
Abstract
Background and Purpose:
An increase in the prevalence of urologic stone disease and the refinement of endourologic techniques has seen a concomitant rise in the use of fluoroscopy during surgery. As such, there has been increasing concern in regard to the intraoperative radiation exposure to both clinicians and patients. The objective of the study was to audit contemporary data on radiation exposure during percutaneous nephrolithotomy (PCNL), in comparison with published series, and demonstrate that relatively low levels are achievable with clinical vigilance and attention to technique
Methods:
A retrospective analysis was performed of all PCNLs undertaken between July 2005 and December 2011. The primary outcome measure was fluoroscopy times and associated radiation exposure, measured as dose area product (DAP). No statistical analysis was undertaken.
Results:
Between July 2005 and October 2011, 376 PCNLs were performed. Data were available on 348 patients including 16 pediatric patients. Mean DAP and screening time (ST) over the whole study period were 45 cGy/cm2 and 96s, respectively. On a year by year basis, the ST and DAP reduced from 917 to 375 and from 180 to 65, respectively. We acknowledge the limitation of this being a retrospective case series.
Conclusions:
This study represents the largest series to date on radiation exposure during PCNL and compares favorably with other published series, including those purporting novel techniques. Subtle changes in surgical technique and experience over time can lead to low screening times and can be potentially achieved by all operators performing PCNL within a high throughput center. It is now recognized that surgical outcome in stone surgery is related to caseload. The radiation dose the patient receives during PCNL is increasingly recognized to be an important factor and can be reduced by careful technique and experience.
Introduction
A
We evaluated the fluoroscopy times and associated radiation exposure, measured as dose area product (DAP), for PCNLs performed between 2005 and 2011.The objective was to quote contemporary data on radiation exposure during PCNL and to demonstrate that relatively low levels are achievable with clinical vigilance and attention to technique.
Methods
