
Abstract
Introduction:
The Thermedx Fluid Management System (TFMS) is an automated pressurized irrigation system that allows concurrent temperature control. Developed for use in multiple surgical specialties, it provides settings specific to several endoscopic urologic procedures. The objective of this study was to critically appraise the functional characteristics and precision of the device regarding irrigation warming, pressurization, and flow during semirigid ureteroscopy.
Methods:
Using an in vitro model, the TFMS was assessed using the proprietary urology tubing with and without a short semirigid ureteroscopy/ureteroscope (URS) (7.4F/35 cm Wolf 425612). Pressures and temperatures were measured using continuous digital sensors (Meriam m1550-gi0015, and Taylor Digital Thermometer 9842). Stepwise increases in settings were measured with and without the ureteroscope (from 100 to 200 mm Hg), and with and without the included pressure release valve (preset for 150 mm Hg). Continuous measures (60/min) were recorded and compared with values recorded by the internal unit sensors.
Results:
At room temperature (18.1°C), the starting irrigation temperature was 19.5°C, increasing to 35.5°C after 7.2 minutes at maximum settings (40°C). Irrigation returned to baseline temperature after 6.7 minutes with the heater disabled. The irrigation temperature was not affected by changes in pressure settings and flow rates. The unit's display readings were 4°C–6°C higher than measured at the tip of the ureteroscope. Flow rates detected at the tip of the URS were 2%–8% less than the unit reported. Pressures were between 8%–17% higher using URS than that reported by the unit, and highest values were encountered when the physical safety pop-off valve was removed from the tubing.
Conclusions:
The TFMS provides a pressurized/warmed irrigation strategy for many endoscopic procedures. It is important to note that the system underestimates pressures at the tip of the endoscope, while overestimating the flow rates and temperatures delivered from the scope when utilizing the device.
Introduction
I
A new product by Thermedx Fluid Management System (TFMS) provides an automated alternative, adding digital pressure and temperature control and fluid deficit monitoring. Using an automated system provides several theoretical advantages, including more reliable control, continuous monitoring of pressures, predefined safety thresholds, and alerts for irrigation flow changes, empty bags, or kinked tubing.
The TFMS has been designed to provide irrigation for endoscopic procedures in general surgery, gynecology, anesthesiology, orthopedics, and urology. Procedure-specific profiles specific to urology include laparoscopy, transurethral resections, ureteroscopy, and percutaneous nephrolithotomy (PNL). Based on the selected procedure profile, the firmware automatically limits its settings to operate within predefined safety ranges. These limitations restrict the upper limits of pressure (i.e., 200 mm Hg for ureteroscopy vs 80 mm Hg for transurethral resection [TUR]), and enable alarms specific to the procedure (i.e., fluid absorption alarm during transurethral prostate resection [TURP]). At the conclusion of each case, a report can be generated (and printed) to document the total endoscopic time, fluid used, average temperature, and fluid deficit.
The objective of this study is to assess both the heating and pressurization functionality of the TFMS using an in vitro rigid ureteroscopy model. The characteristics evaluated include the rate of temperature change, pressure/flow relationships, and the precision of TFMS continuous monitoring systems.
Methods
The TFMS (Fig. 1) was used in this study in combination with the Thermedx Disposable Urology Tubing Set (Thermedx LLC). Pressure settings were adjustable by increments of 5 mm Hg, from 60 mm Hg to a maximum of 200 mm Hg. The Ureteroscopy Mode was selected and pressures recommended for ureteroscopy were limited to 100–200 mm Hg. The pressure and temperature measurements were performed using a continuous digital pressure transmitter (Meriam m1550) and a continuous-read digital thermometer (Taylor Digital Thermometer 9842), respectively.

Thermedx Fluid Management System unit.
Using in vitro models, the TFMS settings were assessed with and without a short semirigid ureteroscope (7-4F, 31 cm Wolf 425612). Pressure, flow, and temperature measurements were performed through the provided tubing set, using room temperature 3L irrigation bags, and then repeated with the ureteroscope attached. Pressure settings for ureteroscopy were performed at 100–200 mm Hg and measured at the tip of the scope.
Temperature Study
Using room temperature irrigation, the initial fluid temperature was recorded flowing through the scope with the TFMS heater off. The maximum temperature setting (40°C) and pressure setting of 100 mm Hg were used, and the time to maximum temperature was recorded by placing the temperature probe 1 cm from the tip of the ureteroscope. This setting was held for 10 minutes after measured temperatures peaked and then the heater was disabled and the time to return to the baseline was recorded. All temperatures recorded at the end of the scope were correlated to the temperature TFMS internal sensor readings displayed on the front panel.
