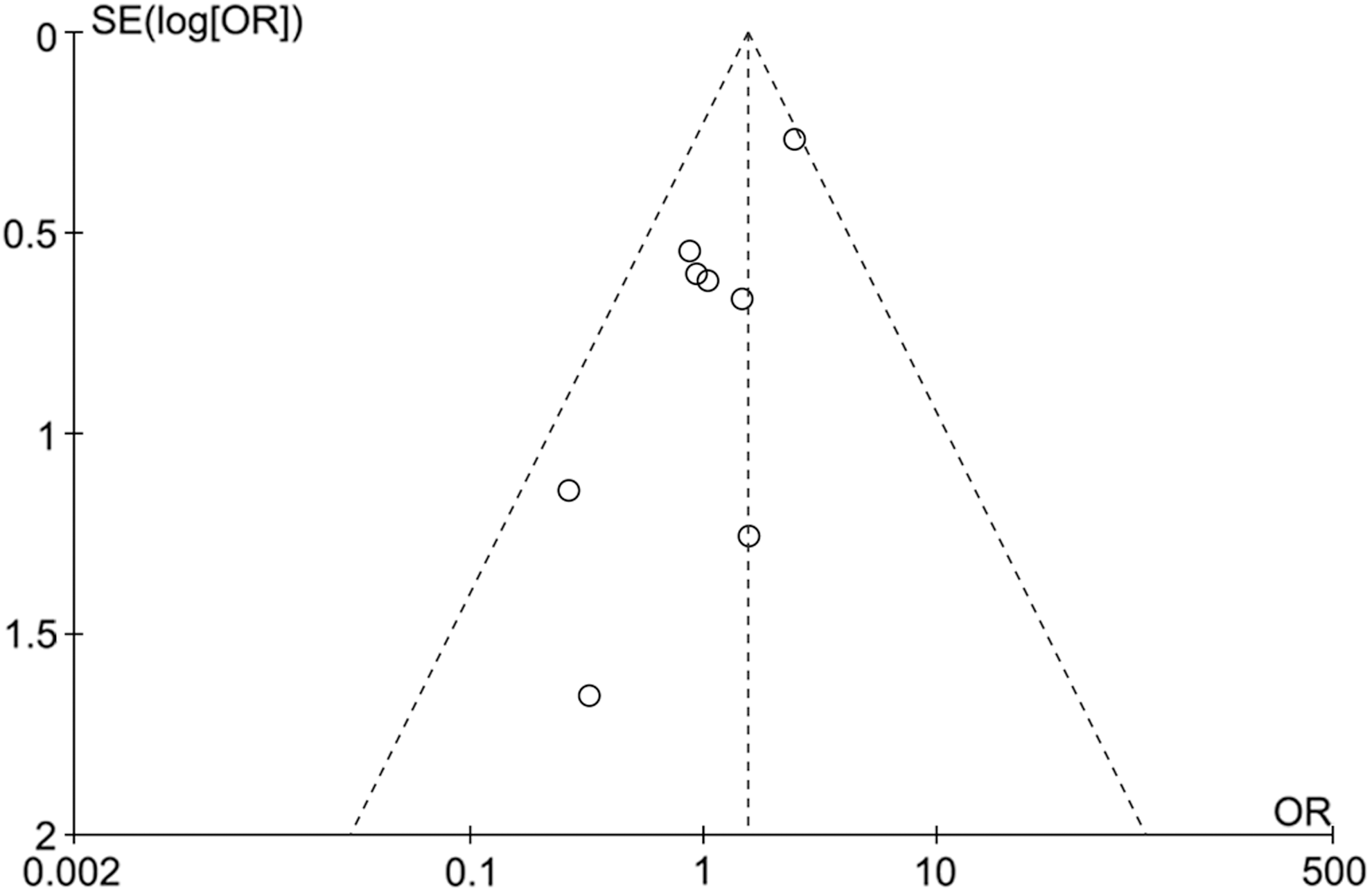
Funnel plot of blood transfusion.