Retrospective data analysis was performed from a single tertiary referral center on all PCNLs undertaken between July 2005 and December 2011. All procedures were performed by two experienced consultant urological surgeons with previously published outcome data. 2,3
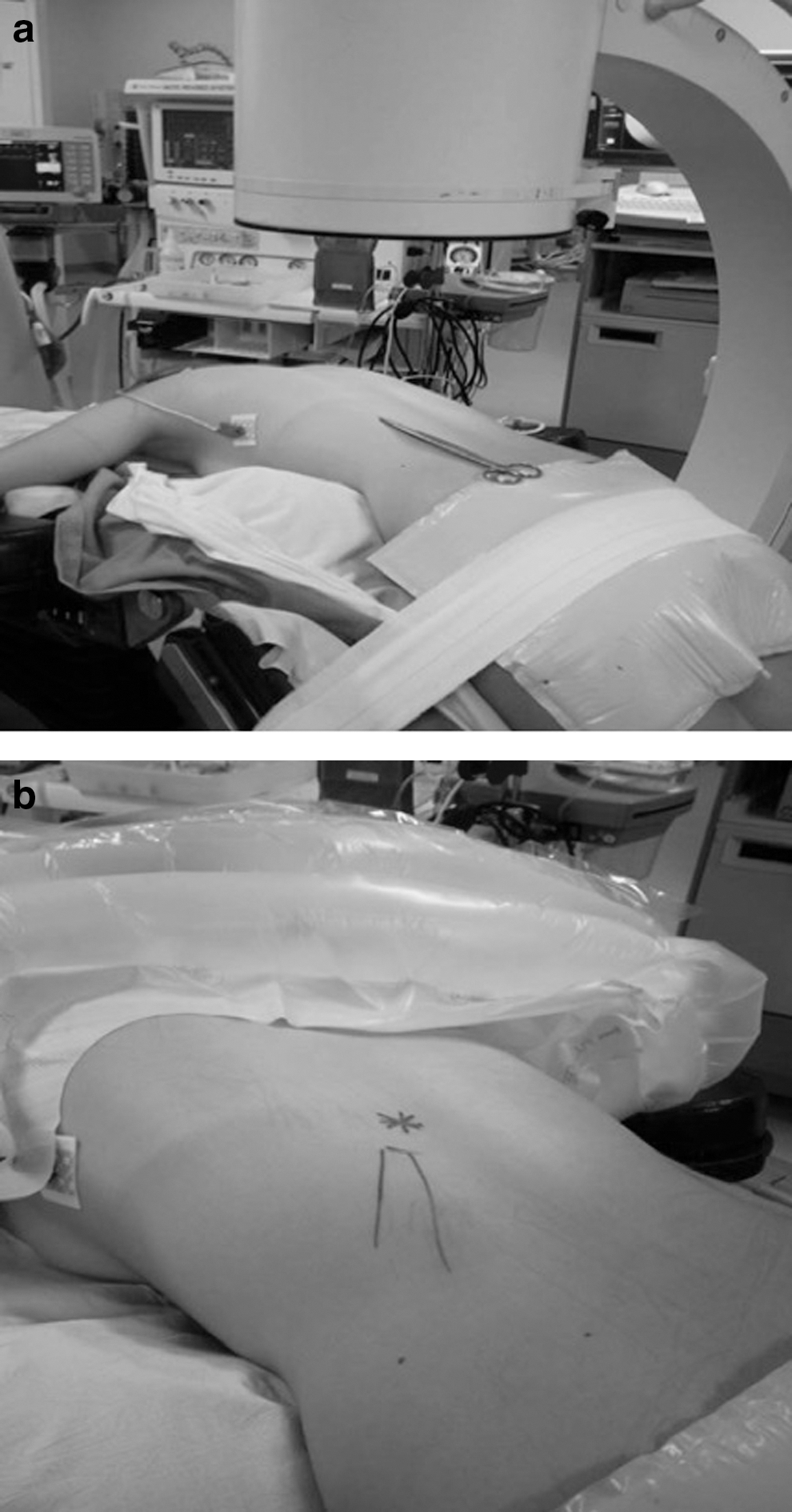
A ureteral catheter was placed at the start of the procedure without fluoroscopy. PCNL was performed with the patient in the prone flexed position with percutaneous access obtained by the urologist under fluoroscopy using a Siemens ARCADIS Varic™ image intensifier, with a diaphragm collimator and a fully digital imaging chain transmitted to an HD flat panel monitor. Collimated fluoroscopy was controlled by the radiographer. A quantitative assessment of radiation from fluoroscopy was documented as screening time (ST) in seconds, and DAP in Gy/cm2.
The position of the stone with relation to skin surface was marked before and after the retrograde instillation of contrast. A Kellett™ needle was utilized for the initial puncture and access achieved using either semirigid, serial dilatators or the Nephromax™ (Boston Scientific) balloon system. A prolonged attempt to access the ureter with a safety wire was not routinely performed.
The radiation dose can be assessed by fluoroscopy time, DAP, or effective dose (ED). DAP reflects not only the dose within the radiation field but also the area of tissue irradiated. It is easily measured, expressed in Gy/cm2, via a DAP meter on fluoroscopy equipment. ED refers to the amount of radiation absorbed by a patient, weighted for tissues exposed, and links it to the risk of a subsequent malignancy developing. The unit for effective dose is the sievert. Where multiple tissue types are exposed, this requires complex calculation and conversion tables or the use of a like-for-like anthropomorphic phantom model. 4 Conversion of DAP to ED has been shown to underestimate radiation exposure. 5,6
Results
Between July 2005 and October 2011, 376 PCNLs were performed. Data were available on 348 patients including 16 pediatric cases. Mean DAP and ST over the study period was 452 cGy/cm2 and 96 sec, respectively. On a year by year basis, the ST and DAP reduced from 917 to 375 and from 180 to 65, respectively (Table 1/Fig. 1).
