
Abstract
Background and Purpose:
Laparoscopic retroperitoneal lymph node dissection (L-RPLND) is an alternative in patients with metastatic nonseminomatous germcell tumors (NSGCT) necessitating resection of residuals postchemotherapy. With the advancement of laparoscopic vascular surgery, prospective management of the great vessels has become feasible and safe. We present our experience with L-RPLND in NSGCT residuals with significant vascular involvement necessitating intracorporeal reconstruction.
Patients and Methods:
We have retrospectively identified 19 NSGCT patients (mean age 27 years) who presented with residuals postchemotherapy. A bilateral L-RPLND was performed in all men. Infiltration of the great vessels was confirmed intraoperatively. Prospective vascular control and temporary clamping was performed in all cases. The vessel wall was reconstructed using vascular surgery techniques. All patients had at least clinical stages of IIA or higher. Follow-up was obtained in all.
Results:
There were no conversions to open surgery. The mean size of the residuals after chemotherapy was 3.87 cm (1.5–9.7 cm). The mean blood loss was 310 mL (50–1000 mL). Mean hospital stay was 6 days (3–9 days). There were no perioperative complications exceeding grade II according to the Clavien-Dindo classification. Distant or in-field recurrence (mean observational period 18 months) did not develop in any patient.
Conclusion:
Laparoscopic RPLND may be considered a safe alternative concept for the management of post-chemotherapy NSGCT residuals involving the great vessels. Bilateral L-RPLND in patients with vascular infiltration is feasible and reproducible when laparoscopic vascular surgery can be reliably handled. All standard principles of open surgery are respected, and initial oncologic results are promising.
Introduction
I
The laparoscopic approach (L-RPLND) has been developed to reduce the operative morbidity of RPLND. A superiority of laparoscopy to laparotomy regarding overall complication rates and morbidity has first been shown by Janetschek and associates. 3 Several centers have shown the feasibility and safety of L-RPLND also for low-volume NSGCT after chemotherapy. Some patients still present with high-volume disease. Of those, a small proportion exhibits tumor thrombi necessitating intraluminal resection and vascular reconstruction. In an earlier study, Beck and colleagues 4 reported a series of 955 patients with residuals after chemotherapy, including 65 patients (6.8%) patients for whom a resection of the vena cava was necessary. Ehrlich and coworkers 5 could show similar results in their series with 78 patients with RPLND after chemotherapy. In five (6.4%) patients, resection and reconstruction of the vena cava was necessary because of extensive retroperitoneal residuals.
The infrarenal vena cava is predominantly involved but the aorta may also be affected. 6 As suggested by Caldarelli and colleagues, 7 tumors involving less than half of the circumference of the vena cava should be handled by primary suture or by the use of a venous patch. In case of lesions involving more than half the venous circumference, resection and respective replacement of the vein is indicated.
The standard approach to excessive retroperitoneal residuals and complete vascular replacement undoubtedly remains laparotomy. The management of NSGCT necessitating partial vascular reconstruction, however, may also be amenable to laparoscopy. The advancement of laparoscopic vascular surgery allows for prospective management of the great vessels and intracorporeal reconstruction while oncologic principles and safety are fully maintained. The technique presented here is based on the use of laparoscopic bulldog or Satinski clamps (Aesculap, Tuttlingen, Germany). 8 The use of laparoscopic bulldog clamps has been introduced in other urologic procedures such as for the control of the dorsal vein complex during radical prostatectomy 9 or for temporary pedicle occlusion during robotic and purely laparoscopic partial nephrectomy as well as in laparoscopic nephroureterectomy. 10
In this retrospective study, we present our experience with L-RPLND in NSGCT residuals with vascular involvement necessitating intracorporeal reconstruction of the great vessels.
