
Abstract
Purpose:
To assess epidemiologic characteristics, clinical and pathologic patterns of presentation, and treatment strategies in a contemporary population with renal masses (RMs).
Methods:
The Clinical Research Office of the Endourological Society collected prospective epidemiologic, clinical, and pathologic data on consecutive patients with RMs who were treated during a 1-year period in 98 centers worldwide. Preoperative assessment and treatment were performed according to local clinical practice guidelines.
Results:
From January 2010 to February 2012, 4288 patients (4355 cases, 4815 tumors) were treated for a RM. The mean age of the cohort was 61.5 years, and the ratio male:female 1.8:1. Caucasians represented 75% of the population, and the median body mass index was 27. The cohort exhibited a high rate of comorbidity (65.6%), including a 48.5% rate of hypertension; one-third of patients had a combination of two or more comorbidities. One-third of patients (36%) had risk factors for renal-cell carcinoma (RCC), of which smoking and obesity were the most common. Diagnosis was incidental in 67% of cases, and 22.2% of cases had chronic kidney disease stage ≥III at presentation. Median radiologic size was 44 mm (range 2–300 mm) and 68% were cT1. Radical nephrectomy and nephron-sparing surgery (NSS) including ablation were performed in 52% and 46% of cases, respectively, while 3.6% of cases were actively surveyed. Median pathologic size was 43 mm (range 2–300 mm) and 63% of the RCCs were pT1.
Conclusions:
Current patterns of presentation of RMs are consistent with the decreasing trends in age and clinical or pathologic size and increasing incidental diagnosis. Patients exhibit a considerable basal comorbidity and presence of risk factors for RCC. Half of the cases are treated by a nephron-sparing modality with an increase in the penetration of NSS techniques in the contemporary urologic practice.
Introduction
T
To overcome the above mentioned biases, in 2010, the Clinical Research Office of the Endourological Society (CROES) launched a multi-institutional registry on RMs. The primary objective of this first report from the CROES Global Renal Mass Study is to assess general clinical and pathologic patterns of presentation and treatment in a contemporary global population with RMs.
Patients and Methods
Study protocol
The CROES Global Renal Mass Study was initiated in January 2010. Participants were urologists invited to include all RM patients who were treated in their department during a 1-year period. Inclusion criteria were: Age ≥18 years, diagnosis of RM and any type of treatment, including active surveillance. The study protocol included epidemiologic characteristics; risk factors for RCC, basal clinical, laboratory, and radiological measurements, type of treatment, pathologic and perioperative variables, and follow-up (radiologic and renal function) variables.
To capture the current diagnostic practice, the study investigators were asked not to modify their diagnostic protocols and not to perform any additional test, intervention, or pathologic investigation outside their routine practice. When more than one tumor was present, clinical and pathologic stages were based on the largest or more advanced tumor. Clinical and pathologic stages were assigned according to the 2002 tumor-node-metastasis classification. 9 Thrombus level was further defined according to the Mayo classification. 10 Chronic kidney disease (CKD) stage was calculated according to the Modification of Diet in Renal Disease formula. 11 Creatinine and hemoglobin levels were recorded on postoperative day 1 and postoperative complications during the hospital stay.
All participating centers received approval by their Institutional Research Board (IRB) or Institutional Ethics Committee when required, and all accepted the Data Transfer Agreement. If IRB approval was not needed, the centers agreed to comply with the guidelines usually in place when IRB approval is granted. Centers were asked to complete the follow-up for at least 5 years after inclusion according to local protocols.
The authors of this report were invited by the CROES council to form an international representative Steering Committee responsible for directing the CROES Global Renal Mass Study. They are members of the Endourological Society and were selected based on their recognition as experts in the treatment of patients with RMs.
Data collection
Data were electronically collected and patients deidentified. Centers were asked to report data not routinely collected as not available (NA) whereas data not provided were classified as missing data. Patients were included more than once if different treatments were performed (e.g., surgery followed by medical treatment because of progression, bilateral tumors treated in two different sessions). The total number of treatments included in more than one session was categorized as cases. The database was designed to identify patients and cases and to capture changes in treatment (e.g., during active surveillance) or new treatments during the full follow-up period.