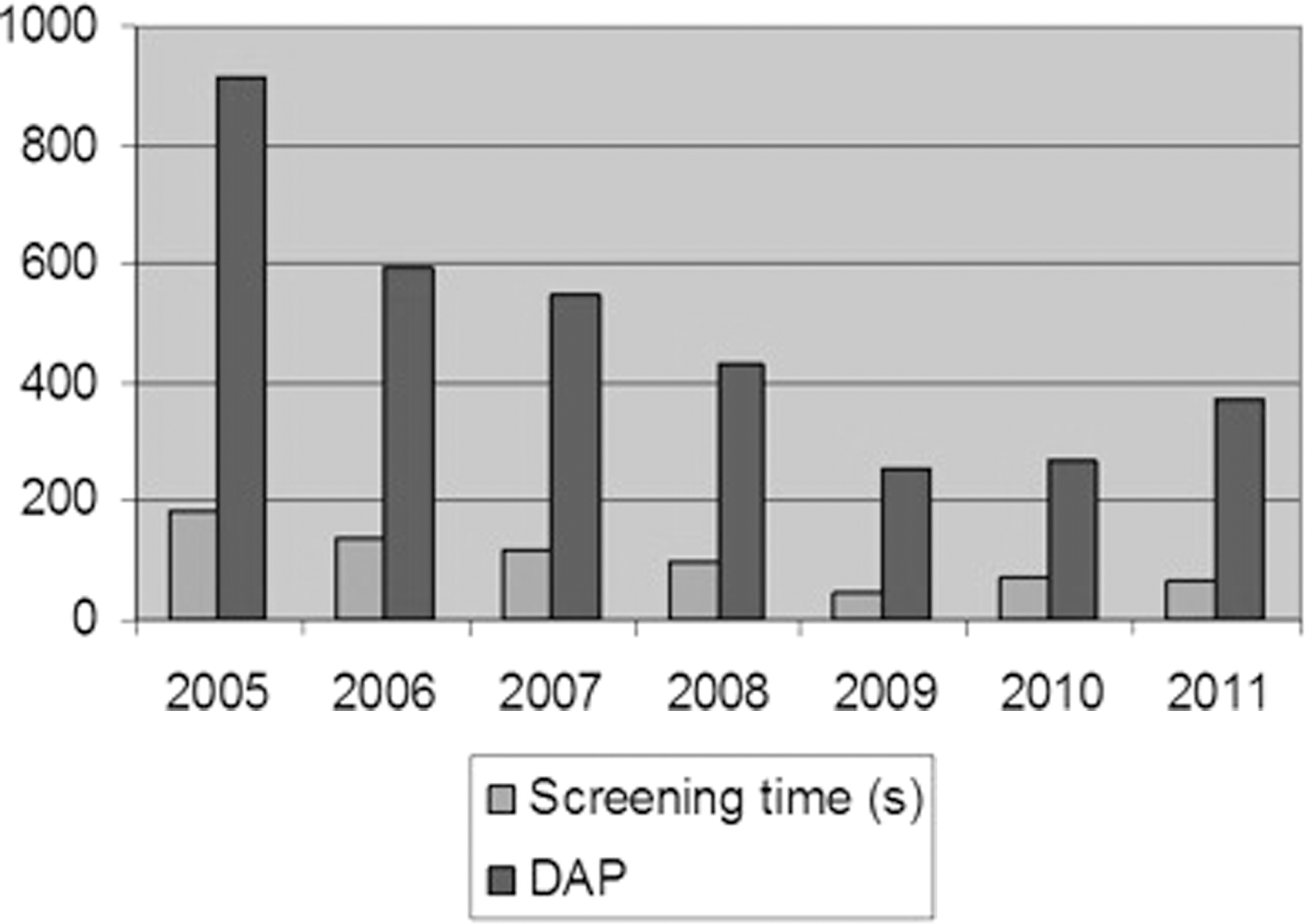
The trend in mean dose area product (DAP) and screening times for the 348 percutaneous nephrolithotomies over time.
DAP=dose area product.
A total of 156 females and 192 males were involved in the study. The average age of the study group was 52.79 years old. Data on stone size were available for 289/332 adult patients (Table 2).
n=number of patients; PCNL, percutaneous nephrolithotomy.
Data on body mass index (BMI) were not available, but the population is predominantly inner city with significant comorbidity and obesity.
Regression analysis was performed on patients treated with single stones. There were 185 total patients analyzed; results of their STs (Fig. 2) and stone size (Fig. 3) are graphically demonstrated. An analysis of variance test was performed demonstrating significant reductions in flouroscopy time over the study period (F=8.8, P=0.003).

Screening times of solitary stones managed between 2005 and 2012.