Patients and Methods
We have retrospectively identified 19 patients who presented with retroperitoneal residuals after platinum-based chemotherapy for metastatic NSGCT. In-house Institutional Review Board approval had been given (529/2012R) before data analysis. After platinum-based chemotherapy, all men underwent systematic bilateral L-RPLND between 2009 and 2013 as described before. 8 All patients had shown partial involvement of the infrarenal great vessels by NSGCT residuals on preoperative imaging (Fig. 1). Primary inclusion criteria for L-RPLND were tumors involving less than half of the circumference of the infrarenal or suprailiacal great vessels and tumors with a small vascular contact. 7 Residuals involving more than half the vascular circumference or excessive retroperitoneal residuals with need of complete vascular replacement have to be treated by open RPLND. Infiltration of the great vessels and tumor thrombi were ultimately confirmed intraoperatively. All oncologic principles including complete template resection were fully respected. Vascular reconstruction was performed duplicating open surgery.
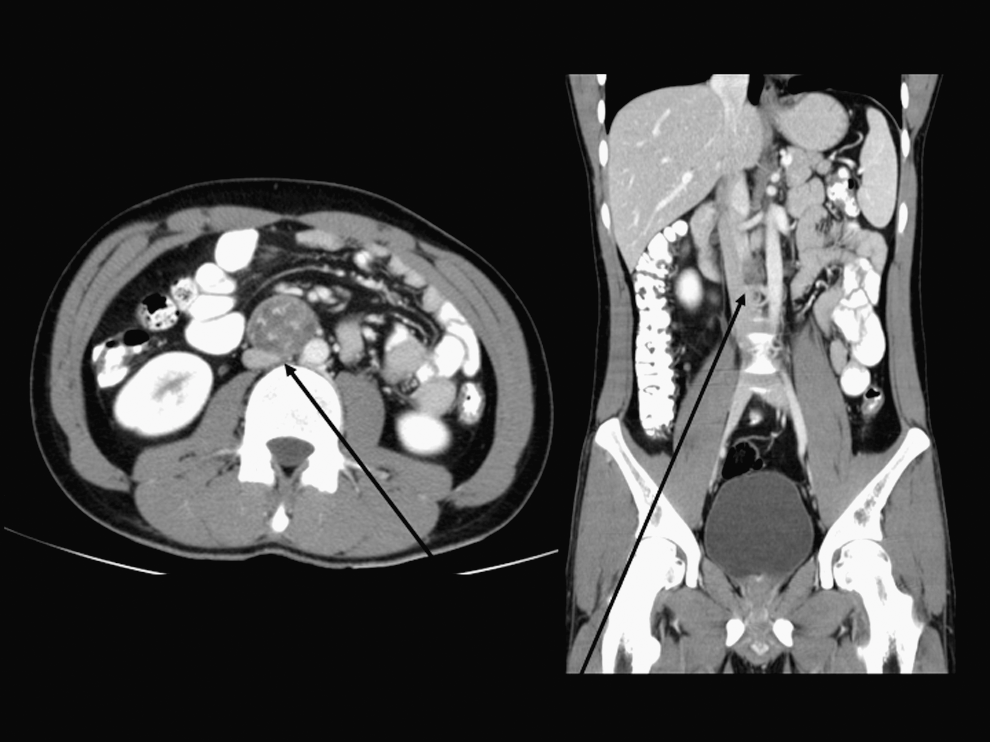
CT scan demonstrating large interaortocaval residual after platinum based chemotherapy. Arrows show site of infiltration and intravascular growth.
All men had a full preoperative work-up including vascular ultrasonography, CT, or MRI as well as assessment of tumor markers (beta-human chorionic gonadotropin, alpha fetoprotein, lactate dehydrogenase). Positive markers after chemotherapy were an exclusion criterion for RPLND, and these men received salvage chemotherapy. Patients with in-field relapse secondary to previous open RPLND were also excluded from the analysis. Patients with extensive vascular involvement requiring complete replacement of the great vessels underwent primary open RPLND. 7
Technique
The featured technique is stepwise and reproducible based on the use of laparoscopic bulldog or Satinski clamps resembling open surgery. 8 –10 L-RPLND was performed as described previously using a 4-trocar midline approach. The dissection includes removal of all residuals and lymphatic tissue within the boundaries described by Weissbach and associates. 11,12 The trocars are placed entirely in the midline with a 10-mm camera port 2 cm above the umbilicus, two 12-mm working trocars approximately 15 cm above and below the camera port, as well as a 5-mm trocar below the xiphoid for liver retraction.