The database was censored for inclusion in February 2012, and a data audit was conducted according to the rules of CROES. 12 Centers were excluded from participation if fewer than six patients were included; if the patients were nonconsecutive in the 1-year inclusion period; if there was no response to the audit; if there were cases included without data; and when investigators could not provide certainty on the prospective data collection. Subsequently, the database was locked, checked for consistency, and cleaned before proceeding to analysis.
Data analysis
Dichotomous and categorical variables were expressed in frequencies and percentages. Continuous variables were expressed in means, standard deviation, or medians and range depending on the type of variable. Statistical analysis was performed using IBM SPSS Statistics programming software version 19. Statistical significance was set at <0.05.
Demographic variables (age, sex, and ethnicity) and clinical data (body mass index [BMI], comorbidity, and risk factors) were calculated on number of patients. BMI categorization followed the World Health Organization (WHO) classification. 13 Renal function was assessed by cases because it was prone to vary depending on previous renal interventions. Clinical and pathologic stage were checked in all cases and assigned based on specific radiologic and pathologic features (size, perirenal fat, adrenal and venous invasion) included in the database.
Results
A total of 4288 patients (4355 cases) were treated for a RM during the 1-year period in 98 centers. Participating centers are indicated in the Addendum. Figure 1 shows the distribution of cases per continent. Europe included 69.2%, the Americas 21%, Asia 8.0%, Australia 1.2%, and Africa 0.5% of the cases. The number of participating centers per country ranged from 1 to 14 and the number of cases per country from 10 to 702 (Fig. 2). The number of cases per center varied from 6 to 216.
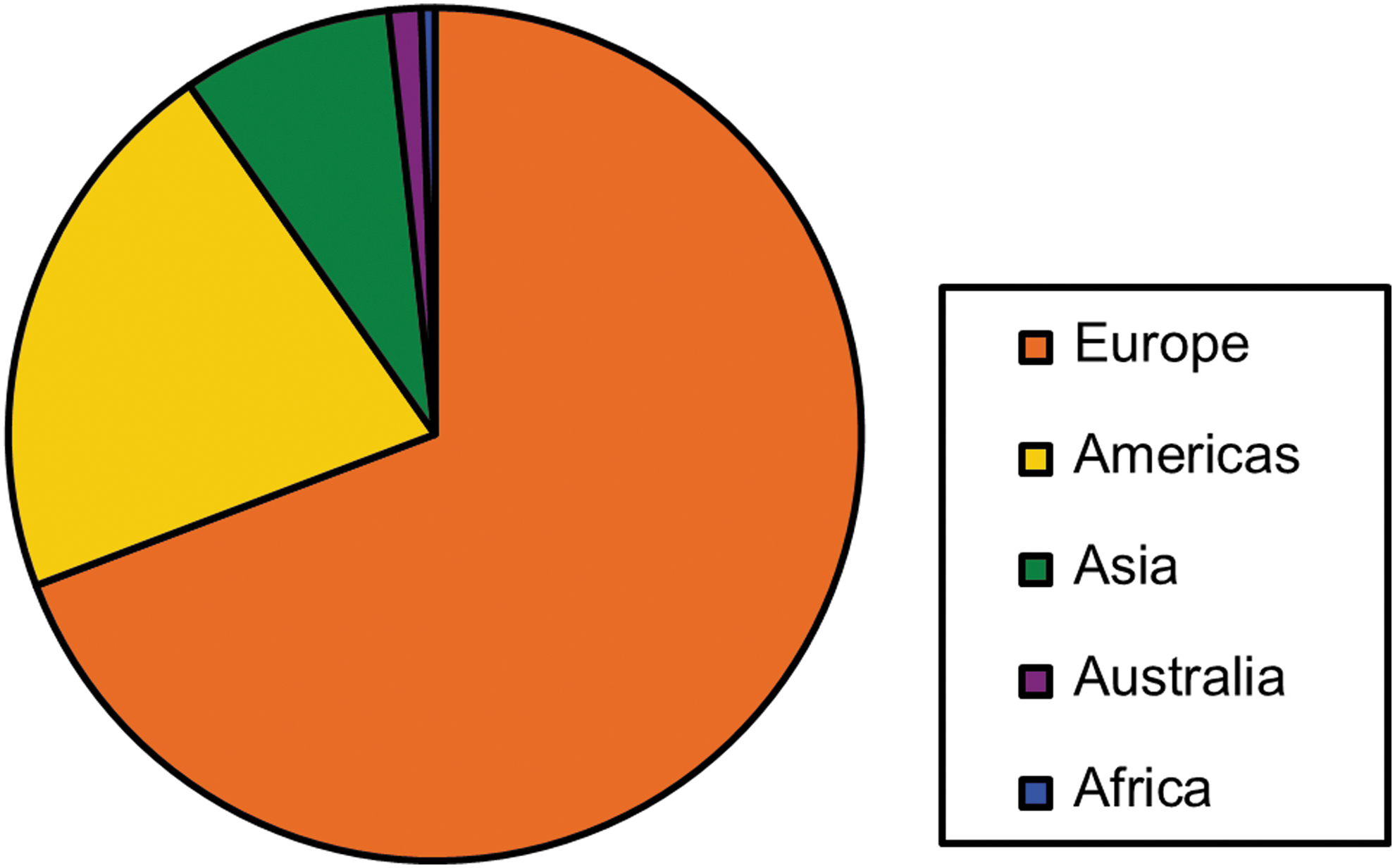
Cases enrolled per continent in the Global Renal Mass Study.
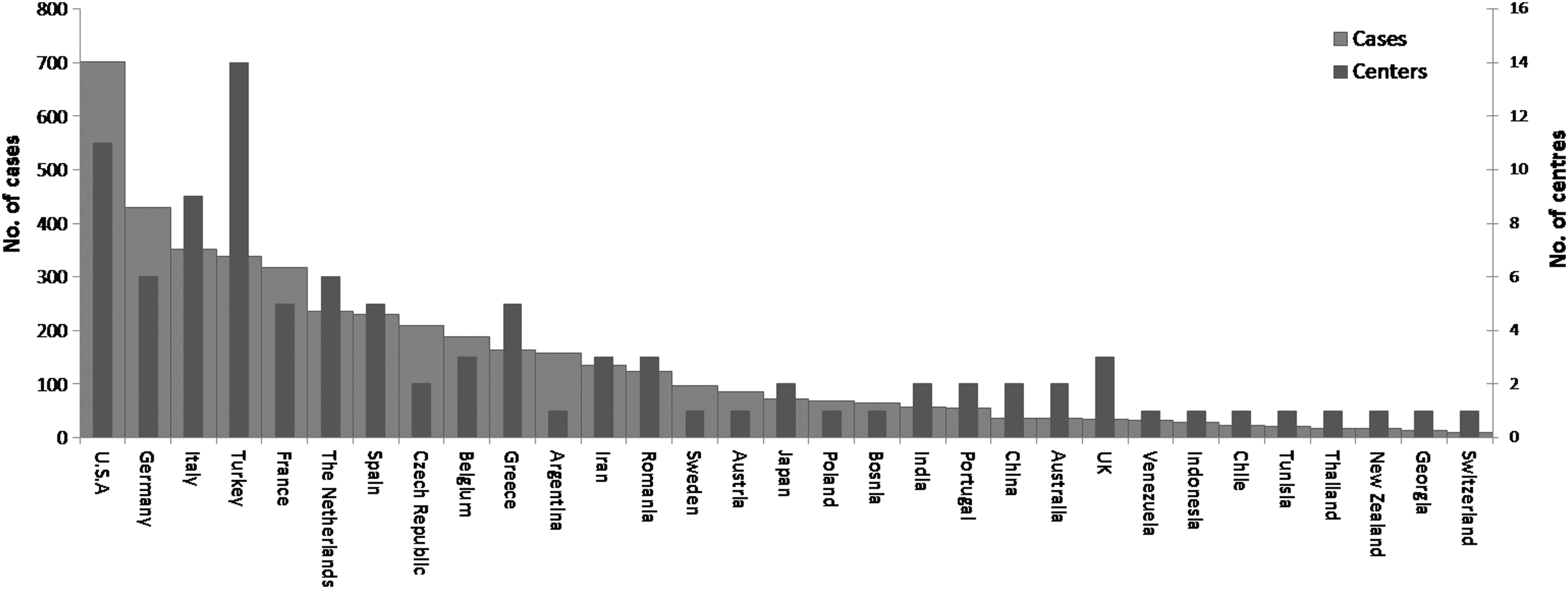
Number of participating centers and patients enrolled per country in the Global Renal Mass Study.
