
Abstract
Background:
With the increasing use of robot-assisted techniques for urologic and gynecologic surgery in patients with severe comorbidities, the risk of a critical incidence during surgery increases. Due to limited access to the patient the start of effective measures to treat a life-threatening emergency could be delayed. Therefore, we tested the management of an acute emergency in an operating room setting with a full-size simulator in six complete teams.
Methods:
A full-size simulator (ISTAN, Meti, CA), modified to hold five trocars, was placed in a regular operating room and connected to a robotic system. Six teams (each with three nurses, one anesthesiologist, two urologists or gynecologists) were introduced to the scenario. Subsequently, myocardial fibrillation occurred. Time to first chest compression, removal of the robot, first defibrillation, and stabilization of circulation were obtained. After 7 weeks the simulation was repeated.
Results:
The time to the start of chest compressions, removal of the robotic system, and first defibrillation were significantly improved at the second simulation. Time for restoration of stable circulation was improved from 417±125 seconds to 224±37 seconds (P=0.0054). Unexpected delays occurred during the first simulation because trocars had been removed from the patient but not from the robot, thus preventing the robot to be moved.
Conclusion:
Following proper training, resuscitation can be started within seconds. A repetition of the simulation significantly improved time for all steps of resuscitation. An emergency simulation of a multidisciplinary team in a real operating room setting can be strongly recommended.
Introduction
S
Life-threatening emergencies with the need for resuscitation in the operating room are rare and differ to some degree from resuscitations in other locations. 5 –7 The patient's history is known and the crisis develops with an anticipated pathophysiology. 5,7,8 Moreover, a critical incident in an operating room has the advantage of very early detection and abundant resources in personnel and equipment to manage the situation. Because of the very low incidence of such events, however, there is a lack of experience in managing these crises. 7 To improve crisis management, simulator training scenarios have been developed. 5,6
To evaluate the management of an acute emergency during robot-assisted surgery, including resuscitation, we enrolled six complete operating teams in an operating room setting with a full-size simulator modified for robot-assisted surgery. All teams regularly work together with a robotic system in this setting.
Materials and Methods
Recruitment
After approval by the local ethics committee (Chamber of Physicians of Nordrhein, Düsseldorf, Germany, Registration Number 114/2011) six teams, each formed by three nurses, one anesthesiologist, and two urologists or gynecologists, participated in this study. Each member of the team had at least 3 months experience in robot-assisted surgery. Each participant provided informed written consent and was ensured that details of the scenario and personal performance by the participants would not be disseminated.
Material and protocol
A full-size simulator (ISTAN, Meti, CA) was modified to hold five trocars. An additional abdominal wall was taped and stuffed on top of the abdominal wall of the simulator without disturbing the integrity of the original abdomen and the electronic equipment inside. The simulator was brought into an operating room, which is used every day for robot-assisted surgery. The table was tilted 45° in a steep Trendelenburg position as done for radical prostatectomies. All the necessary equipment for radical prostatectomies or hysterectomies was prepared, and the simulator was covered with sterile drapes similar to a patient for one of the two procedures.
The simulator was intubated and mechanically ventilated. Intraoperative monitoring provided a three-lead electrocardiogram (ECG), invasive arterial blood pressure tracing, and oxygen saturation. The simulator was programmed with a fluid deficit of 1000 mL and a reduced coronary reserve with mild aortic stenosis. As a standard for these procedures in American Society of Anesthesiologists (ASA) 3 classified patients, the simulator was equipped with an invasive arterial line, a three-lumen central venous catheter, two peripheral venous lines, and a gastrointestinal tube.
The first team was called into the room and introduced to the scenario. The two urologists or gynecologists (attending and resident) and the two operating nurses (one scrubbed at the table and one assisting) were informed that all trocars had been placed and CO2 insufflation had begun without difficulties and that the patient was ready to be docked to the robotic system.