To test the consistency of temperature control at various pressure settings, maximal fluid temperature was achieved, then pressures were sequentially increased by 20 mm Hg, while recording both measured and displayed temperatures.
Pressure and Flow Studies
Using room temperature irrigation, the TFMS was set to 100 mm Hg and pressures were measured at the tip of the scope (Fig. 2). Increments of 20 mm Hg were used and pressures recorded. These settings were then repeated and flow rates were measured at the tip of the scope by determining the amount of time required to fill a 100cc beaker. Trials were repeated 10 times for each setting, and two-tailed Student's t-tests were used to compare measured vs displayed flow rates (significance p<0.05).

Setup with a ureteroscope.
Pressure tests were repeated with and without the use of the physical pressure release valve (preset for 150 mm Hg) located immediately proximal to the female luer-lock fastener (Fig. 1). At the time of the study, the TFMS had been approved for 200 mm Hg used for ureteroscopy, although the tubing sets had not been updated.
The ureteroscope was coupled to the pressure sensor by using a 3/4 inch threaded step-down pipe fastener to secure a 1.5 inch section of suction tubing to the sensor port. An adjustable biopsy port (Gyrus ACMI) was inserted into the tubing using a pipe fitters tape (to prevent leakage), and was tensioned around the beak of the ureteroscope to provide a watertight seal. When the tubing was used alone, the female luer lock fitting from the tubing was attached to a male luer lock fastener, which was inserted into the pressure sensor tubing connector. When the pressure valve was removed from the tubing set, it required removal of the luer lock fitting; therefore, a metal stopcock was used to connect the free end to the ureteroscope.
Results
At ambient room temperature (18.1°C) in the operating room, the starting irrigation temperature was 19.5°C. Setting the TFMS to maximum (40°C) and pressure to 100 mm Hg, a maximum temperature of 35.5°C was reached after 7.2 minutes. These settings were maintained for 10 minutes (to ensure no further changes), then the heater was disabled and irrigation temperatures reached baseline after 6.7 minutes.
Increasing irrigation pressure from 60 to 200 mm Hg in 20 mm Hg increments did not lead to a decrease in nadir maximum temperatures. However, temperatures measured at the tip were consistently 5°C lower then that displayed on the TFMS monitor.
Measuring pressures without the ureteroscope TFMS consistently reported lower pressures. At 100 mm Hg settings, the mean displayed pressure was 104 mm Hg, while the measured pressure was 9.32% higher (113.69 mm Hg). Increasing by 20 mm Hg, up to 180 mm Hg, a similar 10% discordance was noted (measured: 197 mm Hg). When settings were increased to 200 mm Hg, the difference decreased to 4.6% (209 mm Hg) as the mechanical pressure release valve caused irrigation leakage to reduce the delivered fluid pressure (Table 1).
Measured pressures were always greater than pressure settings.
UTS=ureteroscopy/ureteroscope.
With the ureteroscope in place, the pressures were significantly increased at 100 (112.1 mm Hg, p=0.03) and 200 mm Hg (216.54 mm Hg, p<0.001). The mechanical pressure release valve functioned appropriately, with minor leakage at 160 mm Hg, and a steady flow (from the valve) noted at 200 mm Hg. However, it is important to note that the peak pressures at the tip of the ureteroscope with the safety valve in place well exceeded the 150 mm Hg rating; reaching 180 mm Hg at the 200 mm Hg setting.
When the mechanical pop-off valve was removed, pressures were significantly increased at 100 mm Hg (115.9 mm Hg p=0.0012). At 200 mm Hg, there was a 15% increased pressure at the tip (230 mm Hg) without the use of the release valve (Table 1).
Although pressure readings displayed by the unit were lower than the measured values, the displayed flow rates were higher. At 150 mm Hg setting, the unit's displayed flow rate was 175 mL/min, whereas measurements through ureteroscopy/ureteroscope (URS) were 160 mL/min (−8%).
Increasing the settings to 180 mm Hg, the resulting displayed flow was 185 mL/min, while the actual flow was 180 mL/min. At maximal pressure (200 mm Hg) settings, the displayed flow was 194 m/min, while the measured flow plateaued at 182.9 mL/min (p=0.001) (Fig. 3). At all other pressures, the measured flow was 3%–9% lower than the displayed flow rate (160 mm Hg p=0.031, all other settings p<0.001).