Patient characteristics
The male:female ratio was 1.8:1. Demographic and baseline clinical patients and tumor characteristics are displayed in Table 1. Missing data and NA data are shown for each of the primary variables. For sex and ethnicity, NA and missing data were merged. Age distribution is shown in Figure 3.

Distribution of age among all patients.
Excluded cases in dialysis, previous kidney transplant, or without necessary data for MDRD calculation.
Interventional includes any type of surgical or radiologic guided modality of treatment.
Symptoms prevalence calculated over number of cases. IVC-syndrome (n=9) and lung embolism (n=10) are left out because very few patients presented with this symptom.
Tx cases with insufficient data.
IQR=interquartile range; NA=not available; BMI=body mass index; DM=diabetes mellitus; RCC=renal-cell carcinoma; CKD=chronic kidney disease; MDRD formula=Modification of Diet in Renal Disease formula (estimated glomerular filtration rate=32788×serum creatinine−1.154×Age−0.203×[1.212 if black]×[0.742 if female]).
Overall, 2814 (65.6%) patients presented one or more comorbid conditions at diagnosis. Hypertension alone, or in combination with other conditions, was the most prevalent comorbidity reported in 48.5% of patients. One-third of patients had a combination of two or more c-morbidities. One-third of patients had a risk factor for a RM, of which smoking (21.7%) and obesity (overall 22.1%, males 20.9%, females 24.1%) were the most common. A previous cancer other than RCC was reported in 7.8% of patients. Excluding those patients with renal replacement therapy or transplantation, CKD stage ≥III was present in 22.2% of cases at the time of diagnosis. On case level, age, hypertension, and clinical tumor size were positively correlated to a higher CKD stage (Pearson correlation coefficient (PCC) 0.31, P<0.001; PCC 0.13, P<0.001; PCC 0.06, P<0.01, respectively).
Clinical tumor characteristics
The total number of clinical tumors reported was 4815. The majority of tumors were diagnosed as an incidental finding (67%). Macroscopic hematuria and flank pain were the most prevalent symptoms in patients with these symptomatic tumors. Overall, only one tumor was identified in 92.1% of cases with an equal side distribution. The median tumor size was 44 mm (range 2–300mm), and in 45% of cases, tumor size was ≤40 mm. Figure 4 shows the distribution of the clinical tumor size. Tumor thrombus was described in 5.9% (n=256) of cases. The level of the thrombus was 0, I, II, III, and IV in 114, 49, 52, 30, and 11 cases, respectively. At presentation, distant metastasis was reported in 318 (7.3%) cases.

Distribution of clinical tumor size among all cases.