The anesthesiologist and the anesthesia nurse were introduced to the patient and the ongoing anesthesia. The patient was described as an ASA 3 classified patient with mild aortic stenosis grade II and coronary artery disease in preoperative stable condition. The anesthesiologist, who was taking over the anesthesia, was informed that during the initial anesthesia mild arrhythmia was observed. All further details were documented on a mock anesthesia record sheet. All participants were informed that they could use all usually available resources.
Next, the patient was docked to the robotic system (da Vinci S2, Intuitive Surgical Inc., Sunnyvale, CA) and the urologist or gynecologist sat down at the console. During this time the number of ventricular extra beats of the patient increased. After 10 minutes the patient developed ventricular fibrillation. The time to call for help, undock and remove the robot, start chest compressions, initiate defibrillation, and the return of spontaneous circulation (ROSC) were recorded. All recorded time spans refer to the start of fibrillation on the monitor. The entire simulation was recorded with two cameras.
All six teams had their simulations on the same day and gathered in the afternoon for a debriefing. Subsequently, a flow sheet for the management of emergencies during robot-assisted surgery was created and posted on the walls of operating rooms used for robot-assisted surgery. After 7weeks the simulation was repeated with all six teams at the same day in the same operating room.
Data Analysis
Data are presented as mean±standard deviation (SD). Sample size calculation was based on the primary hypothesis that there is no significant difference in the time to the start of chest compressions. The hypothesis was tested using Student t-test. Differences were considered significant for P<0.05.
Secondary outcome measures were time to (1) call for help, (2) remove the robot, (3) first defibrillation, and (4) ROSC. The recorded time to remove the robot was compared to presimulation estimates from the participants.
Results
Demographics of the teams
There were four urologic teams consisting of one attending urologist, one urologic resident, one anesthesia resident, one anesthesia nurse, and two operating room nurses. Two additional teams were equally staffed with two gynecologists instead of the urologists. Overall, 36 people participated. In Germany anesthesia nurses assist the anesthetist and do not work independently.
The members of the team had a mean experience in robot-assisted surgery of 16 months (range, 3–34 months). The simulation was repeated with the same individuals after 7 weeks.
Primary outcome measure: Time to start chest compressions
The primary hypothesis was that there was no change in the time span from ventricular fibrillation to the start of chest compressions with the repetition of the simulation. The time to the start of chest compressions during the first simulation was 71±30 seconds (mean±SD) and the time improved to 25±9 seconds at the second simulation (P=0.0080; Fig. 1).

Box plots of the time for resuscitation measures. Open boxes indicate the times at the first simulation while grey boxes represent the results of the second simulation. Time for the first chest compressions (left), removal of the robot (middle left), first defibrillation (middle right), and return of spontaneous circulation (ROSC, right) improved significantly at the second simulation.
Secondary outcome measures: Time spans for additional resuscitation measures
The time to call for help, disconnect the robotic system, perform defibrillation, and ROSC also improved during the second simulation (Fig. 1). The first time span for time to call for help was biased by one outlier (for one team the time to call for help took 4.9 times longer than the mean time of all the other teams). Excluding this outlier would change the P values for comparing the time to call for help between the first and second simulation from 0.0860 to 0.0088.
Debriefing
A debriefing session in the afternoon after the first simulation revealed the difficulties with the robotic system and led to a flow diagram that was made available to the participants and hung up on the wall of operating rooms used for robotic surgery (Fig. 2).