The patient is initially in a left full-flank position in analogy to nephrectomy because the dissection is started on the right. 8,13 The ascending colon is entirely reflected followed by extensive mobilization of the duodenum to expose the great vessels. Because of gravity, a special kind of bowel retractor was mostly not necessary in L-RPLND. In some rare cases an endoscopic bowel retractor was helpful. A vessel sealer (Erbe, BiCision, Tuebingen, Germany) was used in all cases.
Ideally, both the aorta and the vena cava can be fully appreciated at this point. Then the procedure is tailored to the individual tumor location, with most being located either in a precaval or interaortocaval position. First, the lymphatic tissue is slit and the lateral edges of the vena cava are visualized above and below the mass. Then, the vein is fully mobilized posteriorly including a complete transection of all lumbar veins (Hem-o-lok M clips, Weck, Research Triangle Park, NC) allowing the lift off of the vessel entirely from the prevertebral fascia. The gonadal vein is cut to control all potential inflow in the vena cava. Depending on the size of the mass, paracaval and retrocaval node dissection may be continued at this point following the standards of RPLND, including nerve sparing when achievable.
After having complete circumferential access to the vena cava, the mass may be safely approached (Fig. 2). The vein is subsequently cross-clamped above and below the residuals using laparoscopic bulldog clamps (Aesculap, Tuttlingen, Germany) followed by a complete excision including parts of the vessel wall when necessary (Fig. 3). If tangential clamping was deemed sufficient, a laparoscopic Satinski clamp was percutaneously inserted and manipulated extracorporeally. The lumen was then inspected for thrombi or tumor residuals in a bloodless field followed by frozen section analysis of the vessel wall (Fig. 4). The specimens were placed into impermeable bags (Endo Catch, Covidien, Mansfield, MA). In case of a limited excision, the vena cava may be directly repaired using 4/0 Prolene (Ethicon, Johnson and Johnson, Cincinnati, OH) running suture and antegrade flushing in analogy to open surgery (Fig. 5). In case of wider resection critically reducing the vascular diameter, the vessel wall was augmented with an individually tailored pericardial (St. Jude Medical, St. Paul, MN) patch. The patch was placed using 4/0 Prolene in a running fashion.
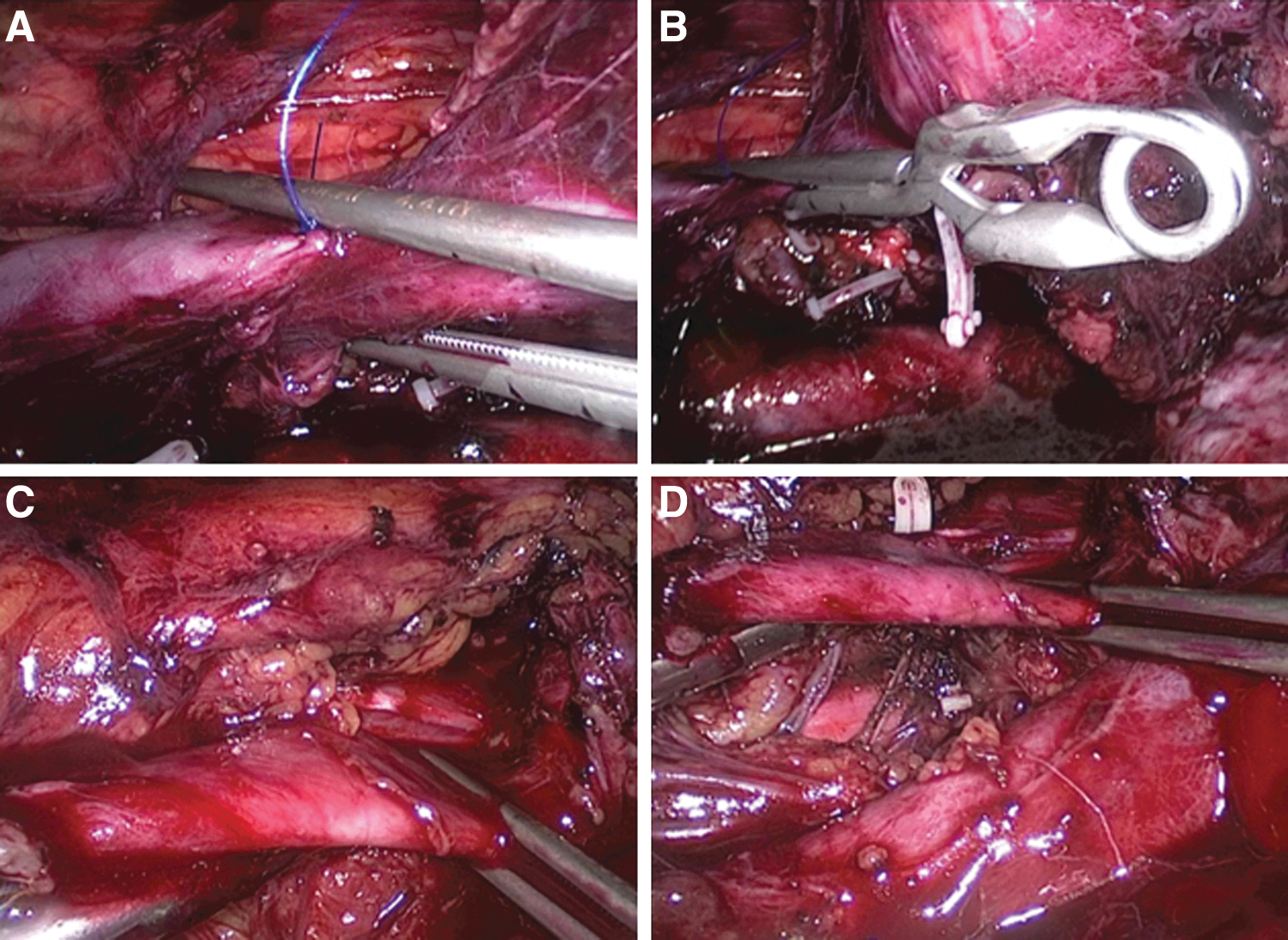
Circumferential dissection and cross clamping of the great vessels.