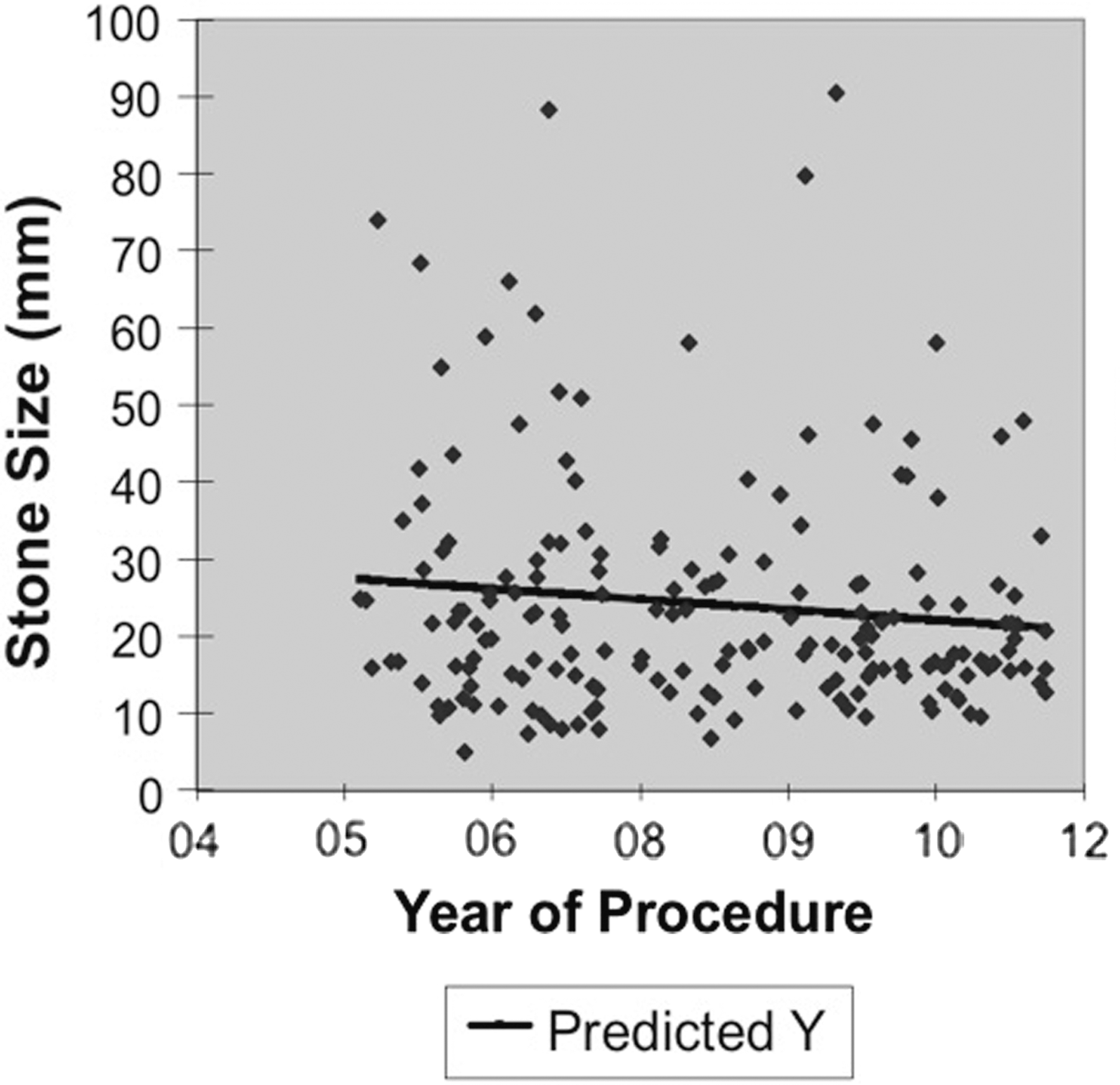
Stone sizes of solitary stones managed between 2005 and 2012.
There was a trend to reduction in stone size over this period, although this was not statistically significant (F=2.8, P=0.1). This suggests that ST was decreasing independent of the stone size managed.
