
Abstract
Purpose:
To assess the impact of listening to preferred music on relieving male patients' pain and anxiety during flexible cystoscopy.
Patients and Methods:
A total of 124 male patients were admitted to our hospital for flexile cystoscopy by a single urologist between January 2013 and September 2013 and randomized to two equal groups. Group 2 included 62 patients who could select and listen to their preferred music during flexible cystoscopy. Group 1 included 62 patients who were unable to listen to the music. All patients were administered the same amount of lidocaine (10 mL) for 3 minutes for local anesthesia before flexible cystoscopy. A visual analog scale (VAS) ranging from 0 to 10 was used to assess patients' pain feeling after the cystoscopy procedure. Anxiety levels were calculated according to the State Instrument of State-Trait Anxiety Inventory (STAI-S), and the pulse rate were recorded 5 minutes before and immediately after the procedure. The duration of the procedure of each group were also analyzed.
Results:
Statistically significant differences were detected between group 1 and group 2 in the mean pain score on VAS (2.53±1.34 vs 1.63±1.09, P=0.002, Mann-Whitney U test), mean postprocedural State Anxiety Inventory pain score (39.4±6.5 vs 34.5±5.8), and postprocedural pulse rate (79.8±5.5 vs 76.0±7.3) (P<0.001 for both, t test). Patients who listened to their preferred music experienced less discomfort and lower anxiety at cystoscopy. Patient age, duration of the procedure, preprocedural STAI-S, and preprocedural pulse rate of each group were comparable.
Conclusion:
Listening to preferred music during flexible cystoscopy is an easy way to improves male patients' comfort and reduce their anxiety. It could be recommended for male patients.
Introduction
F
To our knowledge, there has been no research on reducing paitents' discomfort and anxiety during flexible cystoscopy by music intervention. Because male patients suffer more discomfort than females 3 and most female patients undergo cystoscopy by rigid cystoscope at our institute, we performed a randomized controlled study for male patients to estimate the effect of music engagement on responses to pain and anxiety during flexible cystoscopy.
Patients and Methods
Participants, exclusions, and ethics statement
One hundred and twenty-four male patients admitted to our institute for flexile cystoscopy by the same urologist between January 2013 and September 2013 were enrolled. Ethics review was approved and written approval was obtained from the Institutional Review Board of our hospital (Shanghai Changhai Hospital); full written and informed consent was provided by every patient. Indications for flexible cystoscopy were hematuria and surveillance for bladder tumors. Exclusion criteria were other procedures such as urethral dilation, biopsies, stent placement, and stent removal. Patients undergoing manipulation of the lower urinary tract, patients with a history of chronic pelvic pain syndrome, or with a history of diabetes or arrhythmia were also excluded from the study.
Randomization and procedure
All 124 patients were informed of this study, then randomized into two equal groups. A research nurse had a random number list to ensure an equal number in two groups. Patients were randomized as follows: Group 2 included 62 patients who could select and listen to their preferred music during flexible cystoscopy. Four major kinds of music—classical music, Chinese folk music, popular music, and foreign music—were ready for patient selection. A wide variety of CD and audio equipment was available in the operating room. Group 1 included 62 patients who were unable to listen to the music. The same volume of 10 mL 2% lidocaine jelly was administrated intraurethrally for 3 minutes before flexible cystoscopy for every patient as local anesthesia. The instrument for flexible cystoscopy included a 16F flexible cystoscope (Olympus CYF-5A), a color video monitor (Olympus OEV-191H), and a digital camera (Olympus OTV-S7).
Pain measures
A visual analog scale (VAS) ranging from 0 to 108 was used to evaluate pain. After flexible cystoscopy, patients wrote down their pain feeling on a VAS form. According to the Collins definition, “no pain” was a score of 0, “mild pain” was a score of 1 to 3, “moderate pain” was a score of 4 to 7, and “severe pain” was a score of 8 to 10. 8 The duration of the procedure of each group was also recorded and analyzed.
Anxiety measures
Anxiety levels were calculated 5 minutes before and immediately after the procedure according to the State Instrument of State-Trait Anxiety Inventory (STAI-S). 9 STAI-S is a scale commonly used to measure the trait and state anxiety that contains 20 self-report items. It can measure tension, worry, and apprehension that the respondent experiences at this moment or in current circumstances (state anxiety). The respondent reports on the frequency that he/she experiences symptoms on a 4-point scale (1: not at all; 2: somewhat; 3: moderately so; 4: very much so), and higher score means a greater anxiety level. 9 The duration of the procedure and pulse rate were recorded and analyzed. A research nurse was in charge of recording the patients' pulse rate 5 minutes before and immediately after the procedure by taking the pulse.
