
Abstract
Background and Purpose:
Distinguishing calcium oxalate from uric acid stones is critical to identify those patients who may benefit from dissolution therapy and can also help direct preventive measures for stone growth. We aim to study whether 24-hour urine analysis may predict the urinary stone composition.
Patients and Methods:
We retrospectively identified patients with calcium oxalate and uric acid stone compositions who also had a 24-hour urine collection within 3 months of stone analysis. Patients with calcium phosphate, cystine, and other stone compositions were excluded. Subjects were divided based on their stone type (calcium oxalate vs uric acid stones) and were compared according to demographic data and 24-hour urine analysis. Logistic regression analysis was performed to assess the association between stone composition and covariates. A nomogram was then constructed to predict uric acid stones over calcium oxalate stones.
Results:
Of the 1163 patients identified, 1054 (90.6%) had calcium oxalate stones and 109 (9.4%) had uric acid stones. On logistic regression, body mass index (BMI) (odds ratio [OR] 1.351, 95% confidence interval [CI] 1.133–1.609; P<0.001), urinary sodium (OR 1.021, 95% CI 1.004–1.037; P=0.013), calcium (OR 0.987, 95% CI 0.979–0.996; P=0.003), oxalate (OR 0.890, 95% CI 0.804–0.985; P=0.024), and uric acid (OR 0.989, 95% CI 0.982–0.997; P=0.005) were significant predictors for urinary stone composition. The nomogram with the highest concordance index (c-index=0.855) was obtained using age, BMI, urinary sodium, calcium, oxalate, and uric acid as variables.
Conclusion:
Distinguishing uric acid from calcium oxalate stones can be performed with relative accuracy using parameters from the 24-hour urine stone risk profile and the patient's BMI and age.
Introduction
U
Identifying those with uric acid stones can also help direct medical approaches to decrease stone recurrence. 7,8 Empiric dietary, 8,9 behavioral, 10 and medical therapies 7 may be effective; however, directed therapy may be more effective, if uric acid nephrolithiasis is confirmed by 24-hour urine collections and stone composition analysis. 11
Although an individualized approach based on the stone composition is desirable, it is not always possible. Only patients who undergo endoscopic stone retrieval (ureteroscopy, percutaneous nephrolithotomy) or recover a spontaneously passed stone may have their stones analyzed and thus have the composition revealed. Attempts have been made to correlate CT imaging (single and dual energy noncontrast) to the stone composition with promising initial results. 12 –14
Our objective was to determine whether 24-hour urine stone risk profiles can predict the kidney stone composition. Using this information, we propose a nomogram that may help guide clinical practice.
Patients and Methods
Study design
After Institutional Review Board approval, we identified patients with nephrolithiasis who had a 24-hour urine collection and a stone composition analysis within 3 months of each other. Dates of service ranged from January 2006 through December 2011. Recorded data included: age, sex, body mass index (BMI), stone-related medications (i.e., allopurinol, potassium citrate, loop diuretics, thiazides), 24-hour urine analysis (volume, sodium, calcium, oxalate, uric acid, citrate, and pH), and stone composition. Stone composition was performed on samples obtained from spontaneous passage or surgical stone extraction. Stones were analyzed by infrared spectroscopy and defined as calcium oxalate or uric acid stones based on a predominance (greater than 50%) of that composition.
Patients with calcium phosphate, struvite, and cystine stones were excluded because of a relatively small sample size of these less common stone compositions. Patients were excluded if they were <18 years old or if they were taking allopurinol, potassium citrate, loop diuretics, or thiazides.
Statistical analysis
Continuous measures were described as means, standard deviations, and percentiles. Categoric measures were summarized using frequencies and percentiles. The paired two-sample Student t test and the Pearson chi-square test were used to evaluate the relationship between stone composition and the continuous and the categoric measures, respectively. Logistic regression was performed to assess the association between stone composition and covariates (age, BMI, sex, 24-hour urine stone parameters). SAS 9.3 software (SAS Institute, Cary, NC) was used for all analyses. A nomogram was then created to predict uric acid stones over calcium oxalate stones using R 2.15.2 software (R Foundation for Statistical Computing, 2.15.2). All tests were performed at a significance level of 0.05.
Results
We identified 1163 patients with a diagnosis of nephrolithiasis who had a 24-hour urine analysis and stone composition within 3 months of each other and satisfied all of the exclusion criteria. There were 1054 (90.6%) patients who had calcium oxalate stones and 109 (9.4%) who had uric acid stones.
Patients with uric acid stones were older (60.9 vs 50.5 years; P<0.001), more likely to be male (74.3% male vs 60.8% female; P=0.006), and had a higher BMI (32.4 vs 28.4 kg/m2; p<0.001) than patients with calcium oxalate stones. They also had significantly lower urinary calcium (162.5 vs 235.6 mg/24 h; P<0.001), uric acid (507.3 vs 584.6 mg/24 h; P<0.001) and pH (5.7 vs 6.0; P=0.002) (Table 1).
