
Abstract
Background and Purpose:
Placement of the fourth arm (4th arm) in the lower quadrant (LQ) is commonly described for robot-assisted renal surgiocal procedures but has anatomic restrictions and limited ergonomics. An alternative, upper quadrant (UQ) location is desirable, but patient habitus and spacing may restrict robotic attachment. We investigate current trends in 4th arm port placement and propose an alternative method at attaching the robot—the “Floating Arm” (FLA).
Methods:
Robotic surgeons from the Endourological Society were surveyed. A 20-cm extra-long (XL Protype) da Vinci instrument was developed for the FLA technique. A dry lab allowed quantitative comparison of spacing and ranges of motion for standard da Vinci ports (dVP), bariatric dVP, telescoping dVP, and FLA.
Results:
There were 108 respondents who participated. Half of the respondents avoid using the 4th arm (30% lack of need and 20% because of interference). The majority (90%) typically positions the 4th arm in the LQ, but many reported limitations in this location. Few (5%) place 4th arm in the UQ, while most (73%) have never heard of UQ placement. Existing techniques may increase shoulder height clearance but inversely shorten the working length of the instrument intracorporeally. Alternatively, the XL Protype significantly increased the shoulder length and maintained available working distances intracorporeally. Adjacent arm interference angle was essentially identical (27 degrees) for all ports except a greater range of movement for the XL Protype (35 degrees).
Conclusion:
Few surgeons are using an UQ positioning or use techniques to improve attachment of the 4th arm. The greatest freedom may be obtained by implementing the FLA, but this necessitates production of a longer instrument.
Introduction
A
If the 4th arm is used, the lower quadrant (LQ, inferior/lateral location) is the most common position but has movement restrictions and limited ergonomics within the abdomen for retraction and use. 5 –7 Alternatively, an upper quadrant (UQ, superior/medial location) may be chosen but historically has been avoided because of difficulty attaching the robot (from the robotic elbow contacting the patient).
To overcome some of these obstacles, surgeons have tried longer (bariatric) ports or even placing a robotic port within a standard laparoscopic port (“telescoping”), but neither have sufficiently eased anatomic restrictions and clashing. 8,9 We present our solution to improving placement of the 4th arm arm during upper tract surgical procedures by proposing the “Floating Arm” (FLA)—a robotic port attached away from the body that potentially has no direct contact with the patient other than the working instrument.
Methods
XL Prototype engineered
Our goal was to position the robotic arm farther from the patient to improve spacing between the robotic elbow and the patient. This would necessitate two changes to current capabilities: (1) Produce a longer instrument and (2) develop a method for a functional arm attached at a greater distance from the patient. A 20 cm extra-long Prograsp-like da Vinci instrument (XL Protype) was engineered in our laboratory (Fig. 1) and investigated using an FLA technique—a robotic arm attached to a port, but not physically touching the patient. The FLA allows use of a longer instrument, where the instrument is inserted through a standard da Vinci port (dVP) that is already attached to the robotic arm, passes through some portion of unprotected air, and then placed through an additional port that is placed through the abdominal wall (Fig. 2).

