
Abstract
Purpose:
To report the long-term oncologic outcomes and survival estimates associated with minimally invasive partial nephrectomy (MIPN) and to determine factors associated with those outcomes and survival estimates.
Patients and Methods:
A single-institution, retrospective review was performed on all patients undergoing MIPN for renal-cell carcinoma between 1998 and 2011 with minimum 1-year follow-up. Bivariate and multivariate analyses were performed to assess associations between demographic, perioperative, and tumor factors with recurrence and survival. Survival was estimated using the Kaplan-Meier method.
Results:
Of 417 patients undergoing MIPN, median overall and oncologic follow-up were 3.3 and 2.9 years, respectively. The mean patient age was 63 years (standard deviation [SD]±13.4). The mean tumor size was 2.9 cm (SD±1.48). Only 6.7% of patients had a pathologic stage T2 or greater. There was only one cancer-related death. Estimates for overall survival at 2, 5, and 10 years were 95.6%, 89.1%, and 70.7%, respectively. Estimates for recurrence-free survival (any recurrence) at 2, 5, and 10 years were 98.2%, 93.5%, and 88.3%, respectively. On multivariate analysis, only tumor stage was associated with recurrence, and only patient age and American Society of Anesthesiologists score were associated with overall survival. Technical aspects of the procedure, such as positive margins or use of enucleation, did not influence recurrence or survival.
Conclusions:
Cancer recurrence after MIPN, in a cohort of patients with mostly pT1 tumors, is rare. Recurrence and overall survival are associated with nonmodifiable factors rather than technical ones.
Introduction
F
Consequently, the aim of this study is to identify factors associated with long-term overall and cancer-related survival after MIPN, with the hope of informing preoperative patient selection and intraoperative decision making, and to potentially direct future research on the oncologic efficacy of MIPN.
Patients and Methods
All patients undergoing MIPN (includes standard, hand-assisted, and robotic-assisted laparoscopy) at our institution between November 1998 and September 2011 were included in our Institutional Review Board approved and prospectively maintained database. A total of 480 patients underwent MIPN for pathologically confirmed renal-cell carcinoma; those with benign pathology were excluded from this analysis. Of these patients, a minimum 1-year follow-up was available in 417 patients. Long-term oncologic data were obtained and analyzed retrospectively from medical records, radiographic reports, tumor and death registries, and contact with patients, their families, and referring physicians' offices. In patients with bilateral disease managed with staged procedures (n=3), only the first operation was included. Patients with preexisting metastatic disease were excluded from the study.
Our follow-up surveillance protocol comprised regular history and physical examinations together with laboratory testing, chest radiography, and computed tomography (CT) or magnetic resonance imaging (MRI) of the abdomen, generally following the recommendations of Lam and colleagues. 12 For patients who underwent follow-up at another institution, reports from the referring physician were obtained and entered into our computerized database. All patients were accounted for in calculating overall survival (n=417). In determining oncologic follow-up, chest radiography or cross-sectional imaging was required. Only four patients lacked documentation of the imaging necessary for oncologic follow-up to estimate recurrence-free survival (n=413), which included recurrence locally (anywhere in the ipsilateral kidney), regionally, or systemically. Cause of death was ascertained using a combination of sources: Physician note, hospital records, and the Social Security Death Index.
The surgical approach (i.e., standard laparoscopic partial nephrectomy [SLPN], hand-assisted laparoscopic partial nephrectomy [HALPN] and robot-assisted laparoscopic partial nephrectomy [RALPN] ), use of hilar clamping, and the performance of enucleation vs sharp excision of tumor were determined based un tumor characteristics and surgeon preference.
The dependent variables for statistical analysis were overall survival, cancer-specific survival, and recurrence-free survival. Bivariate assessments were made with the log rank test, using the following independent variables: Patient age, American Society of Anesthesiologists (ASA) score, and preoperative estimated glomerular filtration rate (eGFR), (calculated using the Modification of Diet in Renal Disease equation 13 ); tumor stage, grade, and size; surgical approach; enucleation vs sharp excision; ischemia time; and positive margin. We did not assess tumor cell type because of the small number and heterogeneity of nonclear cell types. We then fit Cox proportional hazards models after backward selection for the most parsimonious model to evaluate for association using those independent variables significant on bivariate analysis. Associations are shown as hazard ratios with 95% confidence intervals (CIs). Statistical analyses were performed using SAS 9.2 software (SAS Institute, Cary, NC).
