
Abstract
Introduction:
The European Association of Urology (EAU) guidelines recommend to perform extended pelvic lymph node dissection (ePLND) in all patients with a risk of lymph node invasion (LNI) higher than 5% estimated by the updated Briganti nomogram. However, this model has been developed in patients exclusively treated with open radical prostatectomy. No study has specifically assessed the accuracy of this model among men treated with robot-assisted radical prostatectomy (RARP). We hypothesized that EAU indications for PLND are accurate also among patients treated with RARP.
Materials and Methods:
We evaluated 615 patients treated with RARP and PLND between 2006 and 2012 at a single tertiary referral center. The predictive accuracy of the nomogram was quantified using the receiver operating characteristic-derived area under the curve, the calibration plot method, and decision curve analyses.
Results:
Median of lymph nodes (LNs) removed was 9 (interquartile range: 6–13). The rate of LNI was 5%. External validation of the Briganti nomogram showed good accuracy (81.8%). A nomogram-derived cutoff of 5% would allow the avoidance of 75% of PLND at the cost of missing of 19.4% of patients with LNI. When the same analyses were repeated in men with at least 10 and 15 LNs removed, the 5% cutoff was associated with a reduction in PLND and with an LNI missing rates of 67.6% and 59.3% and 17.4% and 6.2%, respectively. Similarly, the prediction accuracy increased to 81.2% and 85.3%, respectively. The decision curve analysis showed an increase in the net-benefit in the prediction range between 2.5% and 54%.
Conclusions:
We report the first validation of the EAU guideline recommendation for PLND among patients exclusively treated with RARP. We demonstrated that the accuracy of Briganti nomogram is high, but the proposed 5% cutoff is valid only in the presence of adequate ePLND.
Introduction
E
Materials and Methods
We evaluated the data of 800 PCa patients treated with RARP and PLND at our institution by four surgeons between 2006 and 2012. Overall, 185 patients were excluded because of incomplete clinical and/or pathological information. These comprised 35 patients with an unknown prostate-specific antigen (PSA) level, 27 with unknown primary and/or secondary biopsy Gleason grade, 106 with unknown clinical stage, and 17 with an unknown LN count. These selection criteria yielded 615 assessable patients. Robotic PLND was performed in all patients regardless of their preoperative tumor characteristics. However, the anatomical extent was not standardized among surgeons. Not all patients indeed received an anatomically defined extended PLND. All patients received PLND, including removal of at least all lymphatic tissue in the obturator fossa and along the external iliac vessels. However, the additional complete removal of LNs along, medially and laterally to, the hypogastric vessels and along the common iliac vessels up to the ureteric crossing was based on the clinical judgment of each treating physician. The LN packages from each side were removed and sent for histopathological examination separately. A single dedicated uropathologist examined all PLND specimens for the presence of LNI.
Patient data included age, serum PSA level, clinical stage (T1 vs T2 vs T3), primary and secondary biopsy Gleason grade (categorized as ≤3 vs ≥4), percentage of positive cores (defined as the number of positive cores over the total number of cores taken), number of removed LNs, and tumor risk group according to the National Comprehensive Cancer Network (NCCN) guideline classification.
Statistical analyses
Descriptive statistics focused on frequencies and proportions for categorical variables. Medians and interquartile ranges were reported for continuously coded variables. Mann–Whitney and chi square tests were used to compare the statistical significance of differences in medians and proportions, respectively.
Our analyses consisted of different steps. First, we systematically assessed the sensitivity, specificity, positive predictive value, and negative predictive value of a range of nomogram thresholds from 1% to 10% to correctly predict histologically confirmed LNI. Second, we externally validated the nomogram using the predetermined regression coefficients. The discrimination accuracy of the model to predict LNI was quantified using the receiver operating characteristic-derived area under the curve, where 100% indicates perfect prediction and 50% is considered equivalent to the toss of a coin. The extent of overestimation or underestimation of the histologically confirmed versus the nomogram predicted LNI rates was explored graphically using a calibration plot. Third, we relied on decision curve analyses as described by Vickers and Elkin to evaluate the value of the Briganti nomogram. 26 Decision curve analyses examine the theoretical relationship between the threshold probability of a disease (LNI) and the relative value of false-positive and false-negative results to determine the value (net-benefit) of a prediction model. 26
All statistical analyses were performed using the Statistical Package for Social Science, version 15.0 (SPSS®, Chicago, IL) and R statistical package system (R Foundation for Statistical Computing, Vienna, Austria). All tests were two sided, with a significance level set at 0.05.
