
Abstract
Background and Purpose:
Laparoendoscopic single-site surgery (LESS) is a surgical option for a number of urologic operations, although it does carry technical limitations. One of the major obstacles in performing LESS is accomplishing optimal retraction of adjacent organs. The aim of this study was to investigate the feasibility of a novel self-retaining intracorporeal retractor device, the Internal Organ Retractor (IOR), and to describe our experience using this device in LESS.
Patients and Methods:
A total of 23 patients who underwent LESS using IOR between December 2012 and July 2013 were identified. Among these patients, 11 nephrectomies, 9 adrenalectomies, 1 pyeloplasty, and 2 nephroureterectomies were performed. Perioperative outcomes including operative time, complications related to use of the IOR, and amount of time needed for the application and removal of the IOR were measured during each operation.
Results:
Adequate retraction was accomplished in all surgical cases. The IOR helped to maintain a consistent operative field throughout the surgery. A median application time of a single IOR was 85.0 (range 44.5–187.5) seconds and removal time was 50.0 (20–400) seconds. The median number of IOR sets used was 2.0 (range 1–4), and the median total application and removal time in a single operation were 170.0 (45–750) seconds and 95.0 (20–400) seconds, respectively. There were no perioperative complications associated with use of the IOR.
Conclusions:
The IOR provided satisfactory retraction during LESS, and its application/removal was uncomplicated and needed a minimal amount of time. The IOR reduced the need for additional laparoscopic ports for retraction. We believe that the IOR is a useful retraction tool for LESS and possibly multiport laparoscopic surgeries.
Introduction
L
Another major obstacle is accomplishing optimal retraction of adjacent organs. Because the number of working instruments is limited and there is a small amount of space between these instruments, establishing an optimal operative field is challenging. In many cases, additional ports or needlescopic instruments are needed, and various intracorporeal devices such as a transabdominal stay suture, an endoloop, 2 or an Endograb™, are used.
Although many retraction methods have been described, 2 –5 an ideal technique has not yet been established. The Aesculap® Internal Organ Retractor (IOR; Aesculap AG, Tuttlingen, Germany) is an internally applied retraction device that does not need additional ports. We propose that use of this tool may help to expand the application of LESS, making it more accessible to surgeons with all levels of experience. In this study, we investigated the feasibility of using the IOR in 23 patients who underwent various urologic operations.
Patients and Methods
This study was approved by the Institutional Review Board at Samsung Medical Center (IRB No. SMC 2013-09-064).
Patients
We reviewed medical records of 23 consecutive patients who underwent LESS using the IOR between December 2012 and July 2013. Eleven patients underwent nephrectomies (8 simple and 3 radical nephrectomies), 9 had adrenalectomies, 2 had nephroureterectomies, and 1 had a pyeloplasty. During renal and adrenal surgeries, the IOR was used to retract the liver in the right side and the spleen and pancreas in the left side. The IOR was also used for retraction of the descending and sigmoid colon during nephroureterectomies.
The amount of time for application and removal of the IOR during the operation was measured prospectively. The application time was defined as the elapsed time from entrance of the IOR using the clip applier through the laparoscopic port to the completion of anchoring on the abdominal wall. The removal time was defined as the elapsed time from introduction of the needle holder through the laparoscopic port to expulsion of IOR through the laparoscopic port.
Perioperative outcomes including operative time, estimated blood loss, overall complications, and complications related to IOR use were evaluated.
Port placement for LESS
Surgical procedures and port placement for LESS were performed according to previously described methods with some modifications. 6 –8 Briefly, patients were positioned in a nearly 90-degree flank position, which helps to make the colon pulled down by gravity. Through a 2 to 3 cm umbilical incision, an Alexis® wound retractor (Applied Medical, Rancho Santa Margarita, CA) was inserted. A handmade single port, 6,9 which was composed of a surgical glove and three laparoscopic trocars, was fixed to the outer ring of the wound retractor. After insufflation with CO2 gas, a 10-mm Endocameleon® scope (Karl Storz, Tuttlingen, Germany) was introduced. Articulating laparoscopic instruments (Autonomy Laparo-angle™, Cambridge Endo, Framingham, MA) were used to achieve the required angles, and other conventional laparoscopic devices were used.
Composition and application of the IOR
The IOR is an internally anchored retracting device. It is composed of a reusable atraumatic clip and a disposable silicone ring with an anchoring needle (Fig. 1). Before application, a silicon ring was combined with an atraumatic clip. We used the triangular jaw designed atraumatic clip that provides 5.0 N of grasping force. The IOR was set on the clip applier, which was identical to a bulldog clip applier (Aesculap AG, Tuttlingen, Germany). After adequate dissection of the operative field, the IOR was introduced through a 12-mm port. The anchoring needle was fixed using the jaws of the clip during insertion via trocar to avoid unintended hooking on the multiport trocar or internal organs (Fig. 1d).