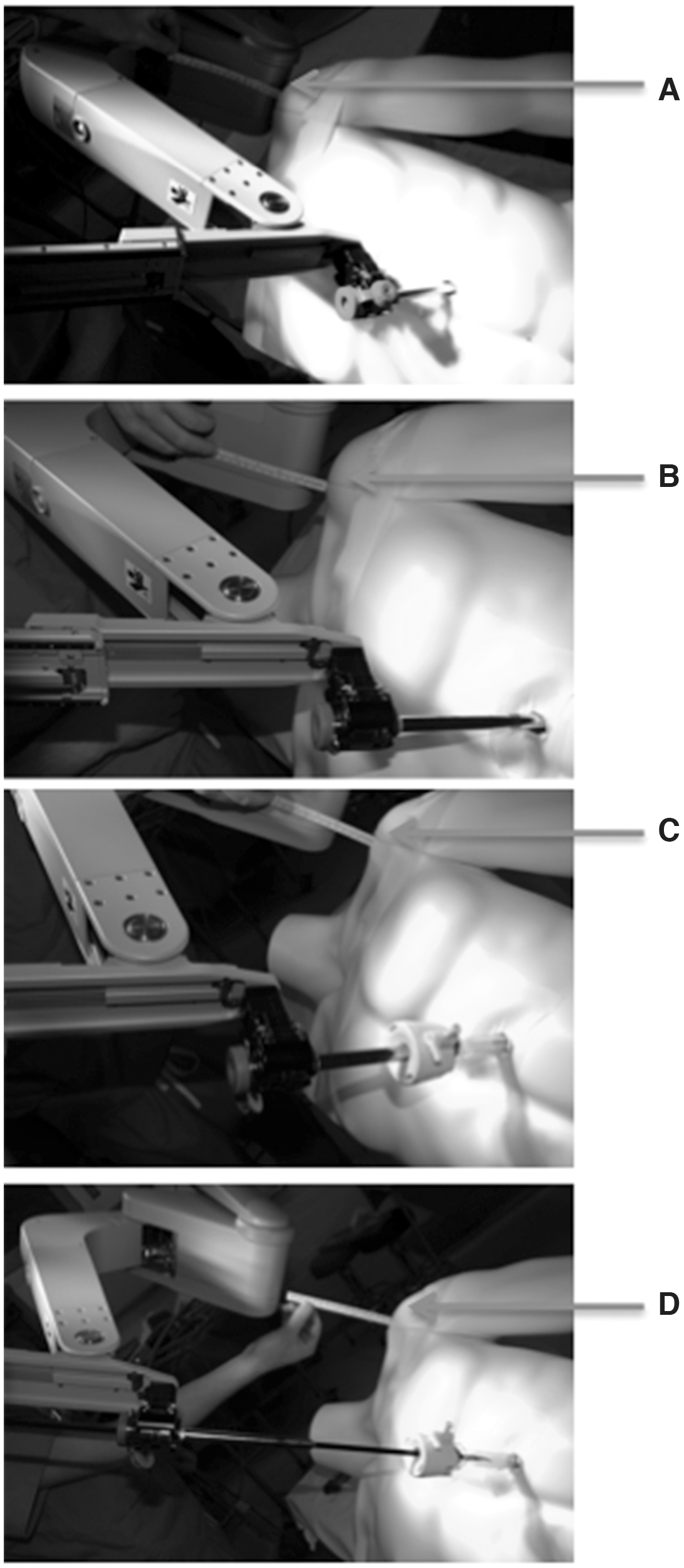
Port combinations to increase distance from the skin for robotic attachment using different port configurations: Standard da Vinci port (dVP), long (bariatric) dVP, standard and long dVP telescoped, and the XL Protype floating dVP.

Attaching the robotic port away from the skin, using an extra-long protype instrument with the Floating Arm technique allows more options for fourth arm placement such as an upper midline abdominal location. Ports 1, 3=working arms; port 2=camera port; port 4=floating port (note the end of the standard da Vinci port is “floating in air” and not inserted through the skin; an instrument passes through port 4, through unprotected air, then through a standard laparoscopic port); port 5=assistant port in the periumbilical region.
Dry lab: Mock patient port setup and measurements
Our dry lab allowed quantitative comparison of spacing and ranges of motion for standard dVP, long/bariatric dVP, telescoping dVP, and the FLA technique. The da Vinci S robot system was docked on a full body plastic mannequin, similar to our standard positioning (modified lateral flank position, bed slightly flexed and reverse Trendelenberg to level the horizontal plane). The patient's lateral arm is tucked to the side or across the body and supported. Although our ports are adjusted laterally in obese patients or inferior/superiorly based on the patient's torso length, or depending on the location of the pathology, we typically gain access for the camera port at the periumbilical region with a Veress needle. A bariatric 12-mm port is placed in this location. A standard 12-mm assistant port is placed in the periumbilical region. One robotic port is placed 8 to 9 cm lateral to the camera port and the other working port placed 8 to 9 cm superior/medial to the camera port. The 4th arm port is then placed at least 8 to 9 cm superior to this supraumbilical working port, but its position is altered laterally to allow robotic arm attachment without contacting the patient. The da Vinci S surgical system is used in all procedures and is brought in posteriorly at approximately a 20-degree angle toward the head of the patient for docking (Fig. 2).
The maximum distance the instrument could be inserted past the end of the port was measured (effectively the intracorporeal working length) (Fig. 1). The distance from the 4th arm elbow to the closest point of possible interference from the mannequin's body (the shoulder) was measured for the different combinations of port placement (standard dVP, long/bariatric dVP, max standard/telescoping dVP, max long/telescoping dVP, XL Protype floating dVP) (Fig. 3). The “swinging angle” from the adjacent working port was also compared among the various port options (i.e., how far the adjacent port could swing before striking the 4th arm or instrument).
