
Abstract
Purpose:
This study aims to provide an overview of type and frequency of musculoskeletal complaints among urologists. In addition, the urologists' knowledge about ergonomic conditions during minimally invasive urology was assessed, and they were asked how they would prefer to gain knowledge about this topic.
Materials and Methods:
An online and hard copy version questionnaire was administered to urologists from different countries, mainly from Europe, performing endourology and laparoscopy.
Results:
Of the 285 respondents, 245 (86.0%) urologists experienced musculoskeletal complaints in the past 12 months and 62.1% were considered to be work related. Most common areas for chronic complaints were neck, back, and shoulders. Almost 50% of the urologists experienced chronic musculoskeletal complaints, for which endourology (odds ratio [OR] 3.06; 95% confidence interval [CI] 1.37–6.80) and laparoscopy (OR 1.70; 95% CI 1.27–2.28) were significant risk factors. One third of the urologists considered their knowledge about ergonomics minimal, and 8% stated that they had no knowledge about these topics. Fifty percent of the respondents preferred to integrate information about ergonomic rules into hands-on training of urologic skills.
Conclusion:
High prevalence of experienced musculoskeletal complaints was found among urologists predominantly related to endourology and laparoscopy. Urologists indicate that they have a lack of knowledge about ergonomics in the operating room. Hence, we recommend integration of ergonomics in hands-on training programs early in the residency curriculum to gain knowledge and awareness and hopefully to offer possibilities to prevent these complaints in the future.
Introduction
M
Advantages of minimally invasive surgery are well known; patients experience less postoperative pain, shorter hospital stay, and better cosmetic results. 2 On the other hand, urologists who practice minimally invasive surgery have to operate in an environment that is completely different compared with open surgery in terms of freedom of movement. For example, laparoscopic surgery often necessitates a nonoptimal posture, in which the surgeon has to work with abducted shoulders and to stand in a static posture for a long time. 2
Surgeons' disadvantages of minimally invasive techniques are becoming increasingly known, and studies have been conducted to evaluate musculoskeletal problems experienced by surgeons practicing minimally invasive surgery. 3 –7 Most studies resulted in a strong association of physical constraints with laparoscopy. Discomfort in neck, shoulders, and back were most frequently reported by surgeons as symptoms because of minimally invasive surgery. 7 –9
Gofrit and associates
5
reported also hand, wrist, and finger pain from hand-assisted laparoscopy. Only a few studies have been performed among urologists,
3,5
and little is known about the physical well-being of urologists practicing endourology. Moreover, with the rapid development of new minimally invasive techniques, it is of major importance to increase awareness of ergonomic guidelines—for example in training programs—and thus prevent the occurrence of musculoskeletal problems at an early stage. The science of ergonomics analyzes these challenges and formulates guidelines for creating a work environment that is safe for the surgeon and the operating team. Ergonomics is defined as “the scientific discipline concerned with the understanding of interactions among humans and other elements of a system, and the profession that applies theory, principles, data, and methods to design in order to optimize human well-being and overall system performance” (
In this study, we investigated the following research questions: (1) If urologists report musculoskeletal complaints, what type and frequency are most common? (2) To what extent do urologists consider their knowledge about ergonomic conditions during MIU? (3) What is the preferred method of gaining knowledge about ergonomics according to the opinion of urologists?
Materials and Methods
Questionnaire
An online questionnaire was developed in collaboration with an ergonomist (RHM) for the purpose of this international study on musculoskeletal complaints experienced by urologists (Supplementary Survey available online at
The questionnaire consisted of four parts. The first part contained 10 questions about general endourology and/or laparoscopy, general medical history, and whether physical complaints were experienced during the past 12 months. Endourology was defined as transurethral resection of the prostate, transurethral resecton of bladder tumor, ureterorenoscopy, percutanous nephrolithothomy. Medical history was predefined as neck hernia, back hernia, joint complaints because of a traumatic event, rheumatic disease, scoliosis, and an open section for other pathology in the medical history of the musculoskeletal system. The second part contained three specific questions for endourology—e.g., workload, physical discomfort, the occurrence of chronic complaints that are attributed to endourology and if the urologist ever reported absence of work because of the experienced chronic physical problems.