Data analyses
SPSS 13.0 was used for data analysis. The Mann-Whitney U test was used to compared the VAS score between the two groups, with P<0.05 considered statistically significant. The independent-samples t test was used to determine differences in preprocedural and postprocedural STAI-S, preprocedural and postprocedural pulse rate, ages, and duration of procedure between the two groups. The chi-square test was used to determine differences of count data between groups.
Results
Of the 124 flexible cystoscopies, 46 (24 in group 1 and 22 in group 2) were performed for diagnostic purposes, with the remainder surveillance procedures; 43 (23 in group 1 and 20 in group 2) were performed for the first time, with the remainder repeated cystoscopy. Age distribution (t test), duration of the procedure (t test), preprocedural pulse rate (t test), ratio of cystoscopy for diagnostic purpose (chi-square), and ratio of patients who had repeated cystoscopy (chi-square) in the two groups were all comparable (both P>0.05) (Table 1).
SD=standard deviation; STAI-S=State Instrument of State-Trait Anxiety Inventory.
The mean pain score on VAS was 2.53±1.34 in group 1 and 1.63±1.09 in group 2. STAI-S score decreased in both groups after the procedure: The mean postprocedural STAI-S score was 39.4±6.5 in group 1 and 34.5±5.8 in group 2. Mean pain score and mean postprocedural anxiety level (STAI-S score) in group 2 were statistically significantly lower than those in group 1 (P<0.001 for both) (Figs. 1, 2). Statistically significant differences were also detected between group 1 and group 2 in the postprocedural pulse rate (79.8±5.5 vs 76.0±7.3, P=0.002) (Fig. 3).
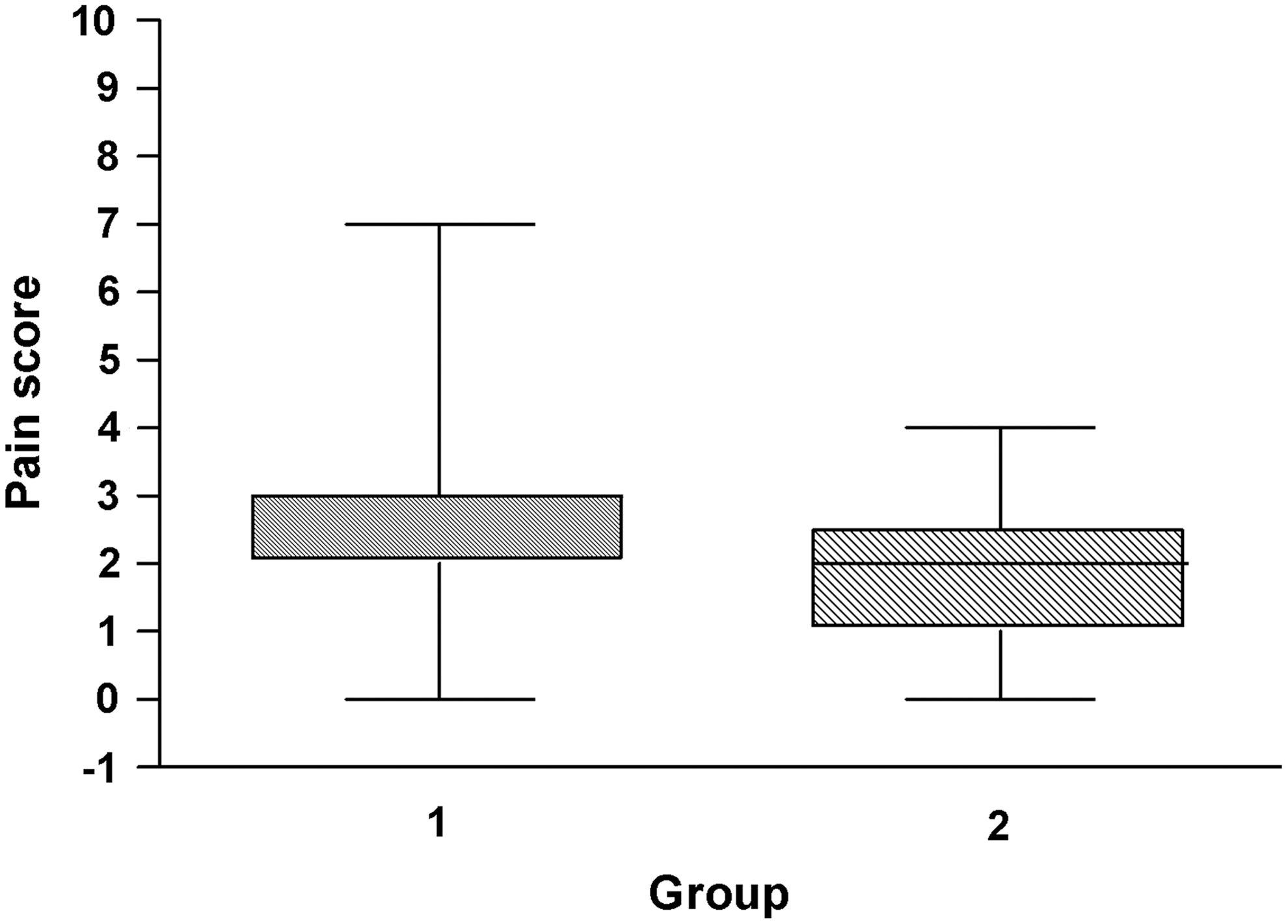
Box plots of pain score (visual analog scale [VAS]) showed difference in pain level between the two groups. VAS score was 2.53±1.34 in group 1 (no music) and 1.63±1.09 in group 2 (music); patients who listened to their preferred music experienced less discomfort at cystoscopy.