Distance between robotic elbow and shoulder using: (
Surveying trends in 4th arm use and position
To better understand trends among other robotic surgeons, a 10-question survey was e-mailed to all members of the Endourological Society in English (n∼1900 worldwide members) querying their robotic training, experience/preferences toward use of the 4th arm in upper tract surgery, and their experience in different port locations. A standard online accessible survey was constructed (Survey Monkey,
Results
Survey
A total of 108 respondents from the Endourological Society participated in the survey. Approximately 43% were fellowship trained in robotic surgical procedures, while 29% were primarily trained with robotics through their residency. The other 28% were taught robotics by colleagues or self-taught. When asked whether the respondents typically use the 4th arm in renal surgery, 46% replied “No,” of whom some justified this choice as one or more of the following: Lack of need (30%), instrument/camera/patient/assistant interference (“clashing”) outside the abdomen (20%), or (“clashing”) inside the abdomen (9%). Respondents most often used the 4th arm for partial nephrectomy (93%), followed by nephroureterectomy (63%), then total nephrectomy (45%) and pyeloplasty (38%). The greatest role for the 4th arm was in kidney retraction and bowel retraction.
The majority of respondents (90%) typically place the 4th arm in the inferior/lateral (LQ) position. Many limitations were experienced with placing the 4th arm in the LQ during a procedure including one or more of the following: Robotic arm clashing (76%), lack of available space for port placement (63%), conflict with kidney tumor location (14%), and difficulty retracting the kidney (9%). Very few (5%) respondents routinely place the 4th arm in the UQ, while most (73%) have never heard of placing the 4th arm superiorly. Last, the majority (68%) never telescope the 4th arm ports to gain extra length or try to avoid instrument collision.
Dry lab
Multiple available robotic ports (standard and long/bariatric) were aligned adjacent to each other with different combinations of telescoping or floating into a standard port for comparison of lengths (Fig. 1). The robot was then docked onto a mannequin according to our port placement, with the 4th arm in the UQ. Different measurements were obtained including patient shoulder height clearance (distance between the robotic elbow and the patient's shoulder), available instrument length inside the body, and adjacent arm interference angle (Table 1).
dVP=da Vinci port.
The floating port had the greatest clearance from the shoulder at 16 cm, while the standard/telescoping port had only 1 cm of clearance; the robotic arm was touching the patient shoulder with the standard port (Fig. 3). Adjacent arm swing angle before contacting the adjacent arm was similar in all ports (range of freedom 27–28 degrees), except the floating port with a range of freedom of 35 degrees. Maximum instrument length inside the body was 17.3 cm for the floating port, while the standard/telescoping was 20.5 cm, and the standard port was 22.5 cm. Maximizing the telescoping technique with the standard or long port resulted in longer clearance distance from the shoulder, 5 cm and 9.3 cm, respectively, but an inversely smaller working length inside the body, 15.1 cm and 10.3 cm, respectively (Table 1).
Discussion
The use of the 4th arm allows for more autonomy by the robotic surgeon at the console, allows less dependence on the skill of the assistant, and releases the assistant for other assisting duties. Our survey demonstrated an increased use of the 4th arm for more complex surgeries, such as a partial nephrectomy and nephroureterectomy. While the survey demonstrated about 50% of surgeons use the 4th arm routinely, much disdain originates with anatomic limitations imposed in the lower/lateral quadrant, a configuration approximately 90% of survey respondents use. Placement of the 4th arm in the lower quadrant is further complicated in patients with smaller bodies or prominent hip bones. To overcome the external obstacles, some surgeons have suggested using the longer robotic ports (bariatric ports). About 32% of respondents have even tried telescoping the daVinci port inside a standard port to gain extra length for robot attachment and possibly decrease external conflict. Even with many of these adaptations, 4th arm conflicts are still common and may lead to decreased use, limited dexterity, or limit locations of the robotic instruments.