The third part contained the same questions specifically for laparoscopy. Chronic complaints were defined as musculoskeletal problems, which are experienced 6 months or longer. The fourth part consisted of three questions to assess how urologists consider their knowledge regarding optimal ergonomic conditions for MIU, whether they consider knowledge about ergonomics in urologic procedures important, and how they prefer to gain knowledge on this topic. All respondents were asked to rate their knowledge regarding monitor adjustment, table height, and body posture on a scale of 1 to 5, where 1 is “no knowledge,” 2 is “little knowledge,” 3 is “moderate knowledge,” 4 is “good knowledge,” and 5 is “excellent knowledge.”
Most of the questions were of a closed format, except for numeric answers such as age, hours of practice per week, and years of practice as urologists. Answer options included rank listing and 5 point Likert scales. The questionnaire ended with extra space to give suggestions for gaining knowledge or any other remarks.
Study population
Inclusion criteria were that the participants had to be urologists, performing endourology or laparoscopy or both procedures. Urologists who perform robot-assisted laparoscopy, retired urologists, residents, and nurse practitioners were excluded from the study. The online questionnaire was sent to all urologists in the Netherlands from September until November 2009. In addition, a link to the online questionnaire was published in European Urology Today (EUT), the newsletter of the European Association of Urology (EAU) in January 2010. Also, we approached urologists personally to fill in the online questionnaire or a hard-copy version of the questionnaire during the EAU Annual Congress in Barcelona in 2010. For the online questionnaire, “cookies” were activated, so urologists could not respond more than once. Participants recruited during the Congress were excluded if they already responded to the online questionnaire.
Data analysis
Logistic regression analysis was used to investigate whether the occurrence of musculoskeletal problems was associated with age, medical history, workload, hours of endourology per week, and hours laparoscopy per week. The data obtained from the questionnaire were analyzed using SPSS version 19.0. The cutoff point for statistical significance was set at a P value of 0.05.
Results
A total of 285 respondents completed the questionnaire. A total of 134 Dutch urologists responded to the electronic questionnaire. The European response on the link in the EUT was 57, which was increased with 94 completed questionnaires during the EAU Annual Congress.