Results
Among the 417 patients, the mean patient age was 63 years (standard deviation [SD]±13.4), 62% were ASA 1 or 2, and the mean pre-operative eGFR was 79 (SD±22.4). Among the MIPN, there were 212 SLPN, 91 HALPN, and 114 RALPN. The mean tumor size was 2.9 cm (SD±1.48). Cell-types included clear-cell in 284 (68%), papillary type 1 in 83 (20%), chromophobe in 28 (6.7%), papillary type 2 in 4 (1.0%), and other or mixed in 18 (4.3%). The tumor grade was 1 or 2 in 271 (65%) patients, and 3 or 4 in the remainder. Most tumors were stage pT1a (329, 79%) or pT1b (59, 14%), with only 28 (6.7%) being tumor stage pT2 or greater (data missing in one patient). Of the procedures, 15% involved tumor enucleation and 85% were performed with sharp excision. The mean ischemia time was 21 minutes (SD±14.2). The final surgical margin was positive for tumor in 23 (5.5%) patients.
The median overall follow-up was 3.3 years (interquartile range [IQR] 2.0–6.0 years), including 120, 70, and 15 patients with follow-up more than 5, 7, and 10 years, respectively. There were 44 deaths overall. Only one patient died of renal cancer. Median oncologic follow-up was 2.9 years (IQR 1.5–4.8 years). There were 17 recurrences (4.1%), including 7 (1.7%) in the ipsilateral kidney, 2 in the contralateral kidney, 3 in the lung, and 5 at other sites. Estimates for overall survival at 2, 5, and 10 years (95% CI) were 95.6% (93.0, 97.2), 89.1% (84.5, 92.4), and 70.7% (56.7, 80.9), respectively. Because there was only one death from renal cancer, we did not calculate cancer-specific survival. Estimates for recurrence-free survival (any recurrence) at 2, 5, and 10 years (95% CI) were 98.2% (96.1, 99.2), 93.5% (88.8, 96.3), and 88.3% (79.6, 93.5), respectively.
Bivariate analyses are summarized in Tables 1A and 1B. Older patient age was associated with tumor recurrence, as were greater tumor stage, grade, and size, as well as the occurrence of a positive surgical margin. Notably, of the 23 patients with positive margin of resection, only 3 had any form of recurrence with 2 recurrences (8.7%) specifically located in the ipsilateral kidney. From a different perspective, of the seven patients with recurrence in the ipsilateral kidney, two (29%) were associated with positive margins. In the three patients with positive surgical margins and recurrence, the median time to presentation of recurrence was 30 months. In the 20 patients with positive surgical margins but no recurrence, the median oncologic follow-up was 31 months. Overall survival was reduced in older patients and those with greater ASA score and lower preoperative eGFR. We also tested the association of tumor recurrence with overall survival, and there was none (P=0.92, data not shown).
Missing 1 patient.
ASA=American Society of Anesthesiologists; RALPN=robot-assisted laparoscopic partial nephrectomy; HALPN=hand-assisted laparoscopic partial nephrectomy; SLPN=standard laparoscopic partial nephrectomy.
SD=standard deviation; eGFR=estimated glomerular filtration rate.
Figure 1 depicts the Kaplan-Meier survival curves for recurrence-free survival, stratified by tumor stage. Figure 2 depicts the Kaplan-Meier survival curves for overall survival, with Figure 2A stratified by age and Figure 2B stratified by ASA score. Of note, the survival estimate for overall survival reached 0% in the subcohort with ASA score 3 or 4 just beyond 12 years.
