
Abstract
Purpose:
Examination of the pyelocaliceal system using a flexible ureteroscope necessitates accurate orientation of the tip of the instrument. This study assessed the use of a novel real-time ureteroscopic navigation system in a pyelocaliceal phantom.
Materials and Methods:
The navigation system used a magnetic tracking device to determine the position of the ureteroscope in a pyelocaliceal phantom and displayed the position of the endoscope on a three-dimensional image that could be rotated. Twenty-eight urologists were divided into group A and group B (seven novice surgeons and seven experienced surgeons in each group). All participants were asked to examine the phantom and identify the positions of three designated calices, without the navigation system (Task 1) and with the navigation system (Task 2). In group A, participants performed Task 1 followed by Task 2. In group B, participants performed Task 2 followed by Task 1. The accuracy rate (AR) of identifying the calices, migration length (ML) of the tip of the ureteroscope, and time (T) taken to complete the task were recorded. The results were compared between Task 1 and Task 2, and between novice and experienced surgeons.
Results:
The AR for Task 2 was 100% in both group A and group B. The AR was significantly lower in Task 1 than in Task 2 for both novice and experienced surgeons in both groups (group A: novice P=0.016, experienced P=0.034; group B: novice P=0.015, experienced P=0.015; Wilcoxon test). In Group A, T was significantly longer in Task 1 than in Task 2 for experienced surgeons. There were no significant differences in ML or T between novice and experienced surgeons.
Conclusions:
Our novel ureteroscopic navigation system improved the accuracy of ureteroscopic maneuvers. Further development of this system for use in clinical ureteroscopic procedures is planned.
Introduction
W