Demographics
Table 1 shows the general demographics. One hundred and five respondents exclusively performed endourologic procedures and 180 urologists performed both endourology and laparoscopy. Mean hours per week spent on endourology were 8.41 hours (standard deviation [SD] 5.98). Mean hours per week spent on laparoscopy was 6.45 hours (SD 8.61).
SD=standard deviation.
Musculoskeletal complaints in the past 12 months
We focused on eight body regions for the purpose of our study: Neck, back, shoulders, arms, wrists, hands, thumbs, and legs. 3,5 –7 Of the 285 respondents, 245 (86.0%) urologists experienced musculoskeletal complaints in the past 12 months. For each of the body parts, Figure 1 shows the percentages of respondents who experienced musculoskeletal complaints of a certain level in the past 12 months, the levels varying from no complaints, to mild, moderate, serious, and severe complaints.
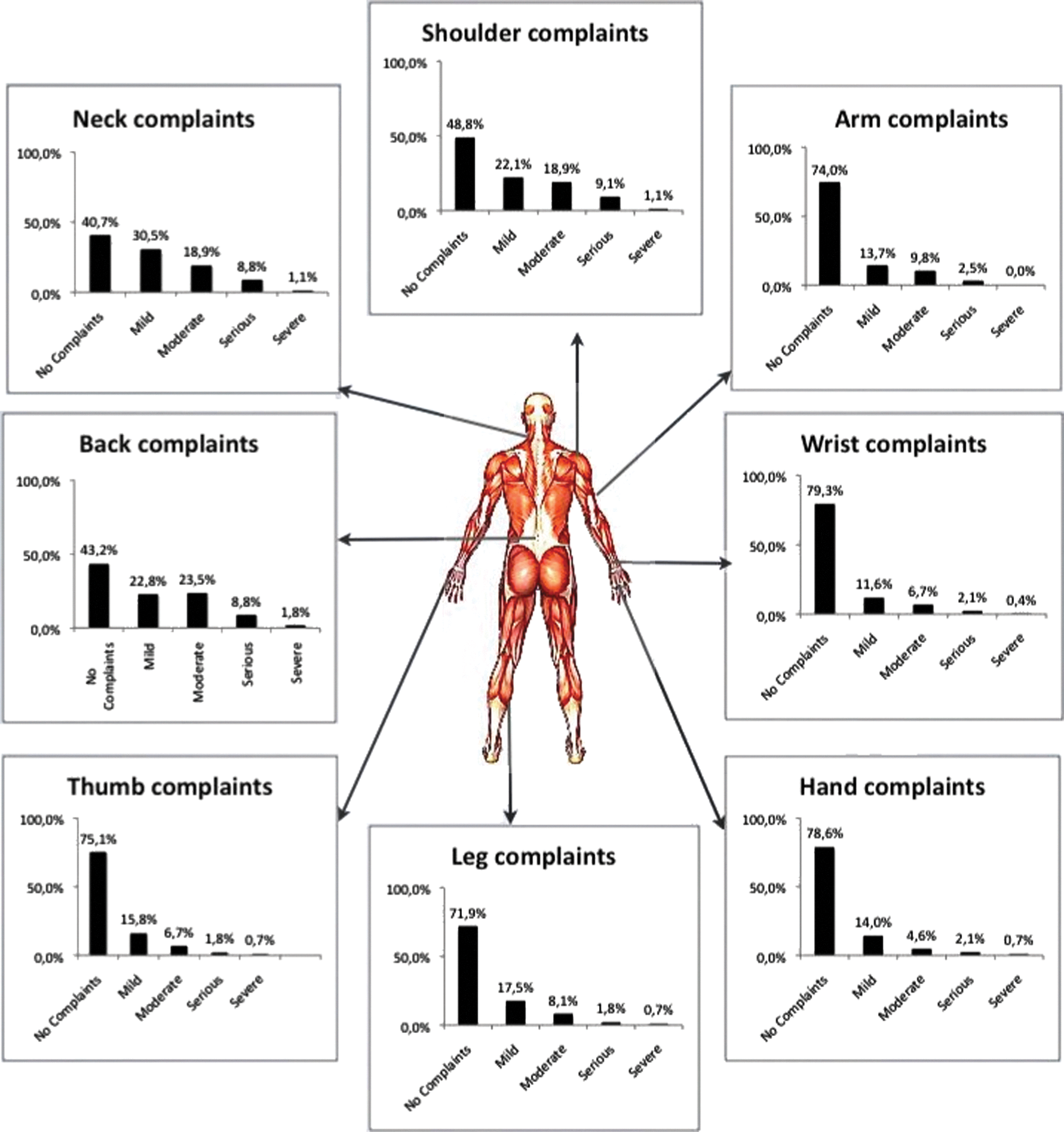
Musculoskeletal complaints experienced in the past 12 months.
Age and medical history were shown to be significant risk factors for reporting musculoskeletal complaints in the past 12 months. An increase of age was associated with a decrease of the risk for complaints (odds ratio [OR]=0.94 per year, 95% confidence interval [CI] 0.90–0.98), and having a medical history increased the risk (OR=3.62, 95% CI 1.34–9.77). For neck (OR=2.03, 95% CI 1.73–3.50), back (OR=2.17 95% CI 1.27–3.72), and arms (OR=1.76: 95% CI 1.01–3.07), only medical history was a significant risk factor.
When body regions were analyzed isolated, number of hours per week spent on laparoscopy resulted in being a significant risk factor for reporting problems in thumb (OR=1.66, 95% CI 1.18–2.33) and shoulder (OR=1.34, 95% CI 1.01–1.77). For leg problems, number of hours spent on laparoscopy per week (OR=1.52 95% CI 1.09–2.11) and medical history (OR=2.06: 95% CI 1.18–3.60) were both significant risk factors.
One hundred and seventy-seven (62.1%) urologists explicitly considered their complaints work related. Figure 2 shows the number of urologists who experienced musculoskeletal complaints and if they consider the complaints as a result of endourology, laparoscopy, or both procedures.

Reported musculoskeletal complaints (MC) in the past 12 months.
Chronic musculoskeletal complaints
One hundred and thirty-nine (48.8%) urologists experienced chronic musculoskeletal complaints. Most common areas for chronic complaints were neck, back, and shoulders. Endourology (OR 3.06; 95% CI 1.37–6.80) and laparoscopy (OR 1.70; 95% CI 1.27–2.28) were both significant risk factors for the development of chronic musculoskeletal problems.