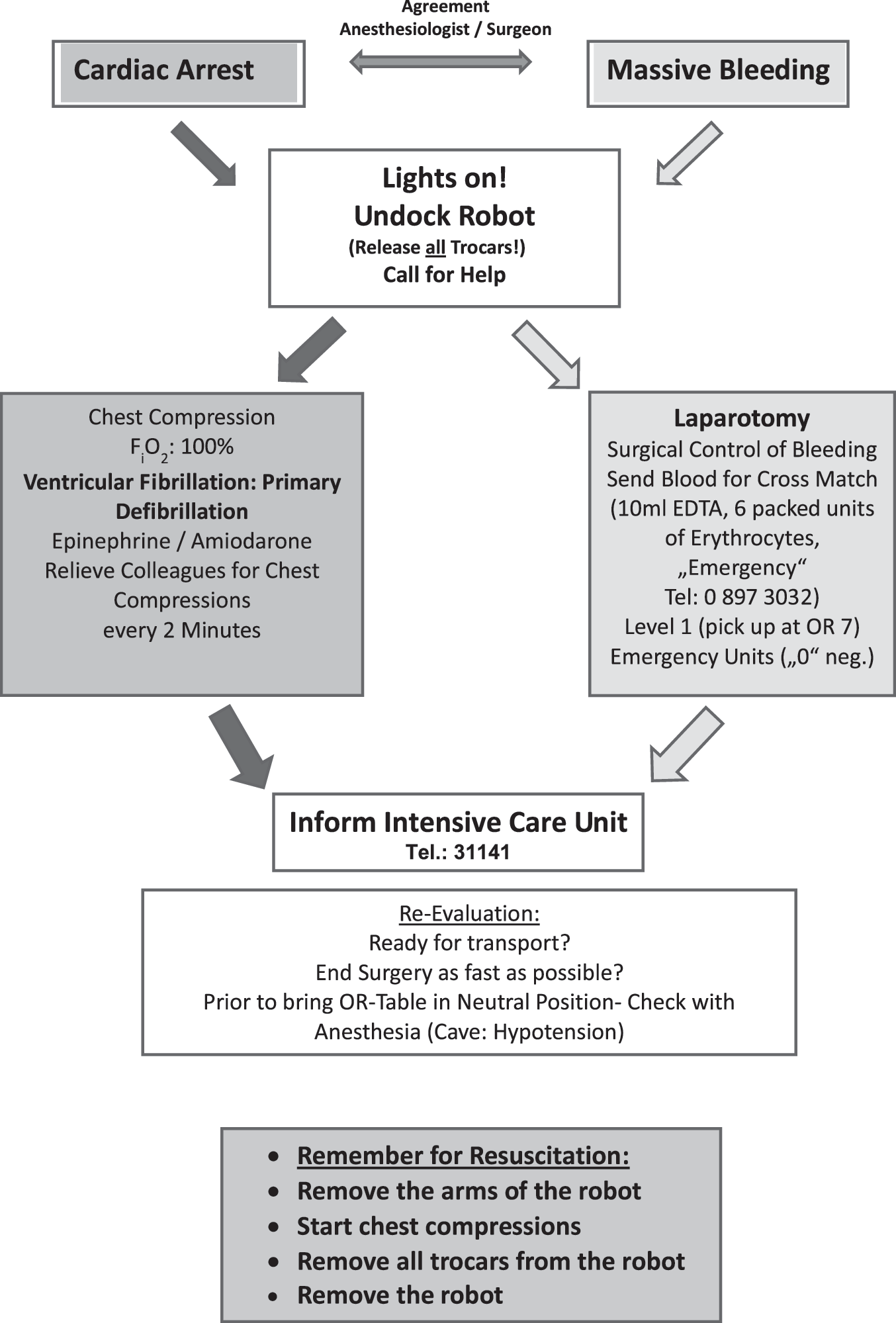
Flow diagram for the management of life-threatening emergencies during robot-assisted surgery. The diagram is the result of the debriefing after the first simulation and represents an interdisciplinary agreement between all departments involved. EDTA=ethylenediaminetetraacetic acid.
Discussion
A robotic system for abdominal surgery can significantly reduce access to the patient in case of a life-threatening emergency (Fig. 3). The complete removal of the system took an unexpectedly long time in the initial simulation. Withdrawing the arms of the robot with the main robot still in place, however, allows for the start of chest compressions within seconds. A repetition of the simulation significantly improved all times for resuscitation measures.

Picture of the scenario in the operating room during the emergency simulation before cardiac arrest. The simulator is completely covered and tilted in a 45° head-down position. Direct access to the chest of the simulator is blocked by the arms of the robotic system.