Controlling a flexible ureteroscope necessitates a certain level of expertise. Novice operators may lose their orientation during flexible ureteroscopy in patients with complicated pyelocaliceal shapes or poor visibility because of macrohematuria and may miss stones and tumors if they do not observe all the renal papillae. Operators generally use fluoroscopic guidance to regain their spatial orientation, but because fluoroscopy provides only two-dimensional images, it is difficult to accurately determine the precise position of the tip of the ureteroscope using this method. A navigation system that helps surgeons to confirm the position of the ureteroscope in the pyelocaliceal system using a three-dimensional (3D) image that can be rotated may increase the accuracy of procedures. To our knowledge, no previous studies have assessed the accuracy of ureteroscopic maneuvers using such a navigation system. We therefore developed an experimental model of a novel ureteroscopic navigation system that used a magnetic tracking device and evaluated the system by analyzing the accuracy of ureteroscopic navigation in a 3D pyelocaliceal system model.
Materials and Methods
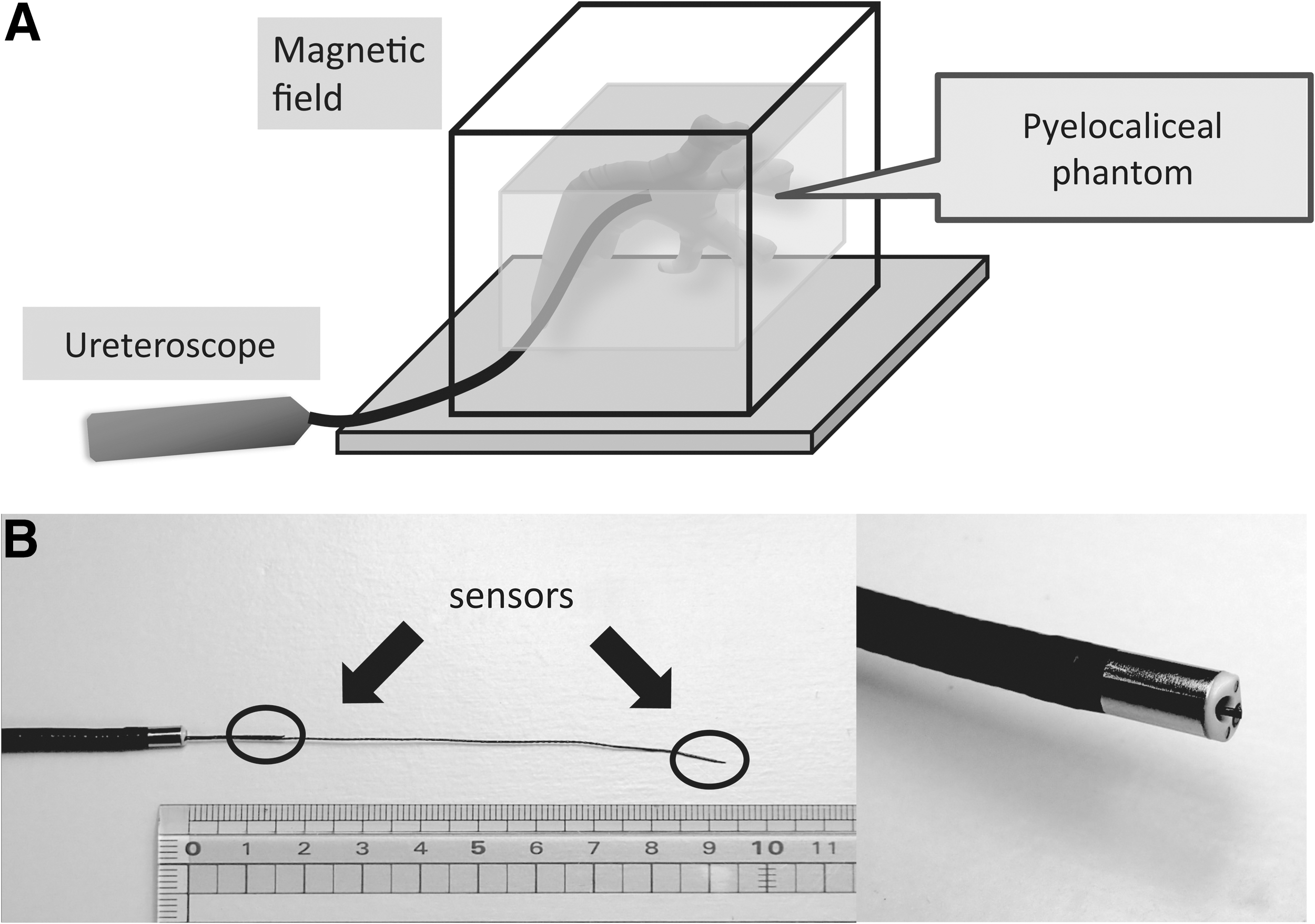
Experimental model of the ureteroscopic navigation system (Fig. 1)
A 3D image of a pyelocaliceal system was created from Digital Imaging and Communications in Medicine CT data (slice thickness, 1 mm) obtained from a patient with a normally structured pyelocaliceal system using OsiriX®. 4 A pyelocaliceal phantom was created using the modified 3D image of the pyelocaliceal system. The phantom was made from polyvinyl alcohol (JMC Corp., Yokohama, Japan) with an outer cuboid shape and an inner cavity for endoscopy. Fiducial markers were attached to four corners of the cuboid phantom.
(
A magnetic field measurement device (3D-Guidance medSAFE; Ascension Technology Corp., VT) was used to track the positions of two sensors on the ureteroscope. This magnetic tracking device provides a magnetic field with a working volume of 400×400×400 mm at a height of 10 cm from the generator. The field generator is connected to a device control unit, which interfaces with a laptop computer. The pyelocaliceal phantom was placed in the magnetic field. A cord with sensors was passed through the channel of the ureteroscope (URF Type-V; Olympus, Tokyo, Japan) to track the position of the ureteroscope in the magnetic field.