From this sample of 124 urologists who performed both laparoscopy and endourology, 19 (10.6%) urologists attributed their chronic musculoskeletal complaints to endourology, 32 (17.8%) urologists attributed their complaints to laparoscopy, and 50 (27.8%) urologists thought they were because of both types of surgery.
Table 2 shows sick reports from musculoskeletal problems attributed to endourology and to laparoscopy.
Urologists' perception of their knowledge about ergonomics in MIU
Although 256 (89.8%) urologists indicated that ergonomics is important in urologic practice, they considered their knowledge mainly little, moderate, or good (Table 3). Eight percent of the urologists reported that they did not have any knowledge regarding monitor adjustments, table height, and body posture.
Forty-eight percent of all respondents preferred to integrate ergonomic rules into hands-on training sessions for MIU compared with 27.9% who preferred to follow training on ergonomics specifically (Fig. 3). Two respondents emphasized the importance to educate residents about ergonomics in the operating room. Another urologist suggested that program directors should give attention to ergonomic rules in the operating room to their residents before starting the procedure. Several urologists suggested a combination of all methods to gain knowledge about ergonomics. Another urologist suggested inviting an ergonomic specialist to give personal advice.
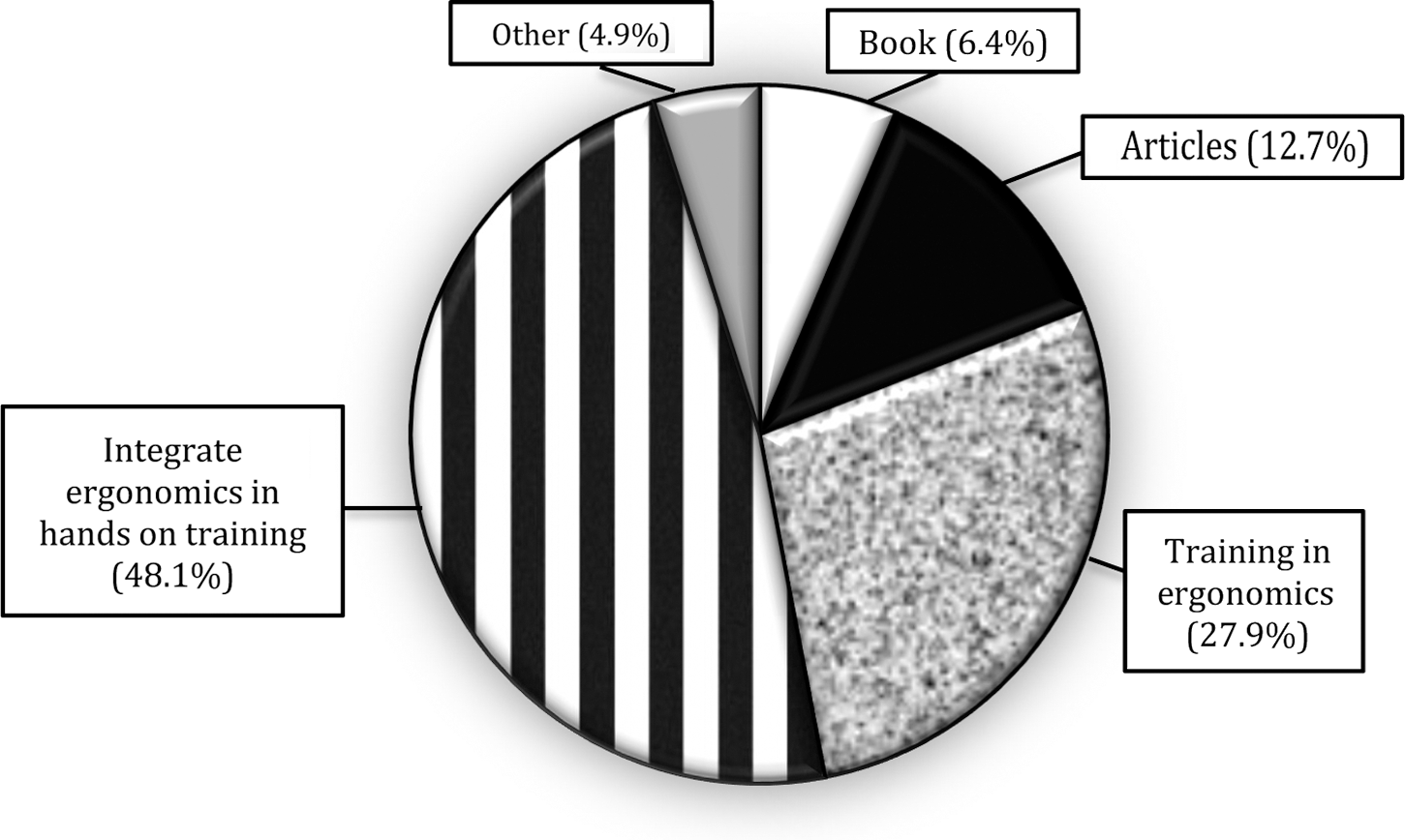
Urologists' preference to gain knowledge about ergonomics in the operating room.