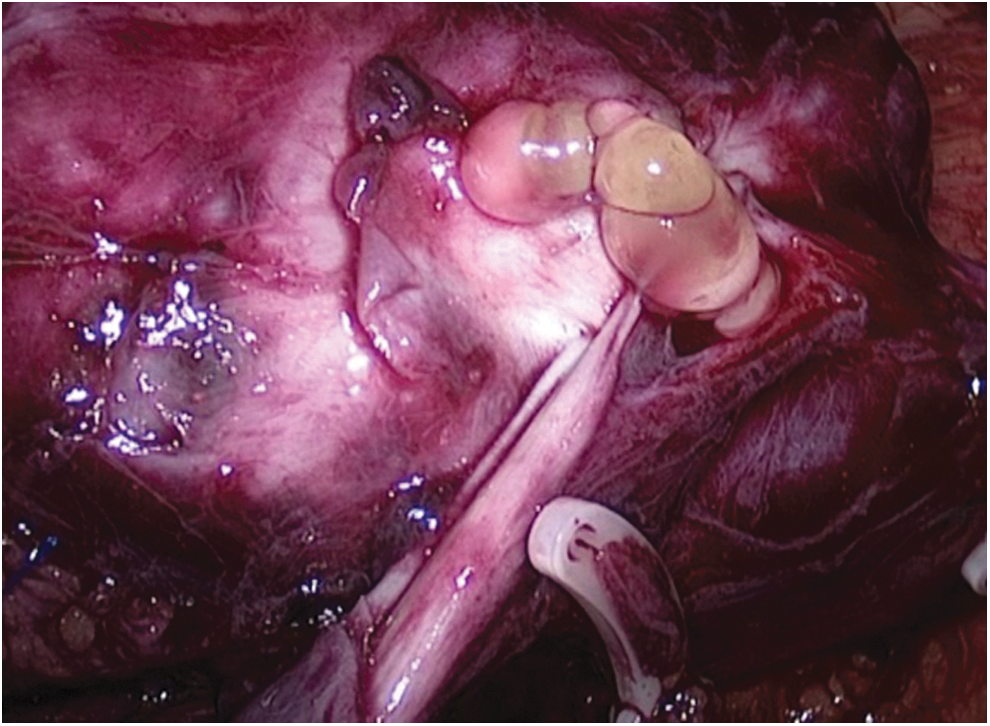
Intraoperative view of the residual mass shown in Figure 1.
Intraluminal tumor thrombus after cavotomy and partial cavectomy in a completely bloodless field.
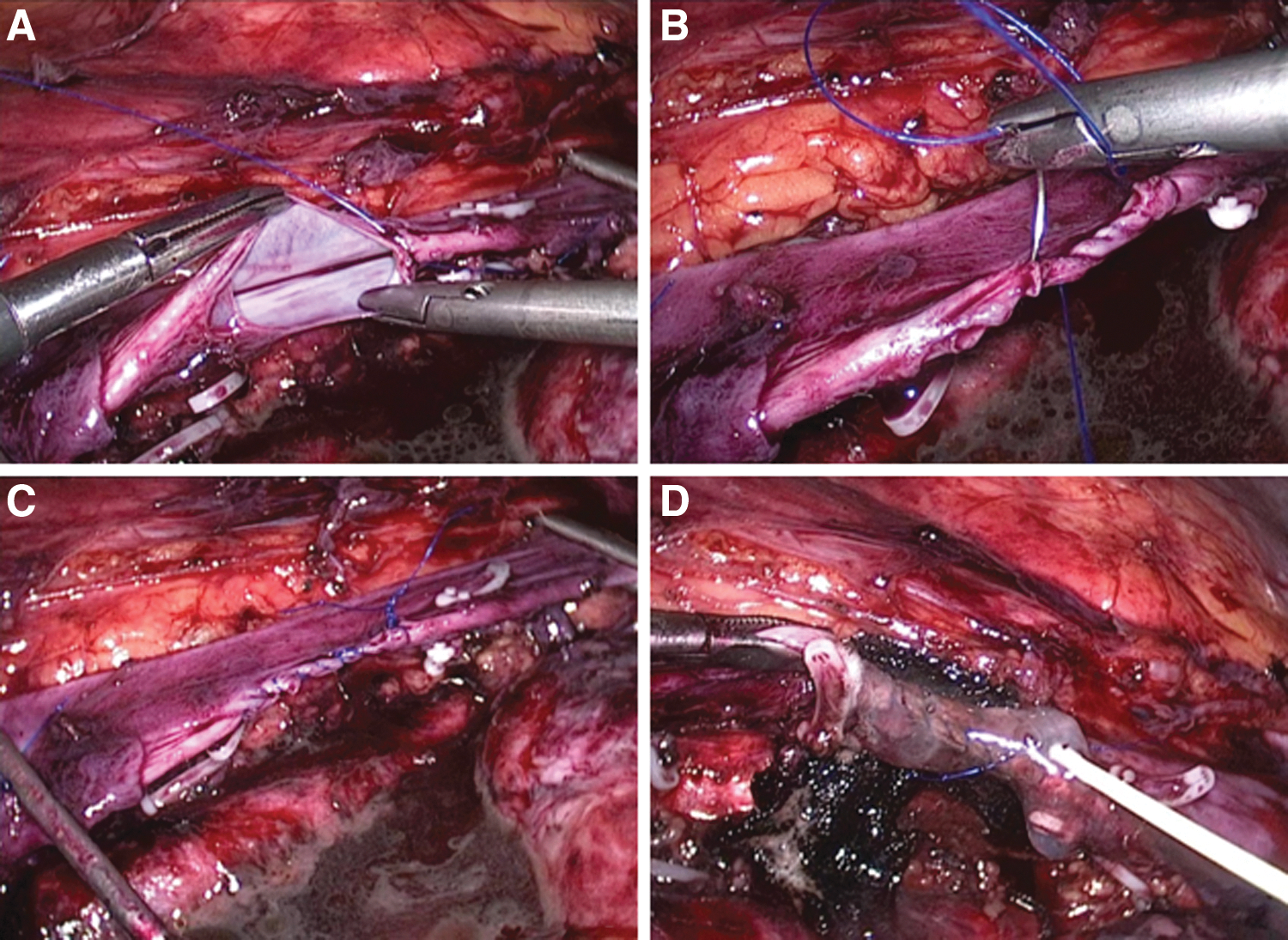
Primary vascular reconstruction of the vena cava using nonabsorbable suture.
After having completed the right-sided template, the port sites were temporarily closed, and the patient was repositioned into a right full-flank position to obtain access to the left template. Ports were reinserted into the same incisions followed by complete left colonic mobilization. The aorta and the left iliac artery were exposed, and a thorough LND was performed between the renal hilum and the ureter's iliac crossing including para-, pre- and retroaortic tissue. In case of preaortic lesions potentially infiltrating the vascular wall, similar principles were applied. Complete circumferential control was achieved and cross-clamping was performed accordingly when needed. As many lumbar arteries as possible were preserved in preaortic lesions. Heparin (5000 IE) was administered intravenously in case of aortic occlusion. Aortic lesions were repaired directly using 4/0 Prolene running sutures while patches were not used. Nonabsorbable clips were placed at all the borders of the lymphadenectomy field to reduce lymphatic leakage. Ports were removed, and the incisions were closed accordingly (Fig. 6). We did not place drains. Postoperatively, all men received a medium chain triglyceride diet for 2 weeks as well as low-molecular weight heparin.

Postoperative result on day 4 after surgery.