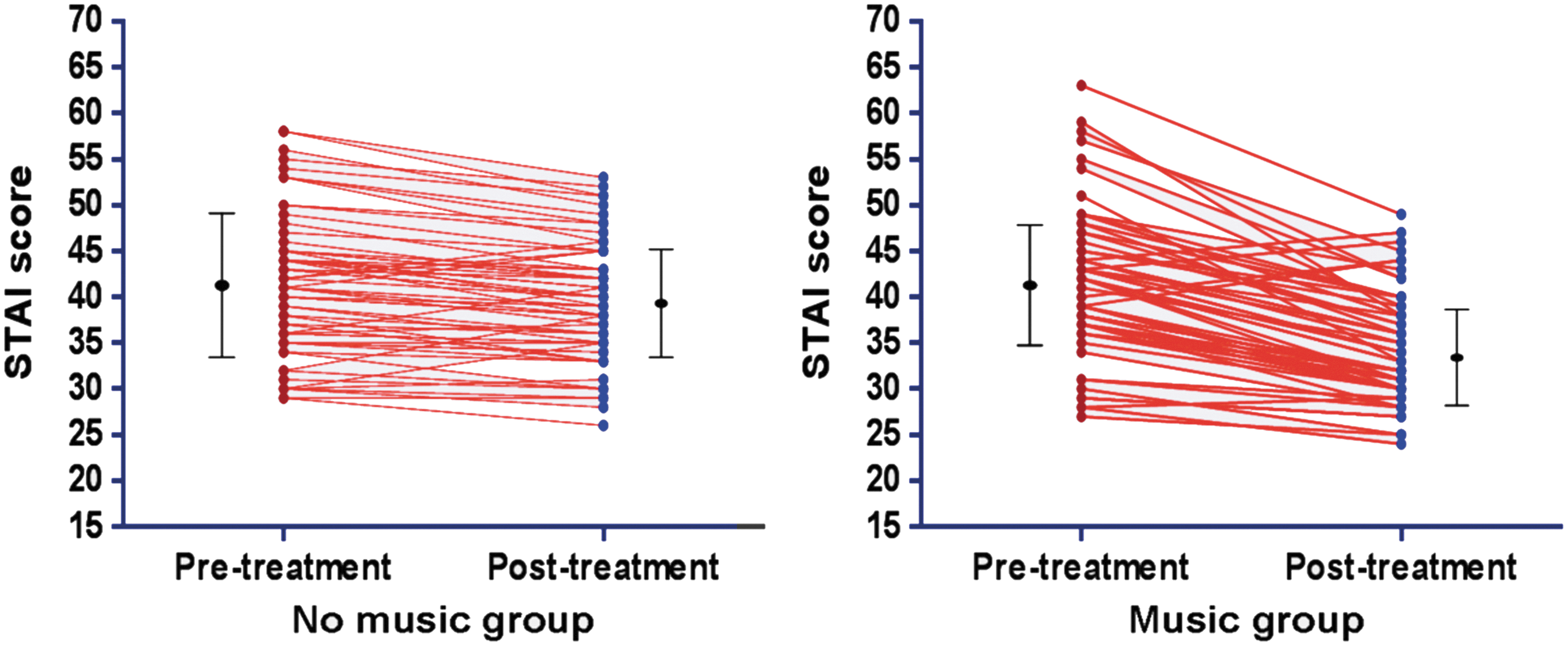
Data point graphs for no-music and music groups pre- and post-treatment with mean and interquartile ranges. The graphs showed reduction of the anxiety levels (State Instrument of State-Trait Anxiety Inventory [STAI-S] score) in both groups after flexible cystoscopy, but the postprocedural STAI-S score in the music group (34.5±5.8) was less than the no-music group (39.4±6.5), P<0.001.