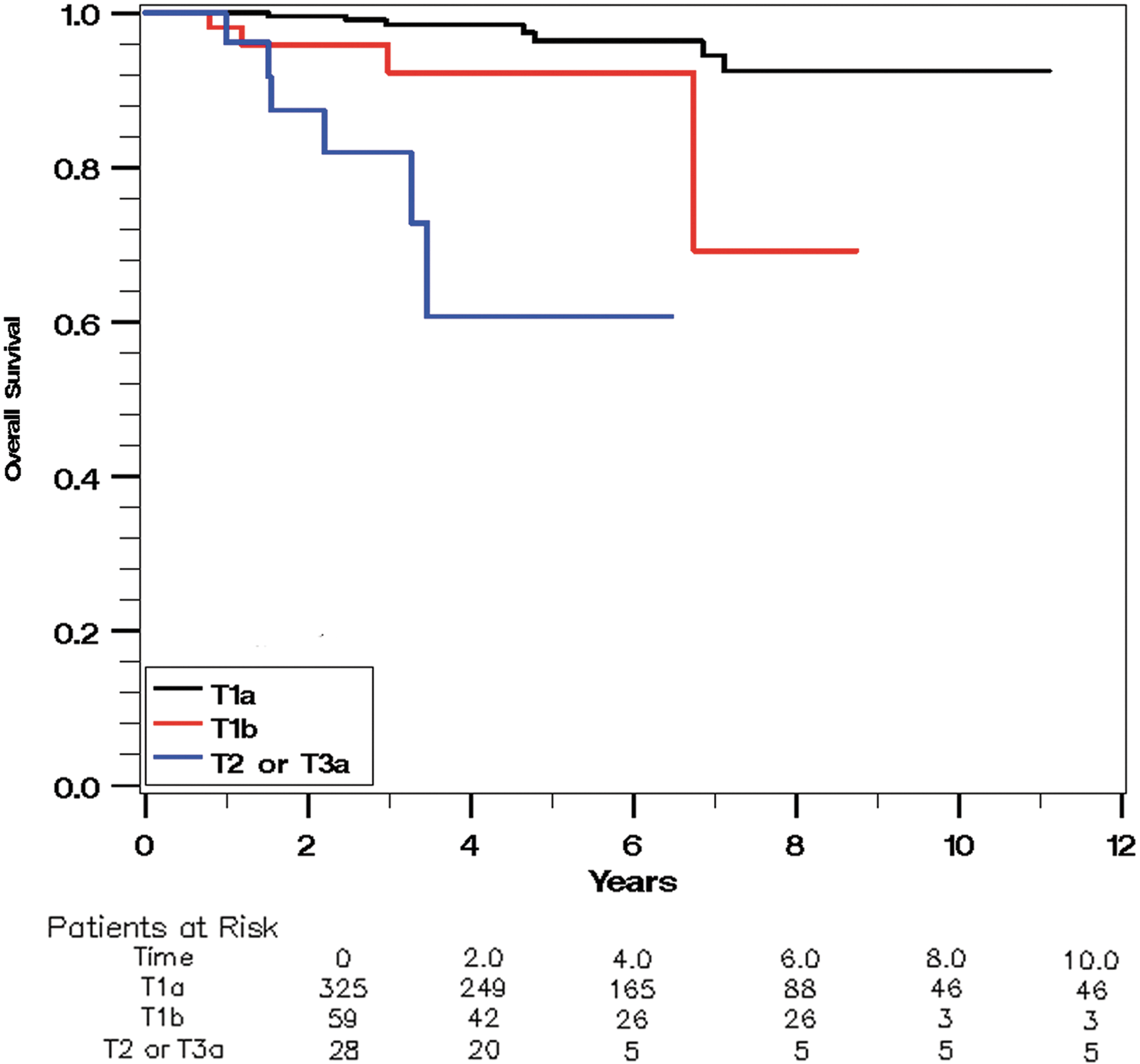
Kaplan-Meier survival curve for recurrence-free survival, stratified by tumor stage.