Discussion
The prevalence of kidney stones is increasing and has recently been reported to be as high as 8.8%. 7 Concomitantly, there has been a significant increase in the number of surgical procedures undertaken for stone disease. Recent analysis of UK hospital episode statistics (HES data) has demonstrated an approximately 150% rise in the number of PCNLs performed per year between 2006 and 2010, 1 and there has been increasing discussion about intraoperative radiation exposure to both clinicians and patients.
Recent data from the United States has shown that the annual per capita radiation exposure from medical sources has increased from 0.54 mSv in 1980 to 3.0 mSv in 2006. 8 The International Commission on Radiological Protection recommends a limit of occupational dose exposure to 20 mSv/year over 5 years, with no more than 50 mSV in 1 year. Public exposure is limited to 1 mSv in a year.
Patients with higher BMI, stone burden, nonbranched stones, and multiple tracts are at increased risk of radiation exposure. 9,10 The proposed mechanism for this in obese patients is thought to be because of the automatic increase in the C-arm's tube voltage to maintain image quality. For staff, radiation scatter, rather than direct exposure, is the concern, with the surgeon receiving the maximum dose, the assistant less so, and the theater nurse being relatively unexposed. 11,12 A recent attempt to quantify organ-specific dose in a small series of 20 nonobese males demonstrated the highest radiation dose was to the skin surface bilaterally with localized differences in organ-specific dose. On the left side, the dose decreased from stomach, transverse colon/pancreas, and spleen to left kidney. On the right side, the gallbladder, liver, and right kidney received the highest doses. 4
The risks of radiation include induction of cellular DNA damage, which may cause cell death or potential DNA mutation. Even an exposure of 10 mSv of radiation can increase the lifetime risk (age and sex adjusted) of fatal cancer by 3%. 13 Data from the Radiological Society of North America suggests that the 20 mSv received by the surgeon during a year's PCNL workload has between a 1 in 1000 to 1 in 10,000 lifetime risk of causing a fatal cancer. 14 This increase has to be taken in the context of the background 1 in 5 lifetime risk of a malignancy developing in the general population.
The principles of as low as reasonably achievable that include collimating the image and pulsed fluoroscopy have been shown to reduce exposure in the pediatric population and are directly transferrable to adult patients. 15
Novel techniques such as the use of air nephrograms and endoscopic guided PCNL have been shown to reduce radiation dose and fluoroscopic time. A retrospective review of 92 patients in which PCNL access was achieved with the use of air nephrograms rather than with iodinated contrast showed an approximately 50% reduction in radiation exposure. 16 As with obese patients, the mechanism for this is from the increased voltage of the C-arm to compensate for the dense contrast in comparison with the surrounding tissue. Data on the use of ureteroscopic guided PCNL puncture has been presented with relatively low STs and radiation exposure—4.2 minutes and 2.8 mSv, respectively. 17
This study represents the largest series to date on radiation exposure during PCNL and has demonstrated a substantial reduction in exposure compared with other published series, including those describing novel techniques (Table 3). Subtle changes in surgical technique and experience over time (Fig. 4), can lead to a reduction in STs and can be potentially achieved by all operators performing PCNL within a high throughput center. The authors advocate preaccess marking of the stone position, caliceal tip, and “line-of-attack.” This means that the only variable angle at puncture is that from the horizontal; fixing the C-arm in full extension over the operative field so the only movement is in and out without loss of position; avoidance of continuous screening; and coning the radiation field. Although time spent positioning an antegrade safety wire in the ureter is commonplace, the authors believe this is not always necessary and can add to both the operative time and radiation dose; a wire placed via the ureteral catheter that is kept within the sterile field will allow through and through access to the kidney if needed.
ED=effective dose.
Conclusions
These results demonstrate a substantial reduction in STs compared with other published data, which is achievable with experience over time. The points of technique to minimize radiation exposure include: 1. Lock the C-arm so the only movement is in and out over the operating field. 2. Mark the stone position and “line-of attack” before puncture. 3. Avoid continuous screening. 4. Avoid protracted manipulation of the guidewire into the ureter.
STs have been suggested as a surrogate for technical expertise, and the ability to perform PCNL with a low radiation dose may be directly attributable to experience gained from a large caseload, further strengthening the argument for the centralization of stone surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.