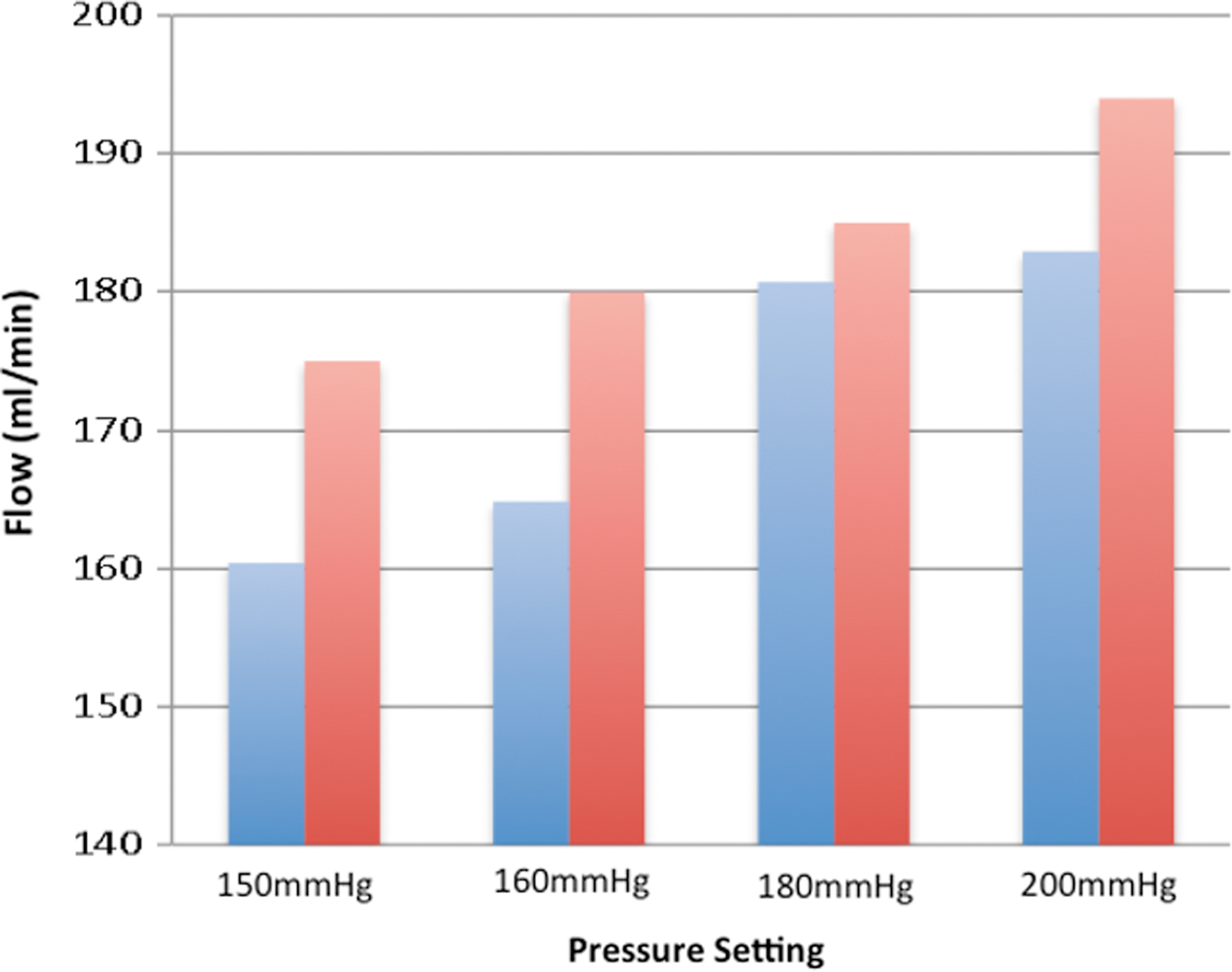
Measured flow rate through ureteroscope (blue) compared with displayed flow rate (red). (All values p<0.05.)
Discussion
The TFMS is a new automated pressure/temperature controlled irrigation system, which allows refined control of irrigation during endoscopic procedures. In this study, the test unit was found to overestimate the temperature and flow rate of fluid delivered by the scope, while underestimating the pressure.
Temperature monitoring is performed using internal sensors; it is possible that the irrigation may cool while traversing the distance between the tubing and tip of the ureteroscope. The time to reach a peak temperature of approximately 7 minutes may decrease the value of this feature for short procedures, such as cystoscopy, TURBT, and distal ureteroscopy, yet may still have value for longer procedures such as PCNL and intrarenal ureteroscopy. The consistency of temperature across a range of pressure settings and flow rates suggests that the heating element adequately adjusts to these variables.
Pressure measurements sensed internally may not account for changes in the luminal diameter across the transitions from tubing to connector to scope. Variations in the length of scope and tubing kinks could further impact the reliability of the displayed pressures. The pressure differential between the scope tip and measured values were relatively small (4%–15%). Several integrated safety mechanisms reduce the potential for large intrarenal pressures. Complete occlusion of the irrigation channel triggered the unit's alarm and automatically shut the pump off. Pressures over 150 mm Hg lead to leaking at the mechanical pressure release valve on the most distal aspect of the tubing. This valve provided a pressure ceiling of 180 mm Hg at the tip of the ureterosope. Without the valve in place, the average pressure at the tip of the ureteroscope was 230 mm Hg, although unsustained pressures of 250 mm Hg were encountered.