Peri- and postoperative data are presented descriptively. Complications are reported using the standardized Clavien-grading. 14 Oncologic outcome is assessed based on sequential follow-up (EAU guidelines). 15
Results
All L-RPLNDs were completed bilaterally without conversion to open surgery. A nerve-sparing (unilateral) procedure was performed in 15, while a radical RPLND was performed in 4. Mean nodal yield was 33.1 (14–65 nodes) per patient. The mean size of the relevant residuals after chemotherapy was 3.87 cm (1.5–9.7 cm). All men had at least three cycles of platinum-based chemotherapy, and the initial clinical stage was at least IIA (Table 1). Mean body mass index was 23.87.
V.=vena; PEB=cisplatin, etoposide, and bleomycin.
The vena cava was affected in 16 while the aorta was compromised in 4 cases (one patient with both vessels affected). The mean estimated blood loss was 310 mL (50–1000 mL). No perioperative blood transfusions were needed. Operative times ranged from 180 to 270 minutes (mean 212 min). The mean hospital stay was 6 days (range 3–9 days). Bulldog clamps were used in 17 whereas partial clamping using a Satinski clamp was done in 2 cases. Intraluminal thrombi were found in three men exclusively in the lumen of the vena cava. Primary vascular repair using a running suture was performed in 13 while a patch was used in 3. Mean cross-clamping time was 26 minutes (12–45 min). The aorta was always repaired primarily using a running Prolene suture. Fibrin glue was applied in all cases. There was no thrombosis or embolism secondary to cross-clamping. There were no perioperative complications exceeding grade II. The immediate postoperative period was uneventful in all.