Results
Patient descriptive characteristics are shown in Table 1. The median patient age was 63.4 (interquartile range 58.4–68.4). The median PSA level was 6.3 ng/mL (interquartile range 4.8–9.0). Most patients had clinical stage T1 (68.3%), primary biopsy Gleason grade ≤3 (88.5%), secondary biopsy Gleason grade ≤3 (65.5%), and were classified as intermediate risk by NCCN guidelines (55.3%). The median number of LNs removed was 9.0 (interquartile range: 6.0–13.0).
Patients are classified according to LNI/status.
pN0=node negative; pN1=node positive; IQR=interquartile range; LNI=lymph node invasion; NCCN=National Comprehensive Cancer Network.
The rate of LNI was 5%. Patients with LNI had a higher PSA level (8.0 vs 6.2 ng/mL), higher tumor stage (T3: 16.1 vs 2.4%), higher tumor grade (primary biopsy Gleason grade ≥4: 51.6% vs 9.4%), higher percentage of positive cores (median: 50.0 vs 33.3), and a higher number of LNs removed (median: 15.0 vs 9.0) than their counterparts without LNI (all p<0.001). No significant differences were recorded according to LNI status for age, year of surgery, and secondary Gleason score (all p<0.05; Table 1).
In the first step of our analyses, we tested the performance characteristics of various thresholds for discriminating between patients with or without histologically confirmed LNI, and quantified the number of avoidable PLNDs versus the number of potentially missed patients with LNI (Table 2). In our population of 615 patients, 461 (75.0%) were classified below the 5% threshold. Accordingly, a PLND would have not been recommended in those patients by the most updated Briganti nomogram. Avoidance of PLND in those 461 individuals would have resulted in missing LNI in 6 patients (19.4% of all patients with histologically confirmed LNI, and 1.3% of all patients with avoidable PLND). For patients with Briganti nomogram-predicted risk of LNI below 5%, the most frequently observed characteristics were a PSA value of between 4.01–10.00 ng/mL (66.7%), clinical T1c stage (68.3%), primary biopsy Gleason grade ≤3 (88.5%), and secondary biopsy Gleason grade ≤3 (65.5%).
Percentage is indicative of specificity; bpercentage is indicative of one-sensitivity; cpercentage is indicative of one-specificity; dpercentage is indicative of sensitivity.
PLND=pelvic lymph node dissection; PPV=positive predictive value; NPV=negative predictive value.
In the second step of our analyses, we evaluated the predictive accuracy of the most updated Briganti nomogram in predicting pathologically confirmed LNI. 18,23 The discrimination of the nomogram was 81.8%. The calibration of the nomogram was virtually ideal for the prediction range between 0% and 10% (Fig. 1A). Noteworthy, 90.4% (n=556) of patients lied within this prediction range. Conversely, for the prediction range between >10% and 50%, the nomogram tended to underestimate the real LNI risk (maximum underestimation: 9.2%). Finally, for the prediction range >50%, the nomogram tended to overestimate the real LNI risk (maximum overestimation: 20.1%). When the same analyses were repeated in patients with at least 10 (278, 45.2%) and 15 (118, 19.2%) removed and examined LNs, the 5% cutoff was associated with a reduction in PLND of 67.6%, and 59.3%, respectively. This came at the cost of missing LNI in 17.4% and 6.2%, respectively (Tables 3 and 4). The prediction accuracy analyses (discrimination and calibration) of these two subcohorts are shown in Figure 1B and C.

European Association of Urology (EAU) guideline-based nomogram calibration plot in the overall patient population
Percentage is indicative of specificity; bpercentage is indicative of one-sensitivity; cpercentage is indicative of one-specificity; dpercentage is indicative of sensitivity.
Percentage is indicative of specificity; bpercentage is indicative of one-sensitivity; cpercentage is indicative of one-specificity; dpercentage is indicative of sensitivity.
The decision curve analysis showed that the nomogram was associated with an increase in the net-benefit in the prediction range between 2.5% and 54% (Fig. 2).