On logistic regression, BMI, urinary sodium, calcium, oxalate, and uric acid were significant predictors of urinary stone composition. BMI was the most significant predictive factor for uric acid stones over calcium oxalate stones (odds ratio [OR] 1.351, 95% confidence interval [CI] 1.133–1.609; P<0.001). Having high urinary sodium resulted in a higher risk of uric acid stones (OR 1.021, 95% CI 1.004–1.037; P=0.01), whereas high urinary calcium (OR 0.987, 95% CI 0.979–0.996; P=0.003), oxalate (OR 0.890, 95% CI 0.804–0.985; P=0.024), and uric acid (OR 0.989, 95% CI 0.982–0.997; P=0.005) were associated with a lower risk.
The nomogram with the highest concordance index (c-index=0.855) was obtained using age, BMI, urinary sodium, calcium, oxalate, and uric acid as variables (Fig. 1). When urinary pH, a variable commonly associated with uric acid stone risk, 15 was added to the nomogram, it resulted in a slightly lower c-index of 0.826.
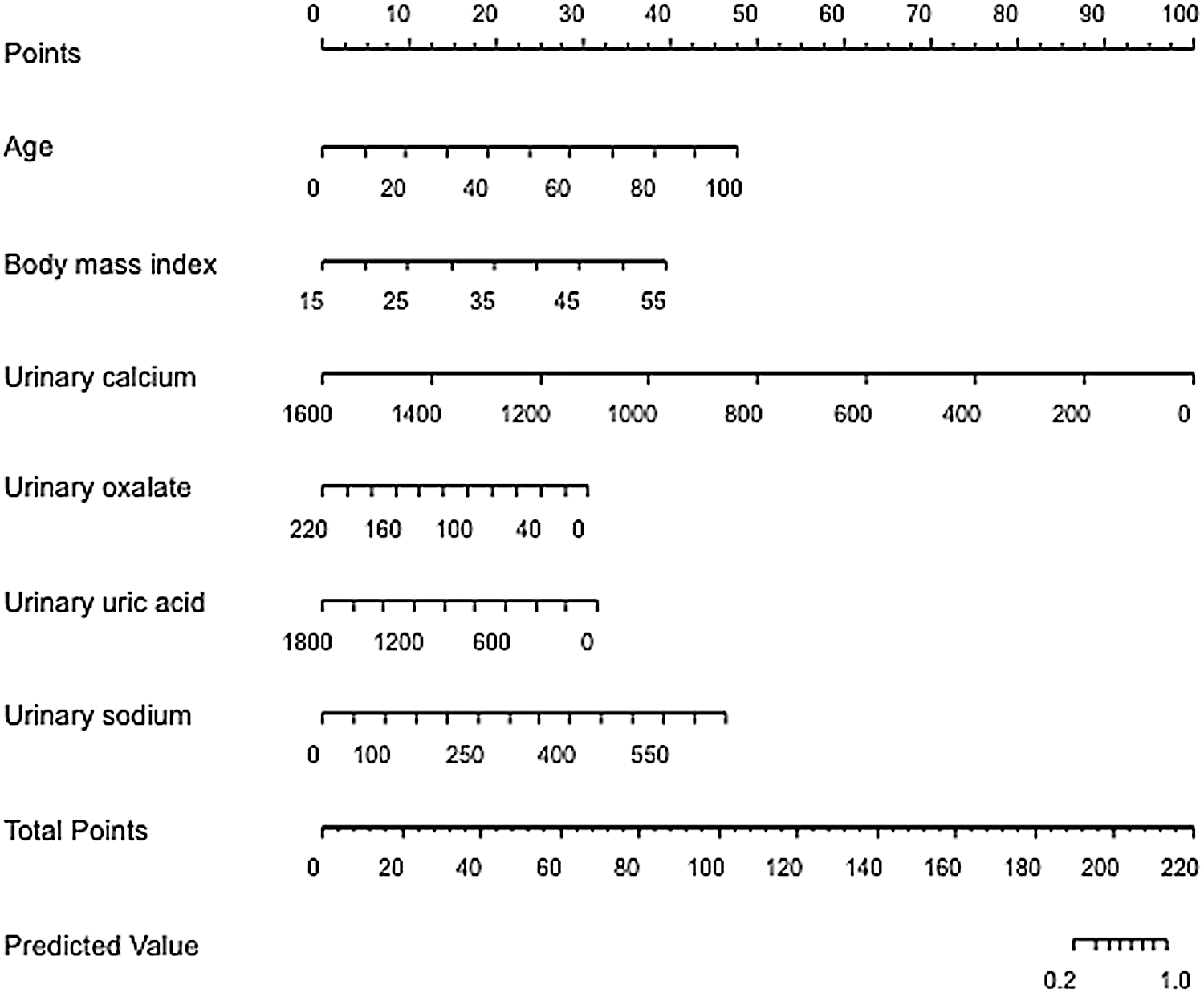
Nomogram to predict urinary stone composition (uric acid over calcium oxalate stones). C-index=0.855.
Discussion
Stone composition guides clinical treatment of stone patients, identifying candidates for dissolution therapy and tailoring interventions to help decrease stone recurrence. 5 –9 Unfortunately, a stone analysis is not available for every stone patient. We attempted to identify surrogate markers for stone composition that could help direct stone management.