Discussion
PN has gradually replaced the RN for the primary management of stage T1 renal tumors due to benefits regarding renal function and mortality. To minimize warm ischemic renal injury, early unclamping, 24 segmental renal artery clamping, 25 and the pure off-clamp technique have been developed. The pure off-clamp technique completely avoids ischemia–reperfusion injury; however, the safety and efficacy of OFF-PN are still uncertain.
This meta-analysis included 10 retrospective studies that compared perioperative and functional outcomes between OFF-PN and ON-PN. The results showed that OFF-PN had higher rates of transfusion, and lower rates of postoperative complication and positive margin than ON-PN, and that OFF-PN preserved superior postoperative renal function compared to ON-PN. Other outcomes of interest were similar between the groups.
According to our analysis, patients that received OFF-PN had an extra 60.7 mL blood loss (although this difference was insignificant) and a higher blood transfusion rate than those who received ON-PN. These results are expected, as there is continuous bleeding from the renal stump during OFF-PN, whereas the renal parenchyma is ischemic when the renal hilum is clamped. Given that adequate intraoperative visualization is essential for precise tumor resection and renal reconstruction, achieving adequate hemostasis at the tumor bed during OFF-PN has become the biggest challenge. Various feasible methods for hemostasis have been introduced in recent years, including the laser-assisted technique, 26,27 the sequential preplaced suture renorrhaphy technique, 28 the usage of a coagulator, LigaSure™, 29 homonic scalpel, 11 titanium clips, 6 and sutures 8 Electrocautery is the most common method and has been reported to not compromise pathological evaluation. 30 The present review did not compare the efficacy between those methods because of insufficient data for additional analysis. Therefore, the method of choice is mainly based on the surgeon's preference and experience. In addition, some urologists use controlled hypotensive anesthesia during the deeper part of resection, while the reconstruction is completed with normal pressure, 31 further improving the feasibility of the off-clamp technique.
The conversion rates were not significantly different between the two groups. During OFF-PN, clamping of the renal hilum is needed when excessive bleeding is encountered. 6,22 Thus, the renal artery is preisolated, and a vascular clip is preplaced to enable rapid hilar control. Moreover, when the bleeding is uncontrollable, a conversion to open surgery is necessary for patient safety during minimally invasive OFF-PN. 6,11,22,23
Before any new technique is widely applied, patient safety is primarily considered. In general, a bloodless operative field with clear visibility is related to fewer adverse events. 32 Surprisingly, our results showed that OFF-PN had a lower postoperative complication rate than ON-PN, and that the urine leakage rate was similar between the groups. This controversial finding could be explained by studies that reported complications based on different criteria without providing specific adverse events, 6,8 –11,22 which may result in bias. More importantly, tumor size and location are associated with an increased chance of complications. 33 Therefore, all outcomes of interest should have been compared based on the tumor size and location. Unfortunately, due to insufficient data, such analyses could not be performed. In a study by George et al., 6 OFF-PN was associated with a significantly lower postoperative complication rate compared with ON-PN (p=0.012). However, there was no significant difference when patients were stratified into endophytic and nonendophytic groups, indicating that selection bias may be responsible for this encouraging finding favouring OFF-PN. This finding, however, indicates that OFF-PN at least has comparable safety with appropriate patient selection.
Oncologic outcome is another main concern of surgeons and patients. OFF-PN had a lower positive margin rate, although the vast majority of patients with a positive margin would not experience tumor recurrence. 34 Wszolek et al. 8 reported that the 5-year cancer-specific survival for patients who underwent OFF-PN and ON-PN were 75% and 79%, respectively (p>0.05). Therefore, OFF-PN offers a comparable oncologic outcome but its effects on long-term survival will still require additional well-designed trials.
