
Abstract
Background and Purpose:
Tubeless percutaneous nephrolithotoomy (PCNL), although an accepted technique by now, continues to suffer from two major limitations: The need for postoperative cystoscopy for ureteral stent removal and inability to perform a “second-look” procedure for any residual fragments. We share our experience with a modification of the standard tubeless PCNL technique that allows us to overcome these shortcomings.
Patients and Methods:
A total of 166 patients selected to have PCNL were randomized into two groups of 83 each. In group A (control group), the patients underwent standard PCNL with the insertion of a nephrostomy tube at completion; in group B (intervention group), modified tubeless PCNL was performed with a Double-J (DJ) stent inserted with a tether attached to its proximal end, taken out through the percutaneous tract. The nephrostomy tube in group A was removed postoperatively on the second or third day, whereas those in group B had the stent removed directly by pulling the attached tether within the office setting 10 to 14 days postoperatively.
Results:
The need for postoperative analgesia was significantly higher in group A compared with group B (mean dose of tramadol needed, 128 mg vs 81.3 mg) (P<0.001). Four patients in group A had postoperative urinary leakage from the nephrostomy site, whereas there were no leaks in patients in group B. Group B patients spent significantly shorter average time in hospital (21.6 hours) compared with group A (54 hours) (P<0.001). Two of the patients in group B needed a second-look procedure, performed by the insertion of a guidewire down the stent, which was pulled out partially by its tether. Presence of the tether in the flank or the process of subsequent removal did not cause any discomfort to any patient.
Conclusion:
The present study demonstrates that tubeless PCNL with a tethered DJ stent overcomes its main drawback, namely, the need for cystoscopy for stent removal, and also allows access to the pelvicaliceal system for second-look nephroscopy.
Introduction
A
Working on the principle that the nephrostomy tube primarily serves the purpose of providing good kidney drainage, the “tubeless” approach was developed using internal drainage to provide the same benefits as an external tube. This approach involves inserting a ureteral Double-J (DJ) stent or a simple ureteral catheter instead of the usual nephrostomy tube after PCNL. 4 There is sufficient evidence from many subsequent studies to show this tubeless approach to be a safe as well as cost-effective procedure, having the benefits of reduced postoperative pain and morbidity, and shorter duration of hospital stay. 5,6 A study conducted by Desai and associates 7 illustrated the advantages of the tubeless approach in a comparison of tubeless, large bore, and small bore nephrostomy drainage in PCNL. Another randomized controlled trial undertaken at our center, which was prospective in nature and to date has the largest sample size of 202 patients, confirmed the same results and demonstrated the tubeless approach to be superior in all parameters—postoperative pain and analgesia requirement, perioperative morbidity, duration of stay in hospital, and recovery time. 8
Tubeless PCNL with placement of a DJ stent has one major limitation—the necessity of cystoscopy postoperatively for stent removal. This is typically performed as an outpatient procedure under a local anesthetic; however, some patients need general anesthesia and short-term hospitalization, adding to the overall cost and morbidity. In addition, whereas a nephrostomy tube helps to re-access the percutaneous tract for second-look nephroscopy for any residual stones discovered on postoperative imaging in standard PCNL, no such facility is available in tubeless PCNL. This also precludes the use of tubeless PCNL when second-look is anticipated, as in kidneys with large and multiple calculi.
In this study, we use a modified technique of tubeless PCNL, in which at completion of the stone removal, a DJ stent is inserted in the ureter with the addition of a tether attached to its proximal end. The tether is brought out through the nephrostomy tract, which enables removal of the stent postoperatively simply by pulling at the tether in the office setting. This simple modification of the standard tubeless technique by adding a tether helps to overcome both the above-mentioned disadvantages of tubeless PCNL—obviating the requirement for a second procedure, cystoscopy, to remove the stent, and more importantly, keeping the percutaneous nephrostomy tract available for second-look nephroscopy.
