
Abstract
Background and Purpose:
Ureteral reconstructive surgery necessitates adequate exposure of the ureteral lesion and results in large abdominal incisions. Robot assistance allows the performance of complex ureteral reconstructive surgery through small incisions. The current series includes only cases of Boari flaps performed by robot assistance and attempts to describe in detail the technique, review the literature, as well as to expand the experience in the current literature.
Patients and Methods:
Eight patients underwent ureteral reimplantation by Boari flap technique. The indications for the performance of the procedure included ureteral stricture from iatrogenic injury in three patients, recurrent ureteral stricture after multiple endoscopic stone management procedures in one patient, ureteral stricture from previous malignant disease in the pelvis or abdomen in three patients, and ureteral stricture due to trauma in one patient. Five cases were located in the left side and three cases in the right side. A variety of parameters were recorded in a prospective database including the time for robot docking and total operative time as well as catheterization and drainage time. The follow-up of the patients included the performance of renal ultrasonography 4 weeks, 3, 6, and 12 months after the procedure.
Results:
Mean age of the patients was 50.8 (range 39–62) years and mean body mass index was 26.2 (range 23.22–29.29) kg/m2. Operative time ranged 115 and 240 (mean 171.9) minutes. Mean blood loss was 161.3 (50–250) mL. Conversion to open surgery did not take place in the current series. No intraoperative complications were observed. Postoperative complications included one case of prolonged anastomotic leakage.
Conclusion:
The robot-assisted approach is efficient in the performance of ureteral reimplantation with Boari flap. Low blood loss, short catheterization time, low complication rate, and excellent reconstructive outcome are associated with the approach. Robot assistance seems to be beneficial for ureteral reconstructive surgery.
Introduction
U
The length of the ureteral lesion is the most important factor for the determination of the most appropriate procedure for ureteral reconstruction and reimplantation. In fact, implantation by ureterocystotomy is usually indicated for short defects of 4 to 5 cm, while larger defects need either the psoas hitch and/or Boari flap. Ureteral lesions between 6 and 10 cm could be bridged by psoas hitch, and longer lesions up to 15 cm by the additional performance of a Boari flap. 3
The need for adequate exposure of the lesion and the subsequent management of the involved structure results in a large abdominal incision. The latter is associated with significant morbidity. 3 The advent of the DaVinci (Intuitive Surgical Inc., Sunnyvale, CA) system provided magnified three-dimensional vision of the operative field, precision in movements, and increased degree of movement in comparison with conventional laparoscopic and open surgical approaches. 4 These advantages rendered the performance of complex reconstructive surgery possible through a few small abdominal incisions, and several investigators have proposed their experience with reconstructive procedures of the ureter. 2,3,5 –10
Nevertheless, the technique of Boari flaps has been scarcely presented among the above case series and counts a small number of cases. 3,4,10,11 The current series includes only cases of Boari flaps performed with robot assistance and attempts to describe in detail the technique, review the literature, as well as to expand the experience in the current literature.
Patients and Methods
Eight patients underwent ureteral reimplantation by Boari flap technique. The indications for the performance of the procedure included ureteral stricture from iatrogenic injury in three patients, recurrent ureteral stricture after multiple endoscopic stone management procedures in one patient, ureteral stricture from previous malignant disease in the pelvis or abdomen (no sign of disease at the time of procedure) in three patients, and ureteral stricture from trauma in one patient. Five cases were located in the left side and three cases in the right side.
Cases of iatrogenic injury were associated with pelvic surgery, which resulted in accidentally ligating or injurying the ureter. Usually these cases are associated with strictures that tend to become longer after the first endoscopic treatment sessions. Cases of malignant disease were associated with lymphoma, cervical and testicular cancer. Two surgeons experienced in laparoscopy and robotics performed the procedures. The technique performed replicated the steps of the open procedure of Boari flap according to Übelhör and was based on the principles previously described by other investigators. 3,12
Surgical technique
Patient positioning and trocar placement
The patient is placed in a dorsal supine position with legs abducted to allow the placement of the robotic system between them. The patient is set in a steep Trendelenburg position of approximately 15 degrees during the robot docking (Fig. 1). All procedures were performed with the use of four robotic arms and five trocars.

Patient position. Notice the angle used for the procedure.
A 15-mm supraumbilical midline incision is made, and the abdominal cavity is entered. Stay sutures are placed on the anterior rectus sheath, the optical trocar (Hassan type) is introduced, and pneumoperitoneum is established. An 8-mm robotic trocar is inserted on the left side of the abdomen four fingertips lateral to the midline and 2-cm cephalad of the hypothetical line between the umbilicus and the pubic arch. A laparoscopic instrument could be inserted to facilitate the dissection of any intra-abdominal adhesions and to push the bowel while the remaining the trocars are inserted. A 12-mm conventional laparoscopic trocar is placed two fingers medially and 2-cm cephalad to the right anterior superior iliac spine. The latter port allows the insertion of grasper, clip applicators, endobag, and sutures. Another 8-mm trocar is placed five fingers to the right from the umbilicus and 2-cm cephalad of the hypothetical line between the anterior superior iliac spine and the umbilicus. A fifth trocar (8 mm) is inserted three fingerbreadths medial and 2-cm cephalad to the left anterior superior iliac spine.