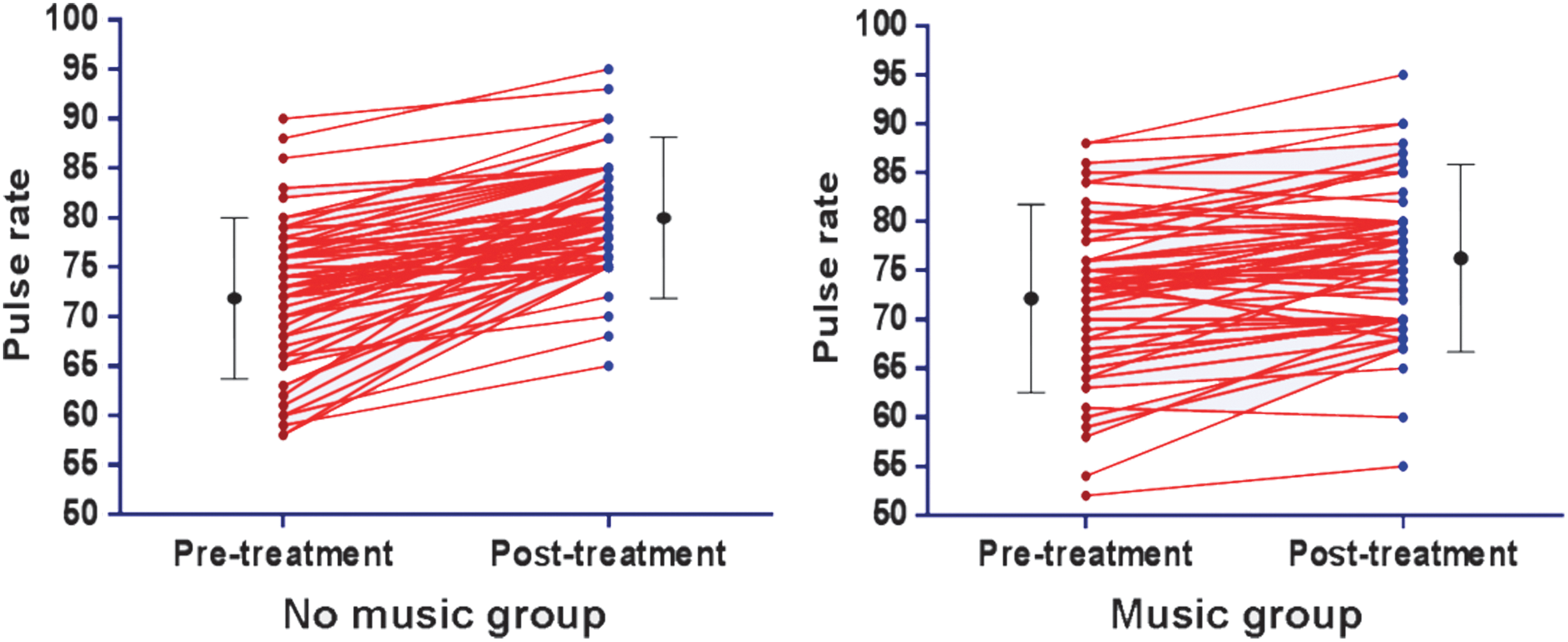
Data point graphs for no-music and music groups pre- and post-treatment with mean and interquartile ranges. The graphs show increase of pulse rate in both groups after flexible cystoscopy, but the postprocedural pulse rate in the music group (76.0±7.3) was less than in the no-music group (79.8±5.5), P=0.002.
Especially when stratified analysis was performed and postprocedural STAI-S and pain scores were compared between subgroups, it was found that music engagement was effective for patients receiving flexible cystoscopy for surveillance or diagnostic purposes, as well as those undergoing their first or repeated cystoscopy, in reducing their pain and anxiety (Table 1). Classification of pain according to VAS scores in the two groups was also demonstrated in Table 1.