Our study demonstrated that a higher BMI and urinary sodium were associated with a higher risk of uric acid stones, while higher urinary calcium and oxalate were associated with calcium oxalate stones. We speculate that obesity and metabolic syndrome are commonly associated with dietary behaviors that increase the risk for disease, which in this situation may include a higher sodium intake; this hypothesis would need to be tested with dietary logs or on a controlled diet. Interestingly, a higher uric acid was more predictive of a calcium oxalate stone, perhaps emphasizing the importance of the concept of heterogeneous nucleation. 16,17
Several studies have been performed evaluating the ability of imaging to predict urinary stone composition. 12 –14,18 Batchelar and associates 18 developed a laboratory system for collecting coherent scatter signals from intact kidney stones. This technique was performed using a diagnostic X-ray tube and image intensifier that could recognize six common stone components (calcium oxalate monohydrate, calcium phosphate, calcium phosphate dihydrate, cystine, struvite, and uric acid). Currently, single and dual energy CT scans have been used to predict urinary stone composition. 12 –14,19,20 Kulkarni and colleagues 13 evaluated in vitro and in vivo models to characterize urinary stones using single source dual-energy CT. Uric acid and nonuric acid stone were identified using two-material decomposition (material density iodine/water) algorithms. Hounsfield unit measurements alone were only 71% sensitive and 69% specific in detecting the uric acid stones.
Spettel and coworkers 21 evaluated the combination of Hounsfield units from a CT scan and urinary parameters as a single tool to predict uric acid stones in a study with 235 patients (212 calcium, 22 uric acid stones). Hounsfield unit (≤500) and urinary pH (≤5.5) combined resulted in a sensitivity of 86% and specificity of 98%, and a positive predictive value of 80%, to determine uric acid stones. In our study, we were able to predict uric acid stones with relative accuracy without relying on CT imaging. This also allows patients with documented stones on radiography or ultrasound imaging to forego the expense and radiation exposure of a CT scan before medical management. Further studies are warranted, evaluating the utility of adding Hounsfield unit measurements to our nomogram.
Other studies have linked some 24-hour urinary parameters to specific stone compositions. 11,22,23 Moreira and colleagues 22 in a study with 110 calcium phosphate stone formers, compared patients with apatite stones with patients with brushite stones, and concluded after a multivariate analysis that brushite stones were associated with higher urinary calcium (329.7 vs 204.8 mg; P<0.001) and higher urinary super saturation of calcium phosphate (2576 vs 1423; P<0.001) when compared with apatite stones. In another study, 24-hour urine parameters were able to predict in 61%, 69%, 56%, and 71% of calcium oxalate, uric acid, calcium phosphate and other (cystine/struvite) stone compositions, respectively. In this study, the overall accuracy was not high with a score of 64%. 23
Our model possesses a relatively high c-index of 0.855, which is on a scale of 0.5 (random chance) to 1.0 (perfect discrimination). To use this nomogram, one would locate their patient's age, then draw a line straight up to find the corresponding points score. This is then repeated, for the rest of the components, and the final score is calculated and plotted on the total points scale. Total scores below 190 would predict that the stone is not uric acid, such that a trial of dissolution would not be warranted.
Interestingly, when urinary pH was added to the nomogram, the c-index dropped to 0.826, suggesting that urinary pH may be less influential when comparing uric acid with calcium oxalate stones. Probably, a low urine pH plays a major role in the uric acid pathogenesis, but it is less important when trying to distinguish between uric acid and calcium stones, especially when other variables are taken into account, such as urinary sodium, calcium, oxalate, or uric acid. This may relate to the fact that calcium oxalate stone formation occurs independent of urinary pH.
Pursuing dissolution therapy involves hydration, urine alkalization (with a target urinary pH of 6.2–6.8 24 ), with or without the addition of allopurinol. Using this nomogram, one could identify the patient's chance of having a uric acid stone, and then counsel the patient on the options of dissolution therapy vs surgical management, including discussions of stone size, location, and patient symptoms. The side effects of medical management and potential risk of treating the incorrect type of stone would be weighed against the improved efficacy of surgery, with its known morbidities.
Because of the retrospective nature of our study, several limitations exist. Selection bias may be present because all patients were evaluated and treated at our tertiary care center. Patients were limited to those with uric acid or calcium oxalate stone compositions; future studies will test the validity of the nomogram construct using calcium phosphate, struvite, and cystine. Uric acid calculi were included if >50% of the stone composition was uric acid. Outcomes with dissolution therapy for mixed stones with varying proportions of uric acid (e.g., 50%–60%, 6%–70%, etc.) have not been reported. Also, it is possible that patients may harbor multiple stone types simultaneously, or changes in composition may occur over time. 25 It will be important to validate our nomogram in other populations.
Conclusion
Differentiating uric acid stones from calcium oxalate stones using 24-hour urine stone risk parameters and patient characteristics appears to be feasible. Age, BMI, urinary sodium, calcium, oxalate, and uric acid may be used together to predict stone composition with a significant level of accuracy.
Footnotes
Disclosure Statement
No competing financial interests exist.