One man returned to hospital 4 weeks after L-RPLND with lymphocele necessitating laparoscopic fenestration. His further clinical course was uneventful. Another patient presented 1 week after L-RPLND with chylous ascites necessitating repeated puncture and drainage. Ascites disappeared after 4 weeks spontaneously.
Histology results revealed teratoma in 7, necrosis in 10, and vital tumor (<2%) in 2 patients, respectively. The mean nodal yield was 32 lymph nodes (range 20–46 nodes). No patient needed additional consolidating surgery or salvage chemotherapy after L-RPLND. Minimum individual follow-up was 12 months while the overall mean follow-up was 18 months. Distant or in-field recurrence did not develop in any patient. Antegrade ejaculation was preserved in all men who had a nerve-sparing procedure. There were no late postoperative complications recorded after 90 days.
Discussion
L-RPLND has challenged the role of open surgery in the management of metastatic testicular cancer. 16 The overall invasiveness of L-RPLND is significantly lower while equivalent oncologic results are obtained. This is not only true when looking at historical data: Only recently, it has been shown that the complication rate and morbidity of open RPLND postchemotherapy remain considerable (up to 51.9%), 2 even in experienced hands. Several groups including ours have shown that L-RPLND is a reliable and safe technique even after chemotherapy in low-volume NSGCT. 8,16 More complex residuals, however, particularly such with vascular involvement from desmoplastic changes and fibrosis, are still performed openly via median laparotomy. 15 We demonstrate the feasibility and safety of laparoscopy in the management of such complex residuals maintaining both oncologic principles and minimum morbidity for the first time.
Frequently, NSGCT residuals are attached to the vascular wall but may occasionally be found in the lumen of the great vessels. The incidence of intraluminal thrombi in postchemotherapy RPLND can be up to 5.8%. 6 Risk factors include poor prognosis according to International Germ Cell Cancer Collaborative Group risk classification and residuals exceeding 5-cm post chemotherapy. 17 When unexpected, these thrombi may cause serious and life-threatening intraoperative complications. 6
The management of lesions not separable from the great vessels or located inside the lumen necessitates vascular surgery techniques. These include cavotomy and thrombectomy, partial or complete cavectomy, aortic resection, and complete vascular replacement. 6 Caldarelli and coworkers 7 proposed that residuals involving fewer than half the circumference of the vena cava may be handled by primary suture or by using patch techniques. In case of lesions involving more than 50% of the circumference, complete resection is recommended. 7
There is a significant amount of men who present with considerable NSGCT residuals for whom laparoscopy is a safe option. Typically, these are pre- or interaortocaval NSGCT residuals ranging from 3 to 10 cm with a broad contact to the vascular wall. Laparoscopic or robotic management of intraluminal tumor thrombi has been previously demonstrated for T3b renal-cell cancer. 18 Both purely intracorporeal and hand-assisted techniques have been described. 19 There was no difference in oncologic outcome compared with an open series while morbidity was dramatically reduced and patient safety was fully provided.
Incorporation of robotic techniques has aided in the process of intracorporeal vascular reconstruction. Concomitantly, vascular surgeons have implemented minimally invasive aortic replacement into their armamentarium. 20 Again, purely laparoscopic and hybridtechniques are used. Safety and efficacy are comparable to open surgery whereas procedure-related morbidity is diminished. Undoubtedly, these techniques are challenging but teachable and reproducible. Ultimately, it is shown that intracorporeal cross-clamping of the great vessels is safe and reliable and so is vascular reconstruction. Interestingly, the latter is not compromised by an obviously longer suturing time. 21 Laparoscopic magnification greatly helps in improving suturing accuracy applying the standards of traditional vascular surgery.