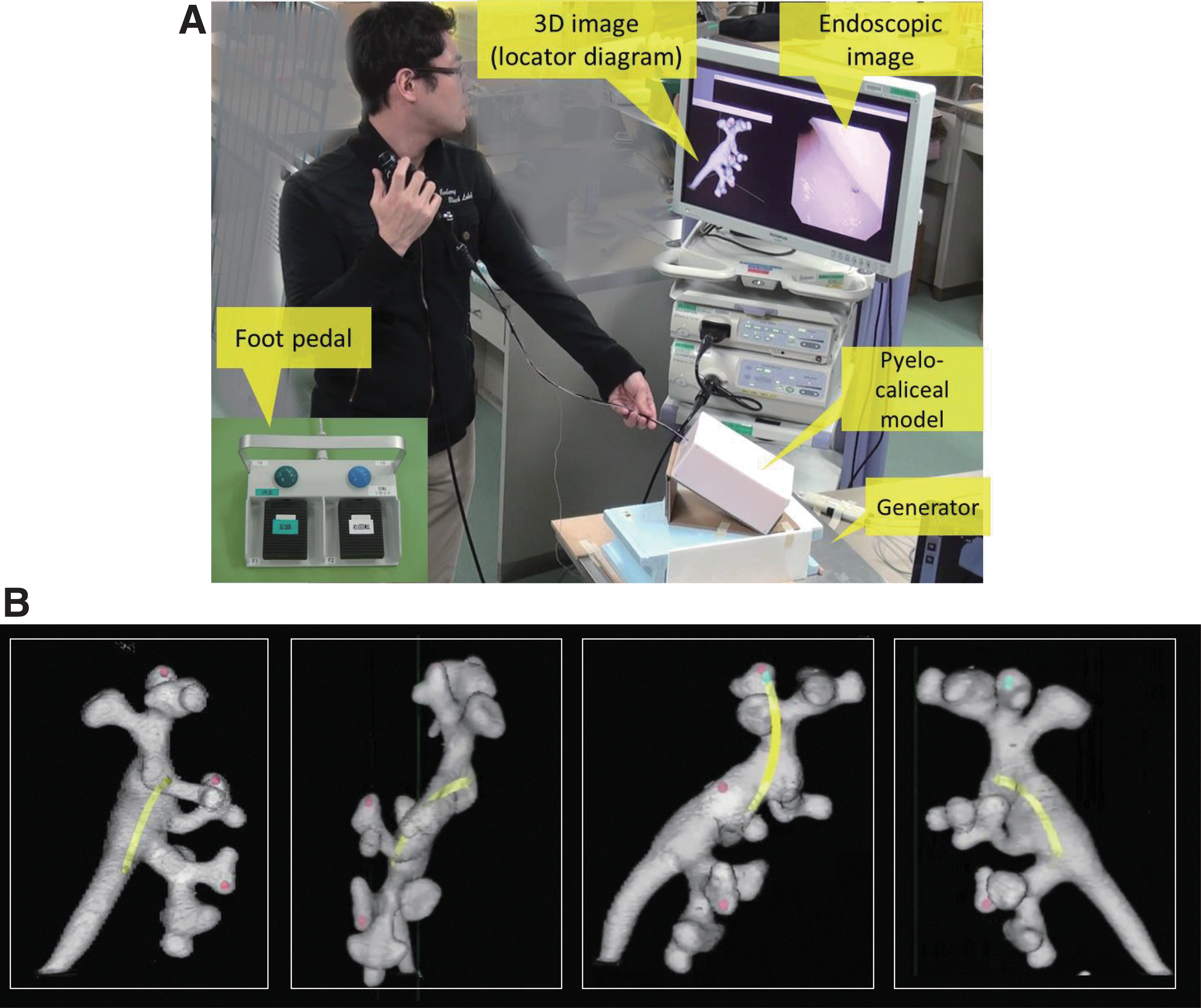
Display of the navigation image (Fig. 2)
The four corners of the phantom with fiducial markers were adjusted to align the position of the pyelocaliceal phantom with the 3D image. After calibration and image registration, the position of the tip of the ureteroscopic was shown on the 3D image of the pyelocaliceal system. This 3D navigation image and the endoscopic image were displayed on a single screen. The tracked positions of the tip of the ureteroscope and a point 8 cm from the tip were displayed in real time with yellow dots on the navigation image, and the two dots were connected by a yellow line that changed shape according to the movements of the ureteroscope. Using a foot pedal with two buttons, the operator could rotate the 3D navigation image to view the depth and current position of the tip of the ureteroscope, and could mark the current position of the tip with a blue dot.
(
Participants and tasks
Twenty-eight urologists were recruited and were divided into two groups. Group A included seven novice surgeons (all male, aged 26–38 years) who had performed 0–5 ureteroscopic procedures each (mean, 2.8 procedures) and seven experienced surgeons (all male, aged 30–45 years) who had performed 40–100 ureteroscopic procedures each (mean, 57 procedures). Group B included seven novice surgeons (all male, aged 25–39 years) who had performed 0–5 ureteroscopic procedures each (mean, 2.1 procedures) and seven experienced surgeons (5 male and 2 female, aged 32–50 years) who had performed 30–80 ureteroscopic procedures each (mean, 51 procedures). To evaluate the ease of use and accuracy of the navigation system, the participants were asked to examine the inside of the phantom without using fluoroscopy. They were asked to identify three designated calices, marked with red circles in the anterosuperior, anteromiddle, and anteroinferior parts of the pyelocaliceal system on the 3D image.