Composition of the Internal Organ Retractor. The Internal Organ Retractor is composed of an atraumatic clip
The atraumatic clip was applied to tissues around the organ that was to be retracted. The clip was not attached to the organ directly to avoid trauma. The anchoring needle was then affixed to the abdominal wall using the needle holder. At the conclusion of the operation, the IOR was removed in the reverse order. While removing the IOR through the multichannel port, the needle was grasped using the needle holder to avoid unintended hooking.
Operative techniques
All surgical procedures were performed in the same manner as that of conventional laparoscopic surgeries.
During nephrectomy, adrenalectomy, and pyeloplasty, the abdominal cavity was adequately visualized after the formation of the pneumoperitoneum. The white line of Toldt was incised, and the colon was shifted medially to allow access to the retroperitoneal space. For the right side, the peritoneum near the liver was incised and dissected away from the upper portion of the Gerota fascia. One or two IORs were applied to retract the liver (Fig. 2a). For the left side, the spleen, pancreas, and descending colon were dissected medially as a whole. One or two IORs were then applied to retract these organs (Fig. 2b). If optimal retraction was not achieved during the operation, readjustment of the IOR was achieved by simply moving the anchoring needles.
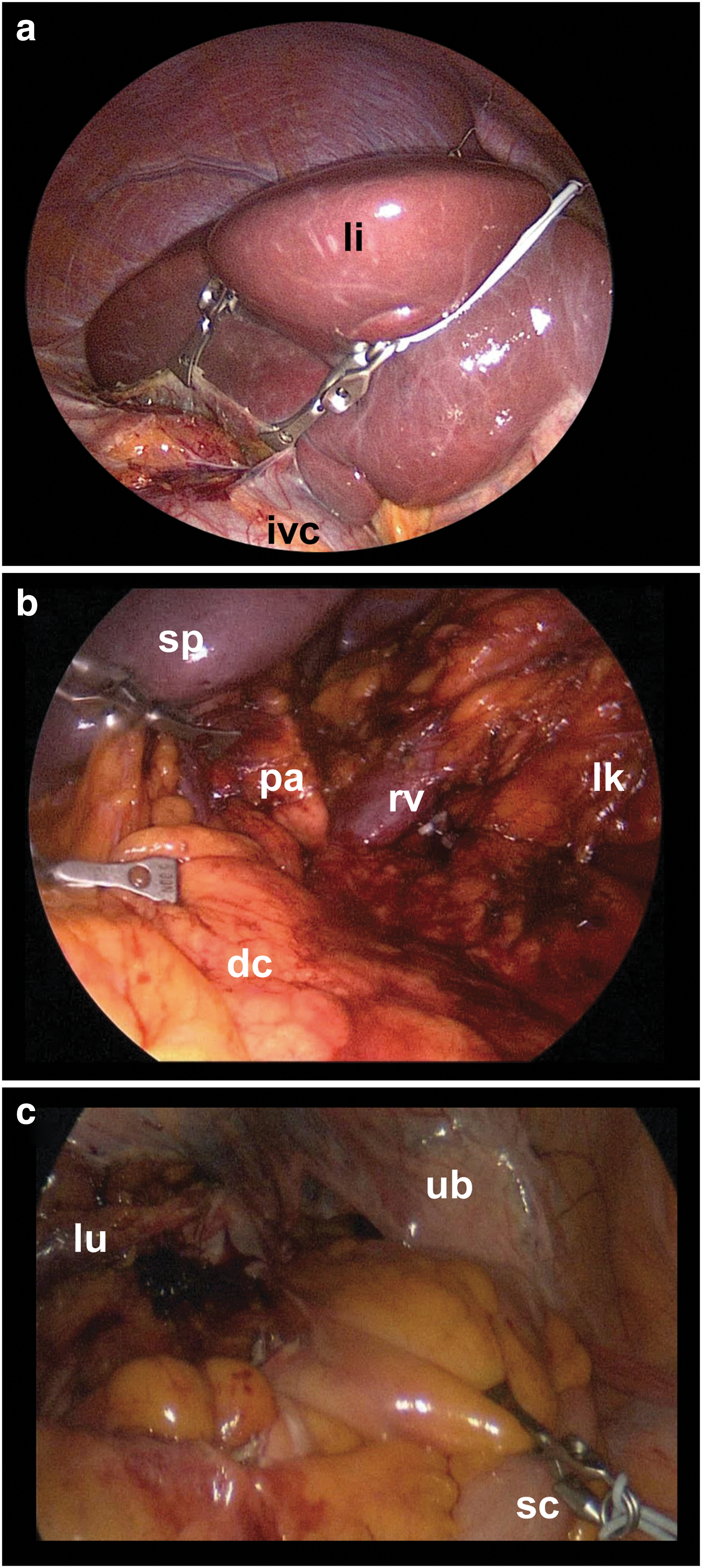
Application of the Internal Organ Retractor. Internal Organ Retractors were applied during various urologic laparoendoscopic single-site surgeries:
For the nephroureterectomy, nephrectomy was performed as described above. For dissection of the ureter, the IOR was applied to retract the sigmoid colon and the rectum medially. The sigmoid mesocolon was grasped with an atraumatic clip to avoid bowel injury, and the needle was anchored to the contralateral abdominal wall (Fig. 2c).