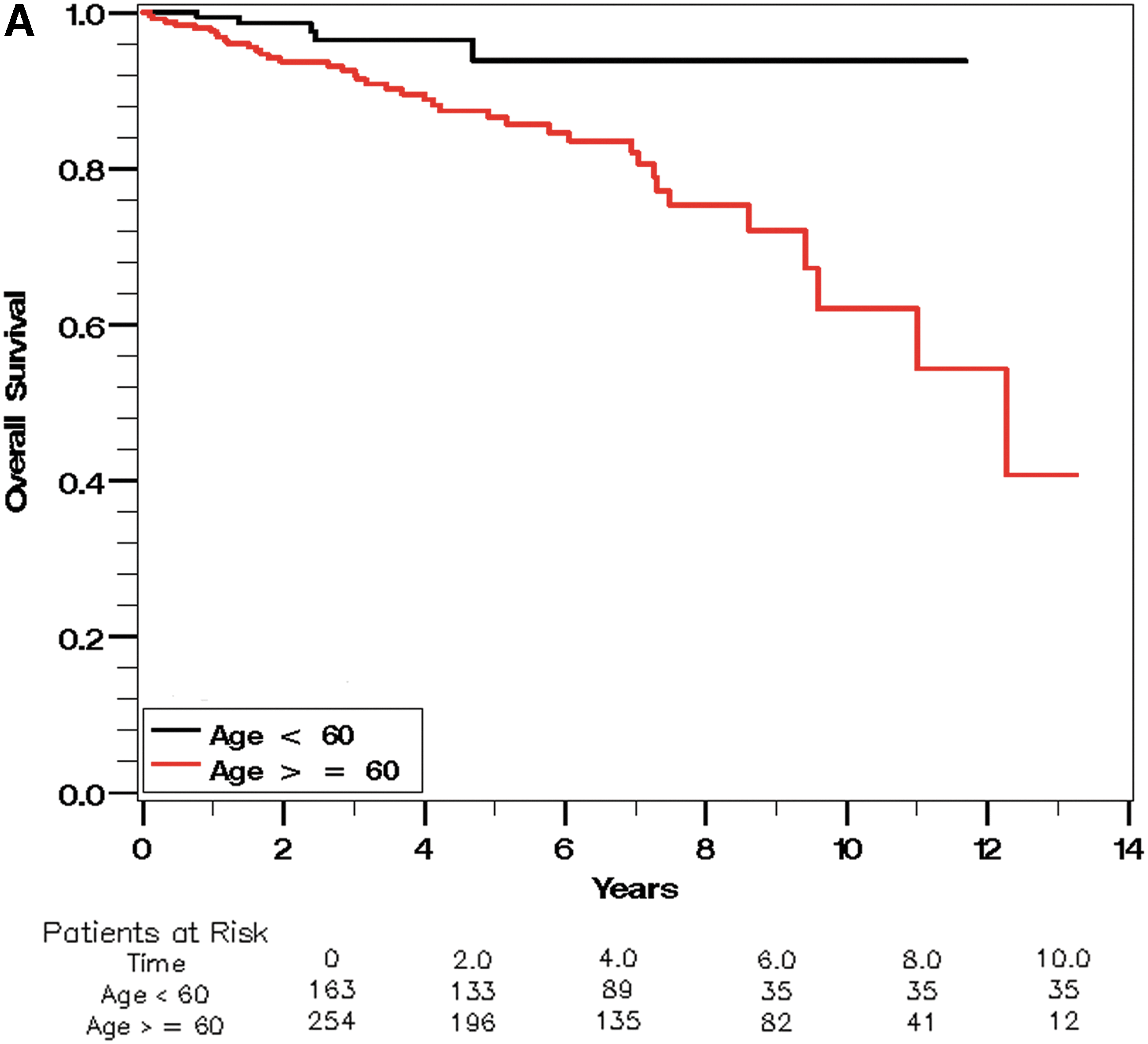
Kaplan-Meier survival curve for overall survival, stratified by age.

Kaplan-Meier survival curve for overall survival, stratified by American Society of Anesthesiologists score.
Results from the multivariate analyses are presented in Table 2. For recurrence, only tumor stage remained associated (P<0.0001). The hazard ratios (relative to stage pT1a) were 4.81 (95% CI, 1.37–16.97) for stage pT1b and 19.46 (95% CI, 5.87–64.59) for stage pT2 or greater. Of the three factors associated with overall survival on bivariate analysis (patient age, ASA score, and preoperative eGFR), the last factor lost significance on multivariate analysis. The hazard ratio for age (P<0.0002) was 1.05 (95% CI, 1.02–1.08), with each additional year being associated with a 5% increase in the hazard of death. ASA score 3 or 4 (P<0.0002) was associated with a hazard ratio of 3.53 (95% CI, 1.81–6.85), relative to ASA score 1 or 2.
Reference group.