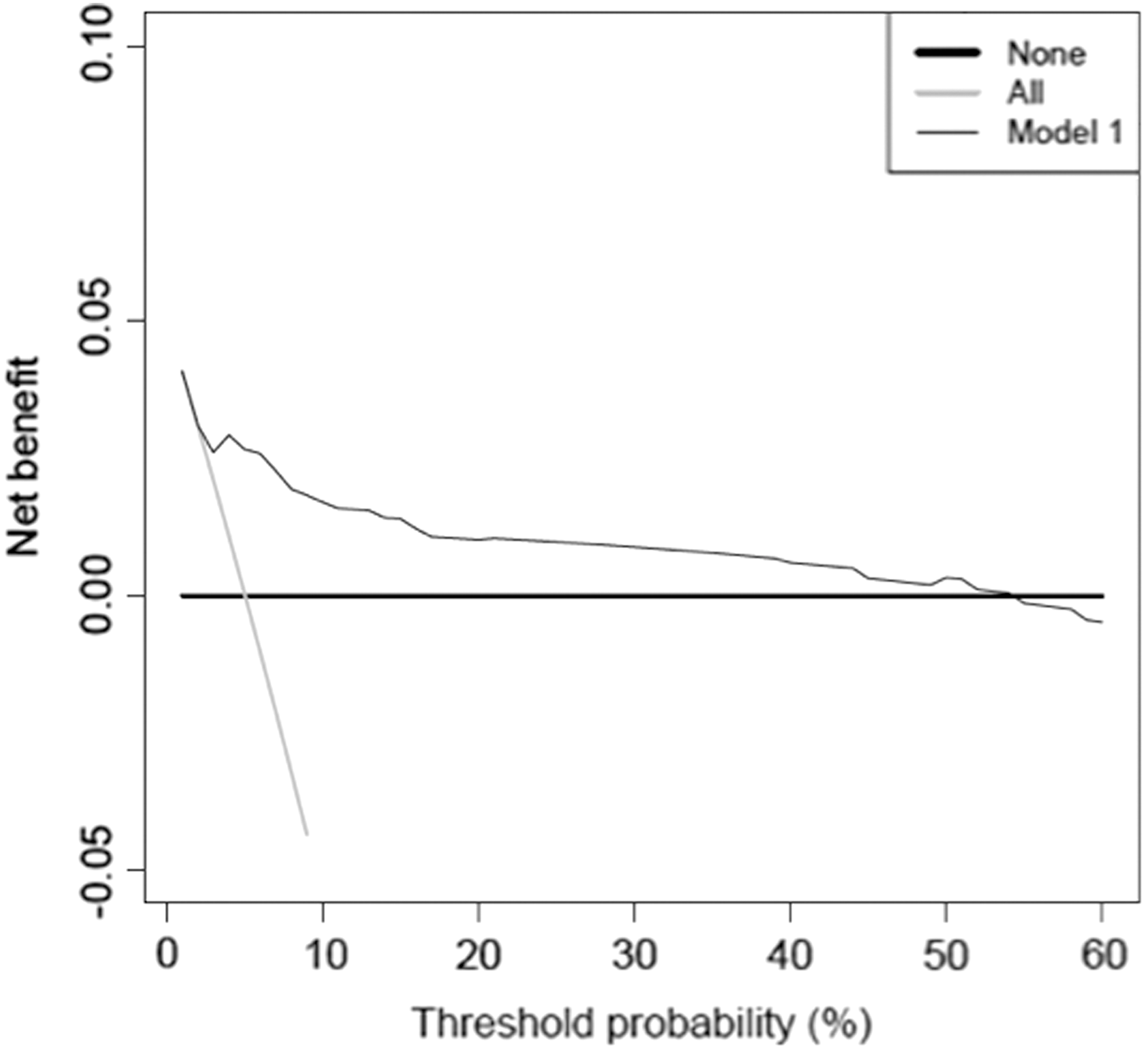
Decision curve analysis demonstrating the net-benefit associated with the use of the EAU guideline-based nomogram. Net-benefit can be interpreted as the proportion of all patients who have lymph node metastases and are recommended for extended pelvic lymph node dissection, if no patients with negative lymph nodes were treated.
Discussion
The most updated EAU guidelines recommend the use of the updated Briganti nomogram to decide the need for ePLND at RP. 23 This nomogram was developed using the data of 588 patients treated with open RP and anatomically defined ePLND. 18 Recently, two studies tested the performance characteristics of this nomogram in an external validation setting. 21,22 However, the vast majority of patients in these studies were also treated with open RP. In consequence, the findings of these reports cannot be directly applied to patients treated with RARP. As minimally invasive techniques are progressively overtaking open RP in the treatment of PCa, we set to perform an external validation of the most updated Briganti nomogram in patients treated exclusively with RARP.
Our results showed that in the entire cohort of 615 patients, 5% harbored LNI. According to the most updated EAU guidelines, the use of the 5% cutoff would allow the avoidance of PLND in about 65% at the cost of missing 12% of patients with LNI. However, in our cohort, the use of the 5% cutoff would have resulted in the avoidance of PLND in 75% of patients at the cost of missing 19% of patients with LNI. This suboptimal characteristic might originate from the difference in the number of LNs removed in RARP versus open RP. Specifically, in the current cohort, the median number of LNs removed was 9. Such number compares unfavorably to the number of nodes removed in open RP series. 18,21,22 This is key, since several reports have documented a direct relationship between the number of LNs removed and the detected rates of LNI. 27 –29 Taken together, it may be argued that the suboptimal extent of PLND in our cohort could have artificially undermined the performance characteristics of the Briganti nomogram. Indeed, when the analyses were limited to patients with at least 15 LNs removed, the use of the 5% cutoff resulted in the avoidance of PLND in 59% at the cost of missing only 6% of patients with LNI.