Results
Among the 23 surgeries that used LESS, 14 cases were right-sided and 9 cases were left-sided. The median age was 42.0 (range 19–71) years, and the median body mass index was 25.0 (19.1–28.1). Baseline characteristics of the patients are summarized in Table 1. Adequate retraction was achieved in all cases. The IOR maintained a consistent operative field, and the need for readjustment was rare. Only one simple nephrectomy was converted to hand-assisted laparoscopic surgery because of severe adhesions and renal vein injury. There were no complications associated with IOR placement or removal. There were 4 intraoperative complications that were not associated with the IOR. Two of these were minor renal vein injuries that were repaired using primary suture, and the other two were minor serosal injuries of the colon that were repaired with sutures without additional port placement.
BMI=body mass index; ASA=American Society of Anesthesiologists.
The median number of IORs applied during a single surgery was 2.0 (1–4). The median total elapsed time for application of the IOR was 170.0 (45.0–750.0) seconds and for removal of the IOR was 95.0 (20.0–400.0) seconds. When using a single IOR, it took 85.0 (44.5–187.5) seconds for application and 50.0 (20.0–400.0) seconds for removal (Table 2).
IOR=Internal Organ Retractor; EBL=estimated blood loss.
In one case, the silicone ring was ruptured during removal because it was grasped directly with the needle holder. Fortunately, the needle was anchored to the abdominal wall, and no injury was sustained.
Discussion
LESS is an evolving laparoscopic surgical method. The feasibility of LESS has been demonstrated for almost all urologic surgeries 10 as a result of the development of various articulating instruments and flexible or adjustable optics. 11 Nevertheless, LESS continues to have challenging technical aspects that prohibit widespread use of the procedure. In LESS, only a single incision is made, and all instruments are introduced in a single direction. This typically limits the number of simultaneously working instruments to two.
We positioned patients in the full flank position to use gravity to retract the intraperitoneal organs in their respective dependent directions. While the colon is easily retracted using this method, however, it is commonly insufficient or impossible for retraction of solid organs such as the liver, spleen, or pancreas. Achieving adequate retraction is the major technical challenge that often necessitates placement of additional ports. Thus, conversion to multiport laparoscopic surgery or hand-assisted laparoscopic surgery is common for the beginners in LESS and is not rare even for experts.
In LESS, needlescopic instruments are good alternatives to additional laparoscopic ports because it virtually does not make additional scar. 12 Notably, however, the grasping and traction power of needlescopic instruments is sometimes not sufficient, and holding the instruments during the operation necessitates additional effort.
Other retraction methods or devices have been developed and used for LESS or other laparoscopic surgeries. Transabdominal stay suture is a commonly used method. 3 The sutures are introduced through the skin to the target tissue and are then pulled outside of the body. In this way, traction can be manipulated extracorporeally with negligible damage to the skin. This technique has limited capability for retraction, however. To avoid a potential pneumothorax, the suture should be applied inferior to the rib cage, which may result in suboptimal retraction of solid organs that are located in the upper abdomen, such as liver and spleen. Intracorporeal handling of large needles is also cumbersome and increases the risk of internal organ injury. In addition, readjustment of the stay suture is also limited during surgery.
Alternatively, Uras and Boler 2 reported an endoloop retraction technique for LESS cholecystectomy. They demonstrated that this method is both easy to perform and a good substitute for traction sutures without the risk of bile spillage. It also necessitates penetration of the abdominal wall, which limits the direction of retraction because of potential injury within the thoracic cavity. This technique cannot be universally applied, because the endoloop needs to be fastened to protruding organs such as the gallbladder or appendix.