Discussion
More than 85% of the urologists experienced musculoskeletal complaints in the past 12 months. Endourologists claim to experience musculoskeletal complaints almost in the same amount as laparoscopists, indicating that MIU in general could be a risk factor for development of musculoskeletal complaints.
The response rate of 285 urologists in this study is the largest sample survey found in the literature about ergonomics in urology, and the authors consider the results of current study representative for the experienced musculoskeletal problems among urologists.
Sixty-two percent of the urologists considered their complaints work related; however our study did not find evidence that total hours per week performing endourology was a significant risk factor for reporting musculoskeletal complaints within 12 months. Laparoscopy was associated with thumb, shoulder, and leg problems. The discrepancy between statistical outcome and the urologists' opinions could be explained by the fact that case load and especially mean hours per procedure are probably more important variables than total hours per week. 6
When compared with other occupations, our findings for neck (59.3%) and shoulder (51.2%) complaints were higher than reported for light workload employees (44% and 42% respectively)—i.e., administrators, service and sales workers—and interestingly also for heavy workload employees (39% and 43%, respectively)—i.e., agriculture workers, fishery workers, and trade workers in New Zeeland. 11,12 From the perspective of general occupations, this form of surgery can thus be considered as one with heavy workload. When compared with similar studies assessing musculoskeletal complaints from minimally invasive surgery, our results are consistent. 3,7,9,13,14 Comparison with other studies based on questionnaires should be interpreted with caution because of its subjective character; however, it appears that urologists have a seriously demanding workload for the neck and shoulder region. 2,6,7,10,12,15,16
Age and medical history—for example, rheumatic disease, back hernia, neck hernia, and scoliosis—appeared to be significant risk factors for development of musculoskeletal complaints. Younger urologists appeared to be more at risk to develop musculoskeletal complaints than the older urologists. This could be explained by the fact that younger urologists are less experienced and endure more muscle tension during their learning curve for endourology and laparoscopy. This corresponds with the findings of Sari and coworkers. 8
A recent study of Nieboer and associates 17 found evidence that short-term training of the nondominant hand during 3 weeks resulted in a better performance of the dominant hand when performing simple laparoscopic tasks in a box-trainer, because of the “intermanual transfer of motor skills” phenomenon. 17 Training of the nondominant hand did not show a decrease in tension of the shoulder and neck muscles. 18 Future studies are recommended to investigate if long-term training in a skills laboratory has a reducing effect on muscle tension, because, hypothetically, more experience in a certain skill results in less stress and muscle tension.
Szeto and colleagues 7 showed that 35.6% of the surgeons reported to “work through pain so that the quality of their work would not suffer.” As a consequence, musculoskeletal complaints could result in chronic problems and loss of quality of care, quality of urologists' life, and even to absence of work. The denial of pain should be taken seriously because sick absence attributed to musculoskeletal complaints does occur among urologists, which are confirmed by current study results. No firm evidence has been found in the literature for the consequences of muscle fatigue in per- and postoperative outcomes 3 ; however, patient safety, urologists' quality of life, and economic constraints because an urologist who is not able to perform surgery or from sick absence should definitely be taken into consideration.