In Task 1, the 3D image on the screen could not be rotated, and the current position of the tip of the ureteroscope was not displayed on the 3D image. The participants were asked to navigate the phantom using only the endoscopic view and to use the foot pedal to indicate when they thought the tip of the ureteroscope corresponded to the locations of the three designated calices marked with red circles. The recorded positions were not displayed on the 3D image.
In Task 2, the 3D image on the screen showed the current position of the tip of the ureteroscope in the pyelocaliceal phantom. The 3D image could be rotated to confirm the shape of the renal papillae and the current position of the tip of the ureteroscope. When the current location of the tip was recorded using the foot pedal, a blue dot appeared on the 3D navigation image.
Participants in group A performed Task 1 (without the navigation system) followed by Task 2 (with the navigation system). To address the possible learning curve effect in participants who performed Task 1 before Task 2, participants in group B performed Task 2 (with the navigation system) followed by Task 1 (without the navigation system). Participants in both groups were given 2 minutes of practice time to examine the inside of the phantom before starting their first task. The participants were asked to complete the tasks as accurately as possible, but were not informed that the time taken was being assessed.
Evaluation of ureteroscopic maneuvers
The accuracy rate (AR) of identifying the marked calices, migration length (ML) of the tip of the ureteroscope, and time (T) taken to complete the task were recorded for Tasks 1 and 2. The AR was calculated as follows:
For measurement of ML and T, the beginning of the task was defined as the time the ureteroscope was inserted into the pyelocaliceal phantom, and the end of the task was defined as the time the ureteroscope was removed from the phantom. The ML was calculated as follows:
Statistical analysis
Continuous variables are expressed as mean (range). Data were compared between Task 1 and Task 2, and between novice surgeons and experienced surgeons, using the Mann-Whitney U test or Wilcoxon test. Statistical analyses were performed using Microsoft Excel for Windows. A P value of <0.05 was considered statistically significant.
Results
Accuracy rate (Table 1)
In Task 2 (with the navigation system), all participants in both groups correctly identified all three designated calices, resulting in an AR of 100% for both novice and experienced surgeons. The AR was significantly lower in Task 1 (without the navigation system) than in Task 2 for both novice and experienced surgeons in both groups (group A: novice P=0.016, experienced P=0.034; group B: novice P=0.015, experienced P=0.015; Wilcoxon test). Furthermore, the AR in Task 1 was significantly lower for novice surgeons than for experienced surgeons in both groups (group A: P=0.009; group B: P=0.01; Mann-Whitney U test).
ML=migration length; T=time; AR=accuracy rate; n.s.=not significant.
Migration length (Table 1)
The ML was not significantly different between Task 1 and Task 2 for novice or experienced surgeons in either group (group A: novice P=0.612, experienced P=0.128; group B: novice P=0.398, experienced P=0.063; Wilcoxon test). The ML was also not significantly different between novice and experienced surgeons for Task 1 or Task 2 in either group (group A: Task 1 P=0.338, Task 2 P=0.277; group B: Task 1 P=0.848, Task 2 P=0.338; Mann-Whitney U test).
Time (Table 1)
T was not significantly different between Task 1 and Task 2 for novice surgeons in either group (group A: P=0.091; group B: P=0.128; Wilcoxon test). T was significantly longer in Task 2 than in Task 1, however, for experienced surgeons in both groups (group A: P=0.028; group B: P=0.028; Wilcoxon test). T was not significantly different between novice and experienced surgeons for Task 1 or Task 2 in either group (group A: Task 1 P=0.406, Task 2 P=0.180; group B: Task 1 P=0.848, Task 2 P=0.848; Mann-Whitney U test).