Patients and Methods
A prospective randomized controlled study at our center within the period from September 2006 to August 2012 was undertaken after acquiring Institutional Review Board approval. During this period, a total of 1043 patients underwent PCNL at our center, of which 166 patients met the inclusion criteria for this clinical trial. They were randomized into two equal groups of 83 each. Allocation and randomization of patient groups was performed in the operating theater after the stone removal by systematic sampling method, and the methodology was in accordance with the Consolidated Standards of Reporting Trials (CONSORT) statement.
The patients in group A (n=83) acted as controls and had a nephrostomy tube (size 12F) inserted at completion of the PCNL, while group B patients (n=83) received a DJ stent with a 3/0 nylon tether attached to its proximal end that was left protruding through the nephrostomy tract. The stent was inserted in antegrade fashion at completion of the PCNL. The inclusion criteria consisted of the following variables: Normal renal function tests, single tract procedure, American Society of Anesthesiologists (ASA) score 1 or 2, lack of any intraoperative complication, the absence of any congenital abnormalities, complete clearance of stone, and minimal blood loss at completion. All caliceal, pelvic, and upper ureteral stones irrespective of stone characteristics such as type, dimensions, and quantity were included as long as the above criteria were met. Any urinary infection detected preoperatively by urine culture was managed appropriately by antibiotics. It was also ensured that no patients had any stents indwelling before surgery. Factors not taken into consideration for patient inclusion were hydronephrosis and puncture site being either supracostal or infracostal.
Perioperative antibiotic prophylaxis was administered in all patients, using a third-generation cephalosporin intravenously for three doses. Procedures were performed routinely under spinal or epidural anesthesia. All of the surgeries were performed by a single surgeon with long-standing experience of endourologic surgery. Retrograde ureteral catheterization was performed first, after which the PCNL was performed with the patient in the prone position. Ultrasonography and biplanar C-arm fluoroscopy were used in combination in accomplishing the percutaneous puncture. The tract was dilated