Preferably, we recommend methods to prevent these musculoskeletal problems. In the past decennia, extensive ergonomic studies have been conducted to optimize instruments and to develop guidelines for laparoscopic surgery. 19 –22 Several studies have shown that instrument handles do not fit all hand sizes. Surgeons with a smaller surgical glove size (5.5–6.5) needed hand treatment more often and experienced more musculoskeletal complaints compared with surgeons with a larger size. 23 –25 To narrow the gap between users and product designers, a variety of surgeons with different statures and features should be involved in the development process of endoscopic instruments.
Table height is defined as the distance from the tabletop to the floor. 26 Berguer and associates 27 recommended a table height of 5 cm below elbow height, with an acceptable range of 12.5 cm below to 2.5 cm above elbow height for open surgery. These recommendations, however, are not sufficient for laparoscopy because of the length of the laparoscopic instruments, and because of the raise of the patients' abdomen from the pneumoperitoneum. The recommended optimum table height: When the instrument handles are at elbow height with a range of 10 cm below elbow height. 27 This corresponds with a table height of 64 to 77 cm above the floor.
Considering monitor placement, it is suggested that monitors should be placed straight in front of the viewer in line with the forearm instrument, avoiding axial rotation of the neck and back. The head should be slightly flexed at an angle of 15 to 30 degrees downward. 22,26
The ideal body posture for a laparoscopic surgeon is standing in a neutral position, the arms are slightly abducted, retroverted, and rotated inward at shoulder level. 22,26 The elbows are bend at about 90 to 120 degrees, the wrists are slightly extended, and the hands are completely relaxed. 28
The recommended monitor height and body posture, however, are assumed to be the same for endourologic procedures as for laparoscopic procedures; ergonomic guidelines for endourologic procedures are not yet established as they are for laparoscopic procedures.
Previous studies already acknowledged unawareness of ergonomic guidelines among surgeons, 10 and our study results show only slightly better results. Surprisingly, almost 25% of the urologists claimed to have little knowledge about ergonomic rules, and 8% of the urologists reported to have a total lack of knowledge considering ergonomics. Nevertheless, the majority of all respondents (89.9%) were willing to improve ergonomic awareness, preferably by integrating ergonomics in hands-on training. Hence, we have to search for strategies to collaborate ergonomists and urologists to transfer this knowledge and guidelines into urologic practice. The authors therefore recommend introducing methods that increase ergonomic awareness among program directors to teach their residents in the operating room and to incorporate ergonomic rules into hands-on training programs in skills laboratory.
In addition, robot-assisted surgery should be taken into account. This type of surgery offers significant advantages in terms of physical ergonomics for the surgeon who sits comfortably in front of the master console working with tool handles that offer more degrees of freedom, compared with conventional laparoscopic instruments. The robot, however, amplifies range so there is no need for twisting hands and stretching arms and shoulders in uncomfortable positions. 29
A limitation of this study is that it relies on self-reported data instead of physical examination. To investigate the exact musculoskeletal complaints and whether these can be attributed to urologic practice, long-term follow-up with measurement of muscle tension should be conducted in future studies.
The second limitation is that we did not include robot-assisted laparoscopy, hand-assisted laparoscopy, single-site laparoscopy, and natural orifices translumenal endoscopic surgery, open surgery, and residents. It would be interesting to investigate if the self-reported musculoskeletal complaints are solely from laparoscopy and endourology or if other types of surgery also lead to these musculoskeletal complaints.
Differences between hospitals in each country can be found. 6 Many operating rooms differ in their armamentarium for urologic procedures. Examples are direct-view scopes or video assisted scopes for transurethral resection, movable or no-movable monitors, and performing resections in standing or sitting position. In our study, this may have led to underreporting of physical complaints of urologists who still depend on nonergonomic devices. Future studies should focus on the current setups of operating theaters and the association of that setup with musculoskeletal problems.
Conclusion
This study showed a high prevalence of musculoskeletal complaints among urologists who perform endourology and laparoscopy and a lack of knowledge about ergonomic rules. In concordance with our findings, we underline the importance to improve ergonomic awareness and to involve ergonomists in the development of urologic skills training to incorporate knowledge of surgeon safety with patient safety in the early phase of urologic practice.
Footnotes
Acknowledgments
The authors would like to thank all urologists who responded on the questionnaire. The authors would also like to thank Mereke Gorsira for her editorial assistance.
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.