Management
The majority of cases (94.1%) received interventional treatment (Table 1). Table 2 shows modality of treatment and approach. Excisional surgery (radical nephrectomy [RN], partial nephrectomy [PN], tumor enucleation, or nephroureterectomy) was performed in 3921 cases (95.6% of interventions) and ablation in 146 (3.6% of interventions). Open surgery was used in half of the cases followed by laparoscopic (36.7%) and robotic (7.7%) approaches. Of the interventional cases, adrenalectomy was reported in 784 (20.0%) and lymphadenectomy in 472 cases (12.0%). Overall, some type of nephron-sparing surgery (NSS) including enucleation and ablation was performed in 46% of the interventional cases.
Cases on active surveillance, medical treatment, or an unknown management (n=255) are not considered in this table.
Two cases were treated in bench and included as open partial nephrectomy.
NA=Not available.
Pathologic outcomes
Table 3 shows the pathologic outcomes of the cases that received any form of excisional surgery (3921 cases). The total number of extirpated tumors among these cases was 4230, with only one tumor extirpated in the majority of cases (93.5%). The tumors were predominantly malignant (85.7%). From the malignant cases, 95% (n=3193) were RCCs. From all RCCs, the clear cell subtype represented 75.9% (n=2424); papillary type I, 9.2% (n=295); papillary type II, 4.4% (n=140); chromophobe, 7.7% (n=247); and other subtypes or differentiations, 2.7% (n=87).
A case is indicated as malignant if at least one of the extirpated tumors was malignant.
Of RCCs according to 2002 Tumor-Node-Metastasis.
Tx cases with insufficient data.
NA=not available; IQR=interquartile range; RCC=renal-cell carcinoma; TCC=transitional-cell carcinoma; AML=angiomyolipoma.
To assign grade, 61 (62.2%) centers used the Fuhrman 4 grades, 11 (11.2%) the Fuhrman 3 tiers, and 14 (14.3%) both systems. Other nonspecified systems were used by four (4.1%) centers while seven (7.1%) centers used a combination of other systems with Fuhrman 3 or 4 tiers. One center did not report on the grading system used. Overall grade was assessed according to Fuhrman 4 tiers system in 2237 cases (grade 1, 225 [10.1%]; grade 2, 1106 [49.4%]; grade 3, 666 [29.8%]; and grade 4, 240 [10.7%]). In 423 cases, the 3 tiers Fuhrman system was used (grade 1, 89 [21%]; grade 2, 220 [52%]; and grade 3, 114 [26.9%]). Only 124 (3.9%) cases with RCC tumors had positive regional pathologic positive lymph nodes (single or multiple).
Discussion
The most important clinical findings of the CROES Global Renal Mass Study are that half of the renal tumors currently managed in urologic departments are small RM (≤40 mm); more than 60% of the patients present with at least one comorbid condition and manifest basal CKD≥III in around one quarter of the cases. When interventional treatment is considered, the distribution between RN and nephron-sparing techniques is almost even. Two thirds of the RCC are pT1, mostly pT1a, and the rate of pathologic positive lymph nodes is very low.
These data, derived from a prospective clinical registry, offer a “snapshot” on the current patterns of presentation and treatment of renal masses worldwide. These figures should be framed between previous population-based registries and those from centers of excellence.
For a registry or database to be reliable, the missing data should be reported and scrutinized. 14 Because some of the registry variables were not compulsory for reporting (e.g., preoperative analytic determinations), a certain number of NA data were expected in those variables without a specific recommendation issued by national or international guidelines. 15,16 In fact, when the study was launched, recommendations in terms of diagnostic tests were only available for imaging and renal function assessment. 15 As an example, in the very recently American Urological Association issued statements, basic laboratory testing is recommended (blood urea nitrogen/creatinine, urine analysis, and estimated glomerular filtration rate) with level IV evidence while other laboratory evaluations are left to the discretion of the clinician. 17
In the Global Renal Mass Study, the rate of NA or missing data for the primary variables is low except for ethnicity and BMI. Data completeness has been cited as one of the key data quality attributes that determines usability of a registry. 14 A review of a Dutch National Intensive Care Evaluation registry shows that data might be incomplete in 5% to 6% of cases depending on how information was recorded, which is comparable to the current data. 14 This represents the strongest point of our report and reinforces the reliability of our findings.