using serial fascial dilators (Cook Urological) with the guidance of fluoroscopy. The stones were removed using a 20.8F nephroscope (Wolf), through a 24F Amplatz sheath (Cook Urological). Ultrasonic and pneumatic lithotripsy (Swiss lithoclast, EMS) were used to fragment stones larger than 8 mm. After stone removal, group A patients had a 12F nephrostomy tube inserted, whereas group B patients had a DJ stent (5F/26 cm) introduced in an antegrade fashion, with a tether (3-0 size nylon string, as provided by the manufacturers) attached to its cephalic end. The tether was brought out to the skin via the nephrostomy tract, and a single nylon suture was used primarily to close the incision site (Fig. 1).
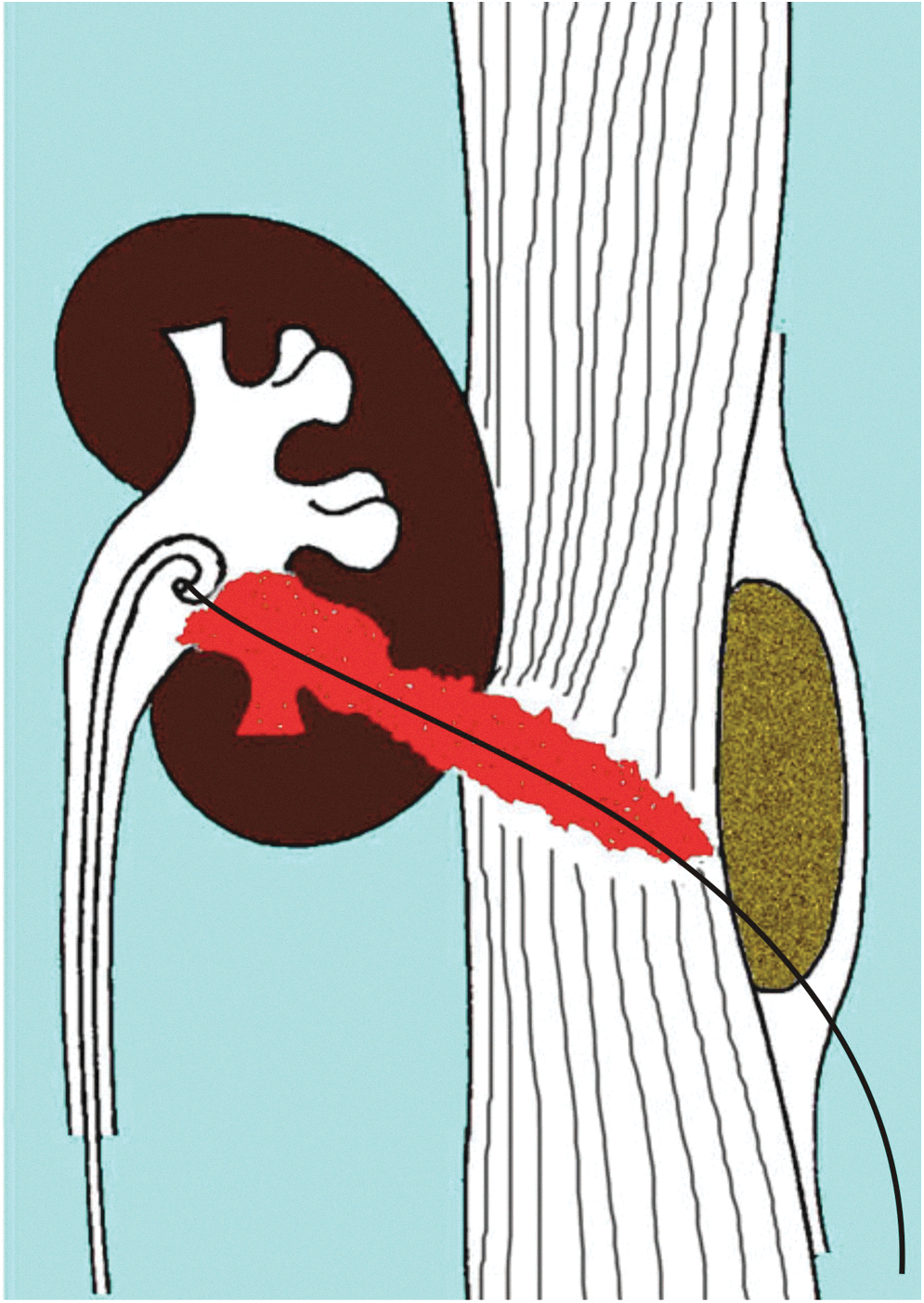
Illustration of the antegrade tether exiting via the nephrostomy tract.
Analgesia used for the first 24 hours postoperatively was tramadol 50 mg administered intramuscularly pro re nata. The pain score was judged within this 24-hour period using a linear 100-mm visual analogue scale (VAS: 0=no pain, 100=maximum intolerable pain). 9 After 24 hours, analgesics were given orally, including anti-inflammatory drugs. No pain and clear urine permitted patients to be discharged from the hospital.
Plain radiography of the abdomen and ultrasonographic examination was performed in all cases on the first or second postoperative day before discharge from the hospital. After 2 or 3 days postoperatively, the nephrostomy tubes were removed in all group A patients after confirmation of complete clearance. In group B, the DJ stent was removed 10 to 14 days after surgery as an office procedure by simply pulling on the tether.
For any residual stone detected on postoperative imaging, second-look nephroscopy was performed—in group A by passing a guidewire through the nephrostomy tube to re-access the tract, and in group B, by pulling out the stent partially with the help of the tether up to skin level, and then passing a guidewire down the stent.
All patients underwent plain radiography and noncontrast CT (NCCT) 1 month after the operation for confirmation of complete stone clearance. Three-month follow-up was performed for all patients. The variables taken into account for evaluation included postoperative pain, the need for and dose of analgesia, postoperative urine leakage, loss of blood, incidence of infection, duration in hospital, stone clearance, and recovery time.