The better preservation of renal function is an apparent benefit of OFF-PN. Although estimating renal function changes through serum creatinine could be masked due to the functional compensation of the contralateral kidney, our meta-analysis still demonstrated that OFF-PN was associated with a decreased loss in renal function compared with ON-PN. Moreover, patients who underwent OFF-PN were half as likely to experience acute renal failure and only a quarter were likely to develop new-onset stage IV chronic kidney diseases (CKD) during a mean follow-up of 3.3 years, regardless of the lower pre-eGFR. 35 In addition, the reported follow-up period in the cohorts were from 6 months to nearly 5 years, 8,22 further indicating that both short-term and long-term favorable renal function preservation can be routinely achieved. This finding is particularly encouraging for specific groups, such as patients with solitary kidney, multiple tumors, renal insufficiency, or risk factors of CKD.
Larger (>4 cm) and endophytic tumors tend to increase the difficulty of PN, particularly when the renal pedicle is unclamped. In addition, unclamping increases the learning curve, especially for inexperienced surgeons. However, Rais-Bahrami et al. 22 found no differences in EBL, postoperative complication rate, and positive margin rate when outcomes were directly compared between unclamped and clamped T1b groups, despite tumors being more exophytic in the unclamped group. This provides evidence that the feasibility and safety of the off-clamp technique can be ensured in selected larger (>4 cm) tumors. In the present study, urologists preferred ON-PN rather than OFF-PN for the management of cT1b and endophytic tumors. Interestingly, when stratified by surgical approach, patients who underwent OFF-PN and ON-PN had tumors with comparable size and depth in the OPN subgroup. 8,9 Unfortunately, the efficacy and feasibility of the off-clamp techniques during OPN and minimized invasive PN for larger and complex tumors could not be compared due to insufficient data.
The presence of heterogeneity was detected in most of the continuous variables but not in dichotomous variables. Different study design, surgical approach and technique, and measurement of outcomes might be primary contributors to the heterogeneity. Therefore, the random-effects model was used to reduce the impact of heterogeneity, but could not completely eliminate it. To explore the source of heterogeneity, a sensitivity analysis for cohorts with comparable tumor size and location was performed. Although heterogeneity was not reduced, the difference of postoperative complication rate and positive margin rate became statistically insignificant, proving that selection bias could explain at least part of those differences.
To the best of our knowledge, this is the first systematic review and cumulative analysis comparing OFF-PN to ON-PN for the management of renal tumors. Our research was carried out at an appropriate time because this issue urgently needs to be resolved and sufficient clinical data have accumulated for analysis. In the present study, relying on the PRISMA, we strictly compiled with the predefined inclusion and exclusion criteria, carefully evaluated the quality of the included studies, and further performed sensitivity analysis to minimize the heterogeneity. Therefore, the validity and stability of our findings are ensured.
However, there are some limitations had to be taken into account. First, all included studies were retrospective. Inadequate random assignment and blinding tended to result in bias. Tumor location, the main factor influencing perioperative outcomes, is different between the groups, further indicating selection bias. Nevertheless, patient preferences and ethical concerns always make RCTs difficult to perform. Second, in some small series, the learning curve could not be ignored, which may influence the validity of the final result. Third, some studies presented continuous variables as median and range, probably because of its non-normal distribution characteristics. We calculated the mean and SD according to statistical methods, which may cause bias. Fourth, none of the included studies in our meta-analysis accounted for volume preservation. Since volume preservation is the primary driver of postoperative renal function, results would have been more accurate if volume preservation had been taken into account.
In conclusion, this meta-analysis indicates that OFF-PN is associated with a higher transfusion rate, comparable postoperative complication rate and positive margin rate, and superior renal function preservation. Given that inherent limitations in retrospective studies and the impact of patient selection bias may prevent definitive conclusions, future well-designed RCTs are required to confirm our findings.
Footnotes
Disclosure Statement
All authors have no financial conflicts of interest to declare.