In the current study, the mean patient age at diagnosis (61.5 years) is lower than previously described and corroborates the decreasing trend reported between 1991 and 2007, from 64.7 years to 62.7 years. 2,18 The lowest and highest interquartiles and the distribution suggest that a considerable percentage of patients presenting with a RM are younger than 50 or older than 75 years of age (19.8% and 16.3%, respectively, data not shown). Consistent with previous reports, two-thirds of the cases were incidentally diagnosed. 18,19
One or more comorbid conditions were reported in two-thirds of the patients, and half of them presented with some degree of hypertension. The high hypertension rate in our population fully reflects the increasing incidence of this worldwide health burden. 19,20 The occurrence of CKD ≥III and CKD II in 22% and 46% of cases, respectively, is higher than described for the population in the age range of our study. 21 It can be only partially explained by the physiologic progressive loss of renal function and likely attributable to the high rate of comorbidity exhibited by our cohort, although the role of tumor size in replacing functional parenchyma cannot be excluded.
Risk factors for RCC were captured in the Global Renal Mass Study. The median BMI was in the range of overweight 13 and the rate of any class obesity higher in our population than the 10% and 14% WHO reported for males and females, respectively. 22 Although our study was not designed to assess causality, cigarette smoking and obesity together with hypertension are well known RCC-associated risk factors. 18,23
In terms of RM clinical size and stage, our study shows that the increase in early stages and decrease in advanced stages previously reported by the Dutch National Histopathology Registry and the National Cancer Data base continues. 1,4,24 The frequency of benign tumors in the Global Renal Mass Study was between the 7% and 33% described among RMs. 25
The above data pose an important paradigm; smaller RMs than in the past are being diagnosed in a population at risk of the development of further renal insufficiency and associated cardiovascular events because of comorbidity. 26 In contrast with previous Surveillance, Epidemiology, and End Results reports but following the increasing trend in NSS showed in the United States, 27 –29 we can affirm that some kind of NSS is being performed in almost half of the cases (46%), demonstrating a sensible advance in the endeavor of NSS. Factors that may drive the type of intervention were not assessed in the current report.
Although the type of surgery (RN vs PN) should prevail over the approach, these preliminary data indicate that at least half of the RNs are still performed by the open approach; when considering the median clinical size in our study, this figure seems excessive. At least for RN, the laparoscopic approach has been proven beneficial over its open counterpart in terms of morbidity, and it is currently recommended when a RN is indicated in the localized stage. 30,31 Rates of adrenalectomy and lymphadenectomy were low, in line with previous reports. 32
Limitations of our study included an uneven rate of inclusion from the different continents, but although the majority of patients came from Europe, the inclusion rate from the Americas allows for future comparison. Because of a variety among the participating centers in terms of hospital volume or in their qualification (academic, reference, or peripheral hospitals), the number of patients included per year and center differs. Although this reflects the wide spectrum of everyday practice, this aspect might influence the data and should be taken into account in present and future analysis. Next, data on surveillance and ablation were reported by a limited number of centers. It should be regarded cautiously when treatment prevalence is considered, but it might truly reflect institutional policies or instrumental availability. Last, conclusions in terms of RCC grade cannot be generalized at this point. While the use of different grading systems reflects variations in practice, an apparent discordance seems to exist in the prevalence of low grades between the centers using 4 or 3 tiers Fuhrman grading. 33 The (low) rate of grade 1 in the subcohort graded according the 3 tiered system is difficult to frame and points out the difficulties encountered in reproducing Fuhrman grading among pathologists. 34
In spite of these limitations, our data provide reliable information on the major decrease in clinical and pathologic size of RMs. It supports the presence of a high rate of comorbidity and of risk factors for RCC in the RM population and confirms the shifting trend from RN to NSS.
Footnotes
Acknowledgment
The Global Renal Mass Study was supported by an unrestricted educational grant from STORZ.
Disclosure Statement
No competing financial interests exist.