Currently, no evidence exists for the benefits of warmed irrigation in ureteroscopy. Extrapolating from other endoscopic procedures is difficult as procedure times and vascular characteristics are unique to each surgery. A meta-analysis accounting for all endoscopic trials utilizing warmed and room temperature fluids was performed in 2011. 1 Included were 13 randomized trials involving transurethral prostate resections, PNL, hysteroscopy (with resection), and arthroscopy. It was found that perioperative core temperatures and postoperative shivering were significantly affected by using room temperature irrigation. Only three studies reported blood loss (TURP, hysteroscopy with resection, and PNL), and all showed a mild decrease in bleeding with a warmed solution. Procedure times ranged from 30 to 100 minutes, and total fluid volumes ranged from 4 to 23 L. Although the lower limits of surgical times and fluid volumes are similar to those encountered during ureteroscopy, it is difficult to ascertain whether warmed irrigation would benefit our patients.
Fluid absorption during ureteroscopy has been reported to occur at a rate of 1 mL/min absorption using irrigation pressures of 200 mm Hg. 2 In comparison, absorption during TURP can be 25 mL/min at much lower bladder pressures of 12–30 mm Hg. 3 Arthroscopy fluid absorption may differ with the specific joint being instrumented and have been reported to be ranging from 1 to 3 mL/min. 4,5 These procedures all use significantly lower irrigation pressures (TURP 60–120 mm Hg, arthroscopy 30–70 mm Hg) than required for ureteroscopy.
Normal pressures in the human collecting system are estimated to be below 20 cmH2O. 6 At any pressure, pyelovenous, pyelolymphatic, pyelotubular, pyelointerstitial, and pyelosinus backflow can occur leading to fluid absorption. 7 Exposure to higher intrarenal pressures as well as pathologies such as hydronephrosis and renal ischemia can cause forniceal tears, 8 increasing the amount of fluid that could be absorbed. 9 In a porcine kidney model, Blew et al. compared three irrigation devices through a rigid ureteroscope and found flow rates were 200 mL/min with gravity (100 mm Hg), 450 mL/min with pressure bags (300 mm Hg), and 220 mL/min with a foot pump. 10 All but gravity provided significantly higher flow rates than encountered in this study, due to the increased pressures generated by the other devices.
In a cadaveric study, irrigation pressures of 200 cmH2O (161 mm Hg) yielded intrarenal pressures of up to 60 cmH2O, with flow rates of 25 mL/min. The use of ureteral access sheaths reduced intrapelvic pressures to 20 cmH2O (14.7 mm Hg), and improved flow rates to 30–50 mL/min. 11 These flow rates are lower than our measured values, as we used an open system in contrast to a kidney with fixed volumes and a single narrow drainage site.
Currently, there are no available data to assess clinical benefits for using this device. Theoretically, more consistent pressures are provided in comparison to pressure bags. Practically, it can help streamline irrigation bag changes, fine tune pressures allowing for adequate visualization, and easily facilitate fluid warming when required. Where fluid absorption is important, the unit can be utilized to calculate differential return and alert the user when concerning levels have been reached. To fully understand the benefits and limitations, a prospective study is required.
Some limitations of this study include the utilization of in situ experiments as compared with in vitro analyses. Although each component can be judged individually in our study, it is important to consider new equipment based on its clinical applicability and cost (yet to be determined). In regard to our measurements, all temperatures were taken with a NIST calibrated digital thermometer. The pressure sensor was fixed to the ureteroscope using tubing with a lumen slightly larger than the outer diameter of the female coupling port. Although the sensor sits within the port, this discrepancy in diameter may reduce the measured pressures, thus leading to an under-representation of measured pressures. In effect, this could mean there is a slightly greater difference between the irrigation pressure at the scope tip and the pressure displayed on the unit.
In summary, the TFMS provides several functions in one unit. It is important for the user to recognize that temperature settings and display readings are higher than that delivered at the tip of the endoscope, while pressure settings are 4%–10% higher at the tip and the flow rates are lower at the tip than reported by the device. Although values of the internal sensors did not match those at the end of the scope, deviations of pressure, flow, and temperature were not great in magnitude.
Conclusion
The TFMS is as an automated pressure and warming strategy for ureteroscopy that performs within expected parameters. Discrepancies in the temperature, flow, and pressure occur with predictable limitations and at magnitudes that do not significantly limit functionality or safety.
Footnotes
Disclosure Statement
No commercial associations or conflicts of interest.