Discussion
Recently developed augmented reality navigation systems use images from specific patients to obtain real-time intraoperative images that help surgeons to increase the precision of laparoscopic and other procedures. 5 –7 Navigation systems for flexible ureteroscopic surgery have not been reported, however. Our novel ureteroscopic navigation system used magnetic tracking. Development of a similar navigation system using magnetic tracking has recently been described for flexible neuroendoscopy, 8 but use of such a system in clinical endoscopic procedures has not yet been reported. Ureteroscopic procedures are complex, and considerable experience is necessary to acquire the fundamental skills needed. 9
Pyelocaliceal phantoms are commonly used for training and assessment of ureteroscopic skills using inanimate bench models (Scope Trainer; Medskills Ltd., Edinburgh, UK and Uro-Scopic Trainer; Limbs and Things, Bristol, UK). Studies using these bench models found that urologists highly experienced in flexible ureteroscopy clearly had better skills than novice surgeons. 10 –12 Such models have become an important training tool to help novice surgeons improve their skills, but the internal shapes of the models are relatively simple. In clinical practice, surgeons have a range of experience and skills, and the anatomic variation among patients increases the difficulty of procedures. A ureteroscopic navigation system that is relatively easy for surgeons at all levels of expertise to use may therefore help to enhance accuracy and safety of procedures.
In this study, ureteroscopic maneuvers using our navigation system were evaluated by measuring AR, ML, and T. The ML was not significantly different between Task 1 and Task 2 for novice or experienced surgeons in group A or group B. T was longer in Task 2 than in Task 1 for both novice and experienced surgeons, but this difference was significant only in experienced surgeons. Because Task 1 was performed without feedback from the 3D navigation image, the participants tended to finish it early after identifying the wrong calices, without being aware of their mistakes. When using the real-time navigation system images, most participants confirmed the position of the ureteroscope many times, resulting in a longer time to complete Task 2. Experience with use of the system is expected to result in reduced T and ML values as the operator gains confidence and reduces unnecessary maneuvers.
The AR was significantly lower in Task 1 than in Task 2 for novice and experienced surgeons in group A and group B. Even experienced surgeons were not able to accurately identify all the marked calices without the navigation system in Task 1. In Task 2, however, both novice and experienced surgeons were able to identify the marked calices with an AR of 100%. These results indicate that it is not easy to accurately identify the current position of the tip of the ureteroscope using only endoscopic images, even for experienced surgeons, and that use of our navigation system increased accuracy for both novice and experienced surgeons. Although no formal evaluation of the user experience was conducted, all participants indicated that they considered the system to be useful for navigating the pyelocaliceal system relative to conventional ureteroscopy with or without fluoroscopy.
Radiation exposure should ideally be reduced as much as possible to prevent harmful effects to both patients and urologists. 13 Use of our system necessitates that the patient undergo preoperative contrast-enhanced CT to provide the 3D image of the pyelocaliceal system. Previously acquired CT images can be used for this, without the need for additional imaging at the time of ureteroscopy. Low-radiation-dose CT is also sufficient to provide the 3D image, which would help to reduce the radiation exposure of patients.
Use of our system may reduce the need for fluoroscopy during ureteroscopic procedures for confirmation of the position of the ureteroscope, although fluoroscopy would still be needed for placement of guidewires and stents. This is expected to result in reduced overall radiation exposure, especially when procedures are performed by relatively inexperienced surgeons who may need relatively long fluoroscopy times. Our navigation system shows the real-time position of the ureteroscope more clearly than on fluoroscopic images. The recording function can also mark the current position of the tip of the ureteroscope on the 3D pyelocaliceal image to record the location of pathology for future review, or to show which areas have already been visualized.
Our novel navigation system is still under development. Clinical use would require development of a new flexible ureteroscope with a built-in sensor at the tip. Alignment of the position of the image also still needs to be refined. The optimal placement positions for the four markers on the body need to be determined, and technical challenges related to intraoperative deformation and changes in position with breathing need to be overcome. We hope that our ongoing development of the system and future testing in live animal models will overcome these difficulties. We believe that our system has the potential to help surgeons with a wide range of experience to ensure that they observe all the renal papillae, thereby increasing the detection rate of upper urinary tract stones or tumors, as well as increasing the accuracy of surgical procedures by showing surgeons the real-time position of the tip of the ureteroscope on the 3D navigation image.
Conclusions
Use of our novel ureteroscopic navigation system improved the accuracy of ureteroscopic maneuvers in both novice and experienced surgeons, without using fluoroscopy. Further development of this system for use in clinical ureteroscopic procedures is planned.
Footnotes
Acknowledgment
This work was supported by a Grant-in-Aid from the Japan Society for the Promotion of Science (JSPS), KAKENHI (C) No. 25462530.
Disclosure Statement
No competing financial interests exist.