We have incorporated the aforementioned techniques into our L-RPLND armamentarium allowing for a minimally invasive treatment of more complex, higher volume NSGCT residuals postchemotherapy. Still, there are limitations to the technique, rendering it unsuitable for certain scenarios. In contrast to open surgery, the great vessels should not be encaged by tumor residuals above the renal pedicle or below the iliac bifurcation for L-RPLND. Circumferential control has to be safely obtainable at or below the level of the renal vessels and the bifurcation. Otherwise, a laparoscopic approach cannot be considered sufficiently safe because of a significant risk for massive uncontrollable hemorrhage. The same applies to those who need total replacement of the aorta and vena cava. In these cases, hybrid techniques may be of value. Tumor size itself, however, is not an exclusion criterion for L-RPLND as long as the residuals are below the renal vessels. The largest solitary mass we treated in this series was 9.5×6 cm in a man with growing teratoma syndrome postchemotherapy. Nerve sparing may be offered to some of these men when oncologically safe, applying the same criteria as in open surgery. It has previously been shown that nerve sparing can be reliably provided during L-RPLND. 8,12 As recommended for more advanced residuals, a bilateral full-template approach was used in all while a radical RPLND was performed when deemed oncologically necessary. 1
In this series we have not found major complications (grade II and higher) according to the Clavien-Dindo classification underlining the safety of L-RPLND even in this selected group of patients.
Whenever the wall of the vena cava is extensively affected by residuals, partial replacement using a patch may necessary. Simple resection and occlusion of a previously unobstructed vein will inevitably lead to symptoms including distal thrombosis 22,23 or chronic venous disorders. In our L-RPLND series, a complete ligation of the vena cava was never necessary. Intracorporeal reconstruction was achieved in all men, even in those for whom a patch was necessary to obtain an adequate lumen. Notably, cross-clamping did not cause thrombosis and subsequent embolism. Neither were there problems related to the pneumoperitoneum. This may be because of flushing before ultimate closure.
Thorough preoperative assessment helps identifying those at risk for adjunctive vascular procedures, allowing for proper intraoperative decision-making. 5 When thrombi are suspected, they should be completely excised because of the elevated risk to contain teratoma or viable tumor. 5 In most cases, they are amenable to simple cavotomy and consecutive primary closure. 24 This maneuver is described here for L-RPLND using laparoscopic bulldog-clamps, allowing for a complete laparoscopic excision all residuals. The same principles are applied when a patch is needed for adequate repair. Complete removal and prosthetic repair may be feasible using the same techniques but has not been done in this series. Therefore, open surgery or hybrid techniques are necessary to handle these cases.
Laparoscopic vascular surgery techniques can be safely used to control and handle the great vessels during L-RPLND. This combines oncologic principles and the advantage the minimally invasive approach, including reduced blood loss, less postoperative pain, and shorter hospital stay. This technique allows also for approaching complex retroperitoneal residuals adhering to the vena cava and the aorta replicating the general principles of open surgery. Moreover, in case of unexpected complex bleeding during standard L-RPLND, the aforementioned techniques are easily applicable on both the aorta and the vena cava to avoid blood loss and conversion. There are also several limitations, including the retrospective nature, the highly selected testis cancer subpopulation, and the single-arm design.
Conclusions
Laparoscopic RPLND may be considered a safe alternative for the management of complex postchemotherapy NSGCT residuals involving the great vessels. Bilateral L-RPLND in patients with vascular infiltration is feasible and reproducible when laparoscopic vascular surgery can be reliably handled. Future robotic technology may facilitate vascular reconstruction, leading to a wider acceptance of minimally invasive surgery in advanced NSGCT.
Footnotes
Disclosure Statement
No competing financial interests exist.