All statistical analyses were completed using Z test, which calculated the proportions and means. A 5% error margin was considered as acceptable. SPSS statistical software was used for the calculation of all parameters.
Results
Both the groups were analogous in demographics, such as age and sex, as well as metabolically and anatomically. No disparity was obvious in either group with regard to distribution in calices, pelvis, and upper ureter. These data are summarized in Table 1 (demographics and characteristics) and Table 2 (results).
PCNL=percutaneous nephrolithotomy; DJ=Double-J.
VAS=visual analogue scale; Hb=hemoglobin.
The average VAS pain score in the two groups was as follows: Group A, 59.3 mm; group B, 31.8 mm. The average tramadol dose needed for analgesia <24 hours postoperatively was as follows: Group A, 128 mg; group B, 81.3 mg. Both these parameters concerning pain had differences that were statistically significant (P<0.001).
Postoperative urinary leak through the nephrostomy tract after tube removal was found in four patients from group A, whereas no patients in group B had any urinary leak from the site of percutaneous access, either with the stent in vivo or after removal. In the four group A patients who had a leak, this resolved without intervention within 3 to 5 days.
Infection acquired postoperatively was recognized as any one of these signs: Pyrexia >38°C (>100.4°F), leukocytosis>11,000/mm3 or presence of >5 pus cells in urine/high power field. Incidence of infection was four cases in group A, and three cases in group B, which was not statistically significant (P=0.69). These patients were treated by suitable antibiotics after a urine culture and sensitivity test. The average fall in levels of hemoglobin was 0.39 gm% in group A, and 0.35 gm% in group B, not a statistically significant difference (P=0.165). No patient needed a blood transfusion.
The average duration of time spent in hospital as an inpatient postoperatively was 54 hours in group A and 21.6 hours in group B. This difference was found to be statistically significant (P<0.001). Standard PCNL (group A) patients took 9.1±1.5 days for complete recuperation, whereas tubeless PCNL (group B) patients only required 5.7±1.4 days. This difference was found to be statistically significant as well (P<0.001).
Two group A patients and one group B patient were discovered postoperatively to have small residual stones, for which a second-look procedure was performed as described earlier, and this helped in achieving complete stone/fragment clearance in these three patients.
In group B, the incidence of stent-related symptoms (dysuria, flank pain) was 7/83, all mild, which resolved after stent removal. In this group, the tether protruding from the flank did not cause any discomfort or pain to any of the patients. All stents were removed successfully by pulling at the tether without any significant pain, and there was no incidence of tether breakage or any other complication while pulling out the stent; neither did this lead to any cases of bleeding from the percutaneous tract or hematuria.
No significant perinephric fluid collection was noted in any patient postoperatively either at the Ultrasonography examination on postoperative day1/2, or on NCCT at 1 month. All 166 patients were stone free on NCCT at 1 month. There were also no patients who had to be readmitted for causes such as pain, infection, or obstruction, and no long-term sequelae were detected in any patient during follow-up.
Discussion
Goodwin and colleagues 10 originally described using a “nephrostomy tube percutaneously” for draining a hydronephrotic kidney in 1955. Removing a stone via a percutaneous access was not accomplished, however, until 1976 when Fernström and Johansson 11 reported PCNL for the first time. From that time, over the years, the technique to remove renal calculi percutaneously has been proven as safe, effective, and superior over the conventional open technique. 12 –15
Recently, however, the focus has been around improving the current technique of PCNL and helping to make it a procedure that is cost-effective and has a low morbidity associated with it. One such example is questioning the need for a routine nephrostomy tube insertion after PCNL. Bellman and coworkers 4 adopted a “tubeless” approach that dispensed with the usual nephrostomy tube and instead placed a DJ stent in the ureter. The duration in hospital, need for analgesia, time needed to resume usual daily activities, and cost all reduced dramatically with this approach.