Discussion
Flexible cystoscopy has greatly dereased patients' discomfort and made cystoscopy more tolerable, especially for male patients; however, pain is still inevitable during this procedure. So many studies had examined different methods to reduce male patients' discomfort, such as assessment of the volume of lidocaine, 10 increasing hydrostatic pressure by squeezing the irrigation solution bag, 11 cooled lignocaine gel, 12 simultaneous visualization, 13 application of nitrous oxide inhalation, 14 slow delivery of local anesthetics, 15 use of a special flexible cystoscope sheath, 16 and transcutaneous electrical nerve stimulation. 17 Controversy still exists, however. Some randomized controlled trials and meta-analysis reported that there is no significant difference between lidocaine gel and placebo in the efficacy of reducing pain for male patients during flexible cystoscopy, 18,19 and Cornel and colleagues 20 reported that the pain score of men undergoing flexible cystoscopy could not be obviously affected by simultaneous visualization.
In recent years, several studies had confirmed that music could help patients experience less pain and anxiety during other endoscopic procedures, such as bronchoscopy, gastroscopy, colonoscopy, colposcopy, and hysteroscopy. 21 –25 Similarly, in our trial, we demonstrated that music could improve psychological and physiologic parameters related to pain and anxiety, the VAS score, and that the postprocedural STAI score among patients who listened to their preferred music were significantly lower, either in the patients with surveillance cystoscopy or diagnostic cystoscopy, and either in the patients with first time cystoscopy or repeated cystoscopy. Compared with group 1, the decrease of STAI score in group 2 was significantly more, but the increase of pulse rate was significantly less after the procedure, indicating that music intervention might smooth patients' mood, reduce their discomfort, and relieve their anxiety. Just recently, Yeo and coworkers 26 also stated that listening to music during rigid cystoscopy decreased anxiety, pain, and dissatisfaction in male patients. To a great degree, this statement is supported and confirmed by our results.
The mechanism of music playing an adjuvant therapeutic role in reducing pain and anxiety is sophisticated. Mitchell and colleagues 27 reported that listening to preferred music might provide an emotional distraction and consequently reduce the feeling of pain and the concomitant negative emotional experience. According to functional magnetic resonance imaging analysis, Valet and associates 28 stated that distraction could increase the activation of the cingulo-frontal cortex, the periaqueductal gray, and the posterior thalamus significantly; they also found that distraction could be significantly associated with reduction of pain intensity, unpleasantness, and pain-related activation in some brain areas, especially in the “medial pain system.” The study by Valet and associates 28 also confirmed the opinion of Cook 29 that music therapy could divert patients' attention from fear of pain and that is the reason why so many clinical research studies had reported music therapy could be widely used in both acute pain and chronic pain treatment. 30,31 In addition, some studies even reported that music intervention could reduce the dose of analgesic and sedation drugs in invasive procedures. 23,32
Careful consideration is needed when selecting music for the purpose of releasing both pain and anxiety. Some studies demonstrated patient selection was better 27 ; on the contrary, some stated that researcher-selected music would be most effective, because researcher-selected music could take into account factors that had been known and accepted to be effective in relaxation and pain control. 7,33 –35 In our trial, we combined the patient preference and researcher selection. We selected the music according to experts' recommendations, which should fulfill the conditions such as moderate volume, gentle timbre, smooth melody, few percussive instruments, and without strong rhythm, 7,35 then divided these songs and melodies into four major kinds. Therefore, patients in our study could select their preferred music style that could both match their taste and meet the standard of “theraputic music.”
This study has some possible limitations. First, This is a small and single-center study; a multi-center and large sample study could be more convincing from which to draw a meaningful conclusion. Second, the cystoscopist was not blinded during the procedure, so it is potentially possible that patients in group 2 could get more careful manipulation than those in group 1. Third, there were no specific orientations for patients to watch the flexible cystoscopy procedure, so potentially simultaneous visualization of the procedure might divert attention and reduce discomfort. 13,36 Fourth, although some studies had confirmed that local anesthetic played a role just as a placebo 18 and might make patient exerience more pain when the physician injected the lidocaine jelly into the urethera, 37 leading to a conclusion that local anesthetic might be unnecessary, we still used lidocaine jelly for every patient in our study because of the clinical routine and patient demand for topical anesthesia. Fifth, VAS and SATI scores are partly subjective; some more objective parameters, such as the bispectral index, 38 were not used. Despite these limitations, our study demonstrated that listening to preferred music during cystoscopy reduces feelings of pain and enhances satisfaction and compliance during this invasive procedure.
Conclusion
Patients who were listening to preferred music experienced less discomfort and anxiety at flexible cystoscopy. As a nonpharmacologic and noninvasive intervention, music might be one of the simple but important strategies in office urology for patient satisfaction.
Footnotes
Disclosure Statement
No competing financial interests exist.