Recently, the use of intracorporeal retraction devices that can be applied internally without any damage to the skin has been reported. 4 The Endograb™ (Virtual ports, Misgav, Israel) is a fully insertable and self-contained intracorporeal retracting device similar to the IOR. It is composed of two atraumatic grasping jaws and a wire connecting them. Schlager and associates 4 reported the safety and effectiveness of this device for use in LESS cholecystectomy. This method created no additional skin wounds and could be applied superiorly without injury to the thoracic cavity. It can be introduced through 5-mm port and is repeatedly adjustable throughout the operation. A possible drawback of this device, however, is a limited flexibility of the connecting wire. The operative field in urologic surgeries is mainly located in the retroperitoneal space. For adequate visualization of the field, the intraperitoneal organs (such as the colon, liver, spleen, and pancreas) should be fully retracted to the contralateral side. As a result, the limited flexibility of the Endograb™ could hinder this.
Another attractive method for overcoming the technical drawbacks of LESS is magnetic use of an anchoring and guidance system (MAGS), which was developed by Caddedu and Scott in 2001. MAGS consists of internal neodymium-iron-boron magnetic platforms and external anchors that stabilize and manipulate the internal platforms. 5,13 It is introduced through a single port and is manipulated by an external anchor. Conceptually, MAGS is an ideal instrument for LESS. Aside from the high cost and a steep learning curve, however, an exponential decrease in magnetic strength as a function of distance is a significant drawback of MAGS. This technique is still under development and has only been used in animal models and human cadavers. 14 –16 MAGS may be a promising tool for minimally invasive surgeries in the future, however, and clinical application is anticipated.
Colon and colleagues 17 reported a very similar device to the IOR. It consists of a laparoscopic bulldog clamp fitted with a small metal hook. It was successfully used in a case of LESS cholecystectomy. The main structure is quite different from the IOR, however. The clip consists of a full metallic body and the length is nearly fixed because of its low elasticity. So the application seems to be more limited than the IOR because the distance between target organ and the optimal point of the abdominal wall to be anchored is variable depending on situations.
The IOR is a reasonable alternative to additional port placement for retraction and could be applied in almost all laparoscopic surgeries. The cost of the IOR is also reasonable because the clip and applier is reusable and the disposable silicon ring is supplied with low cost (about $65 in Korea). This method does not result in skin wounds and provides enough traction power that allows maintaining a stable retraction during the entire procedure. The application of one or two IORs could result in optimal retraction of the liver without placement of additional ports. The flexibility and elasticity of the silicone ring allows enough length to fix the anchoring needle to the opposite side of the abdominal wall, which make it useful in various situations.
Furthermore, the application time for a single IOR was approximately 2 minutes, and the removal time was approximately 1 minute. Manipulation of the IOR was intuitive; an atraumatic clip provided a secure grasp of the tissue, and the elasticity and conformability of the silicone ring provided stability and safety during retraction. Unintended contact with or stretching of the retracted organs was rarely harmful, and readjustment was rarely necessary because of the flexibility of the silicone ring. When necessary, repositioning of the IOR was easily performed by moving the anchoring needle to again achieve adequate retraction.
While IOR is not essential for LESS, the retraction provided by use of the IOR and the maintenance of a consistent operative field enables the use of both hands for fine dissection. Furthermore, we expect that the IOR could reduce complication rates of LESS. For surgeons who are not familiar with LESS, IOR may be helpful. It can also be applied to conventional laparoscopic surgeries or robotic surgeries to reduce the number of ports needed for retractions especially in right-sided adrenal or renal surgeries in which adequate retraction of the liver is essential.
Use of the IOR system has some limitations. During application or removal, the anchoring needle could damage adjacent organs or could become stuck in the port. In addition, while the durability of the silicone ring is excellent and it can endure substantial retractions during surgery, grabbing the ring directly with the needle holder could damage the silicone by crushing, which may lead to rupture. It is therefore important to hold only the anchoring needle during removal (Fig. 3). We experienced one case of silicone ring rupture, although fortunately, the needle remained anchored to the abdominal wall and was safely removed. Finally, the IOR is relatively large and needs a 12-mm port. This is not an issue in LESS, however, which can easily use larger ports without lengthening the incision.

Removal of the Internal Organ Retractor. During the removal of the Internal Organ Retractor, operators should pay close attention to securely grasp the anchoring needle to avoid unintended damage.
There are several limitations of our study including the retrospective study design and the small number of patients. The absence of a comparative group that did not use the IOR is also an important drawback. Nevertheless, we consider this study to be valuable because it is the first report of the intracorporeal retraction device in urologic surgery. The IOR is a novel self-retaining intracorporeal retractor device, and it could be applied in many various LESS and laparoscopic surgeries. The role of the IOR needs to be further confirmed by prospective comparative studies with a large number of cases.
Conclusions
We have demonstrated that use of the IOR could provide satisfactory retraction during LESS. Its application and removal was simply and rapidly performed. We propose that the IOR could reduce the need for additional ports for retraction in LESS. We believe that IOR is an attractive retraction method during LESS and possibly even in multiport laparoscopic or robotic surgeries.
Footnotes
Disclosure Statement
No competing financial interests exist.