Robot-assisted prostatectomies and hysterectomies have found widespread popularity and acceptance over the last decade. Even in elderly patients with significant comorbidities robot-assisted surgery has proved to be an effective and safe procedure, and it is expected that more and more elderly patients will undergo such surgery. 1 –3 In our institution, the number of robot-assisted prostatectomies increased from 106 cases in 2009 to 357 cases in 2012. In 2012 approximately 30% of the patients were classified with an ASA classification of 3.
Because of a low incidence of life-threatening emergencies in daily clinical work, it is difficult to expose residents to emergency scenarios and thus difficult to train residents in crisis management. 9 Many residency programs train their residents and often their whole staff, therefore, in the management of specific emergencies in a simulation center. 10 To create a realistic environment, additional staff (surgeons, nurses, etc.) are typically played by actors or volunteers. 9 –11 The participants act within their specialty, focused on specialty-specific problems. In the particular situation of robot-assisted surgery, besides knowledge and skills needed to treat a life-threatening emergency, additional knowledge is required regarding the handling of the robotic system.
We decided to perform our interdisciplinary simulation with anesthesiologists, urologists, gynecologists, and operating room nurses. This scenario adds a challenge of arranging a “crisis team” within different departments with different backgrounds in training and routines to handle emergency situations. Performing emergency simulations with participants from different departments creates the opportunity to exchange specialty-specific knowledge and experience across departmental boundaries. 12,13
In our scenario, the undocking of the robotic system, which would have been just a verbal order in a simulation center with mock surgeons, turned out to be unexpectedly difficult. In the first simulation the arms of the robot were pulled back. This yielded enough room to start chest compressions, albeit still hampered by the robot. In this stressful situation five of the six teams were not aware that the robot could not be completely removed as long as one of the robot arms held a trocar. The complete removal of the robot took much longer than in the second simulation.
In addition, the use of the defibrillator in the operating room turned out to be more difficult than expected. Before the second simulation, both problems had been discussed at the debriefing session.
As a result of this session a flow diagram was created and posted in every operating room suited for robot-assisted surgery. As Babcock already postulated in 1924, specific orders on how to handle an emergency should be posted on the wall. 14 The use of cognitive aids for crisis management have been shown to improve the performance and prevent the omission of additional critical measures 6,15 –17 Hence we can assume that all of the staff who were familiar with handling the robotic system had read that all trocars need to be released before the robot was removed, but this information could not be recalled under the stressful situation of a life-threatening emergency. Limitations to recall memories under stress have been well described before. 18
Our study was limited to two simulation sessions. As Yee and colleagues have demonstrated that specific nontechnical skills significantly improve only from the first to the second simulation but not from the second to third, we abandoned the idea to perform a third session. 11
The study was limited to the situation in which the robotic system could be undocked without major concerns about bleeding or abdominal sequelae of the ongoing procedure. If the emergency had taken place later during the surgery, the whole team decided that after stabilization of circulation the urologist or gynecologist should return to laparoscopy and check whether the patient would require surgical intervention (e.g., active bleeding) before the transfer to the intensive care unit. For the purpose of fast access to the surgical site, it might have been advantageous to leave one of the lateral trocars in place; however, the team decided against that solution due to concerns that a remaining trocar might cause uncontrolled harm during chest compressions and the manipulation of the patient.
Conclusions
An emergency simulation with a full-size simulator using a multidisciplinary approach revealed specific difficulties that were solved following the first simulation. Most importantly, we found that resuscitation in patients during robot-assisted surgery can be started within seconds once the arms of the robot are removed from the patient. Complete access to the patient could only be achieved, however, when all trocars were released and the complete robot removed.
A debriefing and summarizing flow diagram of this specific crisis management helped to improve the time for the resuscitation measures at the second simulation. An interdisciplinary simulation including all departments involved in a regular operating room is strongly recommended.
Footnotes
Disclosure Statement
No competing financial interests exist.