Nevertheless, the use of nomogram-generated threshold value in clinical practice can only be justified when the nomogram can correctly predict the real LNI risk. To address this issue, we tested the predictive accuracy of the Briganti nomogram in the second part of our analyses. The overall accuracy of the nomogram was 82%, and the calibration characteristics were virtually perfect in the prediction range ≤10%. It is of note that 90% of our patients had a nomogram calculated LN risk ≤10%. As such, one can expect that the predictions of the nomogram are optimal in the majority of patients seen in the clinical practice. When we limited our analyses to the subcohort of patients, with at least 15 LNs removed, the accuracy of the model increased to 85% and the calibration characteristics remained virtually the same. Again, this implies that the apparent underperformance of the Briganti nomogram might mainly stem from the fact that the majority of patients in this cohort received a suboptimal PLND.
The third part of our results relied on decision curve analysis. This method depicted the benefit of using the Briganti nomogram to predict LNI (and plan PLND) relative to the assumption that no patient harbors LNI (not performing PLND in any patient). The benefit here represents the potential increase in the true-positive results without increasing the number of false-positive results. Similarly, decision curve analysis can be used to calculate the advantage of using the Briganti nomogram relative to the assumption that all patients harbor LNI (performing PLND in all patients). The advantage represents the potential decrease in false-positive results without increasing the number of false-negative results (Fig. 2). Our decision curve analyses showed that the Briganti nomogram has a higher net benefit compared with not performing PLND in all patients in the prediction range between 2.5% and 54%.
Our results corroborate previous reports. For example, Gacci et al. 22 evaluated 896 patients who were treated with open RP and ePLND at two tertiary referral centers for clinically localized PCa. In their cohort, the use of the 5% cutoff proposed by the EAU guidelines would have allowed the avoidance of ePLND in 42% of patients, and the cost of missing 8% of men with LNI. The discrimination of the full model was 79%, and the calibration characteristics were equally favorable. Likewise, Hansen et al. 21 studied a total of 1282 patients who underwent either open RP or RARP for clinically localized PCa. The use of the 5% cutoff in this report would have allowed the avoidance of PLND in 56% of patients at the cost of missing 13% of patients with LNI. Moreover, they further confirmed that the predictive accuracy of the model was optimal. Specifically, the discrimination was 83%, with favorable calibration characteristics. However, only a minority of the patients included in the study by Hansen et al. received RARP. 21 Therefore, to the best of our knowledge, our study represents the first report that focuses exclusively on this set of patients.
The clinical implication of our report is that the Briganti nomogram can be reliably used to decide the need for ePLND in patients, who are candidates for RARP. However, the use of the 5% cutoff, to decide whether or not to perform PLND, can be used only if an ePLND is performed. This may stem from the fact that the number of LNs harvested during PLND is generally lower in patients treated with RARP in comparison to open RP. 30 –32 Nevertheless, given the fact that extended nodal dissection should be the only way to assess the real nodal status of men with PCa, the use of 5% cutoff remains valid for deciding the need for ePLND among RARP-treated patients.
Our study is not devoid of limitations. The main limitation of our report is the low number of patients with pathological LNs as well as the relatively low median number of LNs removed. As previously explained, this may be related to the fact that RARP negatively influences the extent of PLND. Moreover, in our study, the anatomical extent of PLND was not standardized among surgeons. In this series, the extent and the need for PLND was based on the clinical judgment of each treating physician. Given their low risk of nodal invasion, at least 60% of patients included in our series could have been spared any PLND. Furthermore, our cohort represents data from a single European institution. It remains to be tested whether our findings are representative of other cohorts. As such, an external validation of this predictive model in a multi-institutional cohort is warranted. Despite these limitations, our study represents the first formal validation of the Briganti nomogram in patients exclusively treated with RARP. Our report demonstrated that the model is highly accurate, but the proposed cutoff is valid only in men treated with more extensive PLND.
Conclusions
We report the first validation of the EAU guideline recommendations for ePLND among patients treated with RARP. Our results show that the model is highly accurate. However, the use of the 5% cutoff originally proposed by Briganti et al. in these individuals would have missed 20% of patients with LNI, instead of the 12% observed in the original report. Most probably, this stems from the limited PLND performed in these individuals. Indeed, the performance of the 5% cutoff improved progressively with the increasing number of LNs removed. Therefore, the use of EAU guideline recommendations in men treated with RARP is only valid in the presence of adequate ePLND.
Footnotes
Disclosure Statement
Alberto Briganti is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.