Limitation in the LQ led us clinically to investigate other potential 4th arm port placement options. We tried placing the 4th arm in the UQ, a position often used during pure laparoscopic upper tract surgical procedures for an additional assistant port, but many patients' body habitus interfered with robotic attachment and the elbow of the robot contacted the patient. Clinically, this forced us to move the UQ port more laterally (as one moves the port more medial in a patient in the modified lateral position, this decreases distance between the robotic elbow and the patient). As in LQ positions, longer bariatric ports helped in some patients, but still had limitations in many patients. 9
The FLA allows port placement near the midline and, therefore, differs from previous descriptions within the literature. 5 –7 In our experience, the advantages of UQ port placement include: Ability to retract the bowel medially, ability to retract the liver, and the ability to elevate the kidney and retract it medially or laterally with much less intra-abdominal interference with other instruments. By manipulating the instrument from a cranial position, the 4th arm may perform multiple functions at once—for example, retraction of the liver with the instrument shaft while retracting the kidney with the instrument jaw and tip. This potentially eliminates the need for accessory laparoscopic instruments that are typically used solely for liver retraction in right-sided renal surgery.
Our dry lab compared standard, telescoping, and floating ports to seek ideal logistical use and limitations in UQ utility. As extrapolated in Figure 1, the long bariatric port is almost identical in size to the standard/telescoping port used by other authors. The standard, long, and standard telescoping robotic ports placed in the UQ had close proximity to the ipsilateral shoulder and were not feasible to use, despite having the longest instrument reach inside the body. The max standard/telescoping and max long/telescoping ports improved arm attachment and safe shoulder height clearance, but had reduced remaining instrument length inside the body. Surprisingly, having a longer port and thus higher location for robotic arm attachment did not significantly affect adjacent arm interference. The angles for adjacent arm freedom of movement were essentially similar, with the FLA having the most freedom.
Regardless, the advantage of the UQ 4th arm port placement is that the adjacent robotic arm is usually swung away from the 4th arm during kidney and hilar dissection, and thus would still be less likely to clash externally in this location. Although the swing angle was minimally improved with the longer floating port, the longer XL Protype does allow positioning the ports more medially and, consequently, improves the distant between robotic arms and decreases clashing of robotic arms. Thus, with a floating port, one may move the UQ port toward the midline, a position that clinically is unobtainable because of arm/body interference with all other port combinations (Fig. 4).
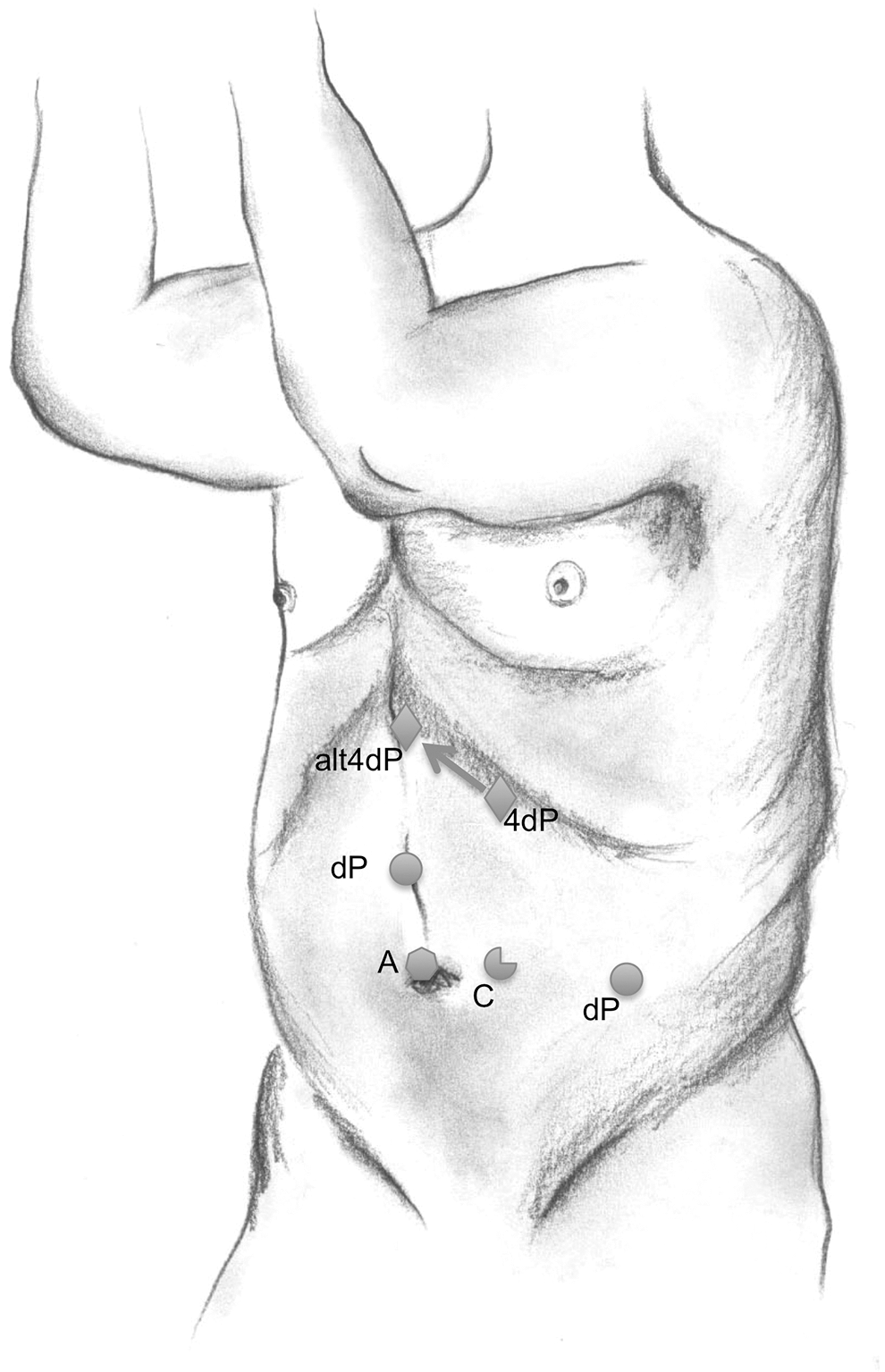
Using the XL Protype (extra-long da Vinci instrument) and a floating arm, one may move the upper quadrant 4th arm port more medial/superior (arrow). A=assistant port; C=camera port; dP=working arm; 4dP=4th working arm; alt4dP=alternative medially placed 4th arm position.