“Tubeless PCNL” has gained widespread popularity, and many studies have attested to its safety and efficacy as outlined earlier. 5 –8 Several studies have shown the safety as well as efficacy of tubeless PCNL in various scenarios such as patients with a single kidney, multiple tracts for renal access, punctures made supracostally, altered renal functions, and even in persons undergoing simultaneous bilateral PCNL. 16 –18 There is no doubt, however, that a nephrostomy tube becomes necessary if there is any significant bleeding or injury to the collecting system. Similarly, a nephrostomy tube becomes a necessity if there is fluoroscopic evidence of residual stone burden at completion.
Tubeless PCNL has one major disadvantage, which is that the stent needs to be removed postoperatively by cystoscopy. Several studies have used various modifications in tubeless PCNL to overcome this problem. Mouracade and associates 19 adopted a method of tubeless PCNL that involved postoperative placement of an external ureteral stent. In this study, as well as several subsequent publications, tubeless PCNL with a ureteral catheter was found to be safe and effective with considerable reduction in hospitalization time, postoperative pain, and need for analgesia. 20 –24
A prospective trial was undertaken by Gonen and colleagues, 25 comparing the results of placing an external ureteral catheter with placing a DJ stent in tubeless PCNL. The results of this study showed that externalized ureteral catheterization is equivalent to the DJ stent, although another outcome noted by the authors was that in patients who may still have evidence of residual stone fragments, a DJ stent may be preferable because this aids in spontaneous passage of the fragments. In addition, in our experience, we have been concerned with the need to leave a urethral catheter for the duration of ureteral stent placement in these patients, with the associated discomfort caused by it negating the benefits of avoiding the nephrostomy tube.
A hypothesis tested by Bellman and coworkers 26 was to attach a string (7F/3F) to the distal end of the stent, and bringing it out via the urethra. This string would then obviate the need for cystoscopy, because it could be gently pulled out to remove the stent when needed, in the office setting. An unforeseen consequence of this approach, however, was that patients could inadvertently pull the string, hence removing the stent prematurely. Subsequently, this technique was modified by attaching the string to the proximal end of the stent and bringing it via the nephrostomy tract to the outside. 27 This modification, like the distal tether, would allow stent removal from the flank without the need for cystoscopy. Our study confirms the feasibility of this approach and attests to the safety and efficacy of placement of a tethered antegrade stent in PCNL.
In this study, the cohort of patients undergoing tubeless PCNL with a tethered antegrade DJ stent experienced significantly reduced levels of pain and needed less analgesia than their counterparts undergoing standard PCNL. Average hospital stay of these patients was less than 24 hours, in comparison with 2 to 3 days in standard PCNL, thereby allowing the majority of patients to be treated as day cases. No patients in the tubeless PCNL group experienced any urinary leak from the percutaneous access site, confirming the effectiveness of kidney drainage provided by the DJ stent. The stents of the tubeless PCNL patients were all removed without cystoscopy or any other procedure, simply by pulling on the tether in an office setting. No difficulty or patient discomfort was noted in doing so. No patient experienced any pain, hematuria, or any other consequence afterward either.
The concept of having an antegrade tether with its outlet in the flank in tubeless PCNL has another application relating to re-look nephroscopy. In a standard PCNL, the tubeless approach is avoided at a time when a second-look procedure is expected for any residual calculi or fragment clearance. With this approach, however, this factor to avoid tubeless PCNL is no more an issue, because the tether allows for re-access whenever needed. This is done by pulling the stent toward the skin, which enables a guidewire to be inserted in this tract toward the pelvicaliceal system. This method re-establishes the original percutaneous tract that was created and allows for any residual calculi/fragments to be removed.
Conclusion
The present study demonstrates that tubeless PCNL with tethered DJ stent provides all the advantages of tubeless PCNL while overcoming its main drawback—namely, need for cystoscopy for stent removal. In addition, it allows re-access to the pelvicaliceal system for second-look nephroscopy if the need arises.
Footnotes
Disclosure Statement
No competing financial interests exist.