CI=confidence interval; ASA=American Society of Anesthesiologists.
Discussion
The management of small renal masses has evolved over the last decade from open surgical PN designed for maximum cancer control to include MIPN focused on the combined goals of oncologic efficacy, reduction of the duration and intensity of convalescence, and preservation of renal function. 14 A number of groups have reported their perioperative and short-term experiences with MIPN, suggesting excellent oncologic efficacy, as well as low recurrence rates. 15,16 Longer follow-up, however, is needed to confirm the oncologic efficacy of MIPN.
Some series that report oncologic follow-up in excess of 3 years are limited by the size of their cohorts. 17,18 Lane and associates 11 recently reported a series that included 45 patients with more than 10 years follow-up after MIPN; overall survival was 78% at 10 years, and metastasis-free survival was 97%. Using both laparoscopic and open surgical cohorts, these authors identified several independent predictors of overall survival and recurrence in the long term: Older age, larger tumor size, absolute indication, and Charlson comorbidity index. Because ASA score and Charlson comorbidity index appear to predict mortality equally well, 19,20 these findings are similar to ours with regard to overall survival. With regard to tumor recurrence, Lane and associates 11 found that surgery type was not associated with oncologic outcome, again similar to our finding that no technical aspects influenced recurrence-free survival.
Finally, our finding on multivariate analysis that positive surgical margins were not associated with tumor recurrence is consistent with a growing body of evidence. 21 –23 There are several possible explanations for the observation that positive surgical margins on pathologic examination of the resected tumor do not result in recurrence in many cases, including: Intraoperative fulguration of the tumor bed, ischemic damage to residual tumor from hemostatic sutures, retraction of normal parenchyma away from the tumor during tissue processing, and/or the appearance of a positive margin when the resection was adjacent to the tumor's pseudocapsule and in fact there is no tumor left in the patient. Alternatively, it may be that the duration needed for positive margins to produce a clinically noticeable tumor has not yet been achieved in most series.
In our cohort, characterized by relatively young and healthy patients with good renal function and small, low-risk tumors, the risks of recurrence and death were low, with estimated 88.3% recurrence-free survival and 70.7% overall survival at 10 years. There was only one cancer-related death. Of the 17 patients with recurrence, only 4 (3 with pulmonary metastases and 1 with abdominal lymph node metastases) had recurrence beyond the ipsilateral or contralateral kidney, adrenal gland, or a resectable solitary metastasis. As such, oncologic risk factors impacted only recurrence, and not survival. The excellent oncologic outcomes in our cohort do suggest great efficacy of MIPN, but they also suggest the possibility that at least some of these small renal cancers are being overtreated. In particular, competing causes of mortality are especially important, as illustrated by the finding of no survival beyond 12 years in patients with ASA score 3 or 4. We, like many other groups, are increasingly using active surveillance in patients with small renal masses and high competing risks of mortality. 24 The excellent results of MIPN provide the context in which we should assess active surveillance strategies going forward.
The present study has several limitations including the selection bias for patients with unilateral, low-volume disease, the changes in surgery and practice patterns over the last decade, the varied learning curves of the different surgeons, errors in retrospective data extraction, and variability of patient follow-up. Despite these limitations, we think that this evaluation of the long-term outcomes of a large cohort of MIPN patients is crucial to better understanding this procedure.
Conclusion
To our knowledge, this is the first study in the literature to examine long-term (≥3 years) oncologic outcomes after three different types of MIPN in a large population with each patient having at least 1 year of follow-up. Our data confirm that MIPN, in a cohort of mostly pT1 tumors, is associated with infrequent tumor recurrence even on long-term follow-up. Only tumor stage influences recurrence; the technical aspects of MIPN such as the surgical approach (SLPN, HALPN, or RALPN) or the method of resecting the tumor (enucleation or sharp excision) were not associated with recurrence. With limited impact of these small renal cancers on mortality, the clinician's operative decisions should be guided by the understanding that recurrence-free survival is influenced by tumor stage and that overall survival is influenced by patients' age and medical condition.
Footnotes
Disclosure Statement
Dr. Wolf is American Urological Association Chair, Practice Guidelines Committee, and an editorial consultant for Urology Times. For the remaining authors, no competing financial interests exist.