Clinically, we have attempted floating ports with currently available standard instruments, but we experienced short intracorporeal lengths and limited floating heights. Longer instruments (such as our Protype X) are not currently available for clinical applications. As depicted in Table, while the standard port allowed a maximum instrument length inside body to be 22.5 cm, when using the long port telescoped within a standard port, the intracorporeal instrument distance was reduced to 10.3 cm.
Realizing that port attachment's limiting factor hinges greatest on instrument length, we developed a prototype grasping instrument 20 cm longer than existing robotic instruments (XL Protype). One can float the port in and out depending on the amount of distance needed within the abdomen, realizing that for every cm one floats the port out, this reduces the amount inside the abdomen by an equal amount. With the XL Protype, the instrument length inside the body was maintained adequately at 17.3 cm, greater than telescoping ports. This extended length allowed us to truly “free float” the port and greatly improve the clearance distance from the patient's body and the 4th arm elbow, while maintaining instrument working length. This would potentially allow most anatomic positions for the 4th arm, while removing limits imposed by a patient's body habitus.
There are some cautions to take into account with the FLA technique. The instrument is inserted through a standard dVP, passes through some portion of unprotected air, and then needs to be manually placed through an additional port. This limitation could easily be overcome by producing an extra-long dVP to compliment the extra-long instrument. Nonetheless, once the 4th arm is guided intracorporeally, it is rarely removed; if the instrument is removed or changed, the assistant needs to guide it back through two ports (rather than one).
In addition, whether using the telescoping or floating techniques, the fulcrum of the robotic arm changes. The fulcrum in standard robotic port application, also known as the remote center, lies at the fascia level. 10 This fulcrum limits excessive torque at the abdominal wall and instrument. Because the 4th arm is primarily used for retraction, there are usually minor amounts of movement of the robotic arm, and the standard port traversing the fascia provides some protection. Burping the port, by using the clutch button, will change the remote center and make the movement as free as possible, likely relieving any tension on the abdominal wall.
The authors acknowledge some limitations with their survey. While the Endourological Society e-mail list includes approximately 1900 contacts worldwide, these may include duplicate e-mails, nonrobotic surgeons, urologists without access to a robot, and some nonrespondents. Only an English version was distributed, and this may have limited some responses as well. Furthermore, only one e-mail request was distributed. Nonetheless, we assert that our survey was meaningful in helping understanding current trends among other robotic surgeons and to substantiate our pursuit of technical refinement.
Conclusion
Currently, the 4th arm is underutilized, especially in the UQ, because of external interference with port attachment or instrument clashing. Protype XL and the FLA technique offer a solution for more optimal and safer use of the 4th arm.
Footnotes
Disclosure Statement
Dr. Johnston is on the speaker's bureau for Janssen Biotech/Johnson/Johnson and Medivation/Astellas. For the remaining authors, no competing financial interests exist.