The above trocar positioning takes place for cases of right-sided Boari flaps and cases located on the left side when the strictured site is up to the level of the pelvic brim (Fig. 2). In the case of a left-sided procedure, the two robotic trocars are inserted in the right abdominal wall while the third robotic and assistant trocars are inserted on the other side. Robot docking takes place, and the instruments used are the following: a fenestrated bipolar forceps, a large needle driver, a Hot Shear™ (monopolar curved scissors) and a ProGrasp™ forceps.
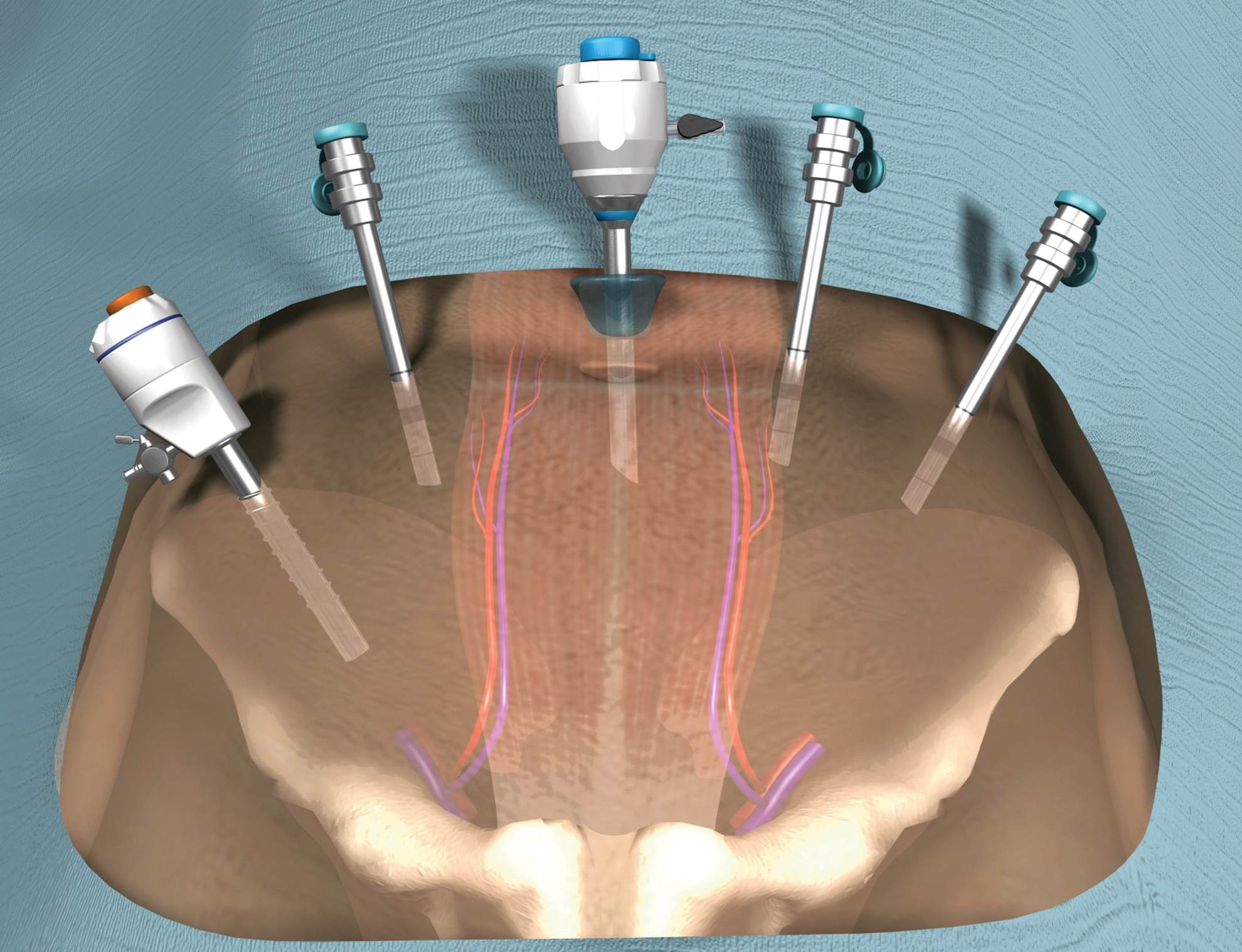
The trocar placement for right-sided Boari flap ureteral reimplantation. The same positioning could be used for long strictures up to the level of the pelvic brim on the left side. Otherwise, left-side cases could be managed with the placement of the trocars in mirror image to the one presented in the figure.
Technique of Boari flap formation
The technique performed is practically a replication of the open Boari flap technique according to R. Übelhör. 12 The cecum or sigmoid colon is initially mobilized depending on the side on which the procedure takes place. The ureter is identified at the bifurcation of the iliac vessels. Careful preparation of the ureter is performed with caudal direction guided to the site of the stricture (Fig. 3a). The ureter is retracted by the fourth robotic arm during the dissection. A clip is placed proximally to the cephalad side of the strictured ureteral segment while the caudal side is transected as distal as possible at the point that the ureter is inserted into the bladder (Fig. 3b). Then, the bladder is mobilized as distal as possible ipsilaterally to the structured ureter. It is very important not to transect the vascular supply of the bladder. Saline was used to fill the bladder, and the surgeon could decide the performance of a Boari flap ureteral implantation. The posterior bladder wall was fixed on the psoas muscle with the use of 3-0 polyglactin suture (psoas hitch).
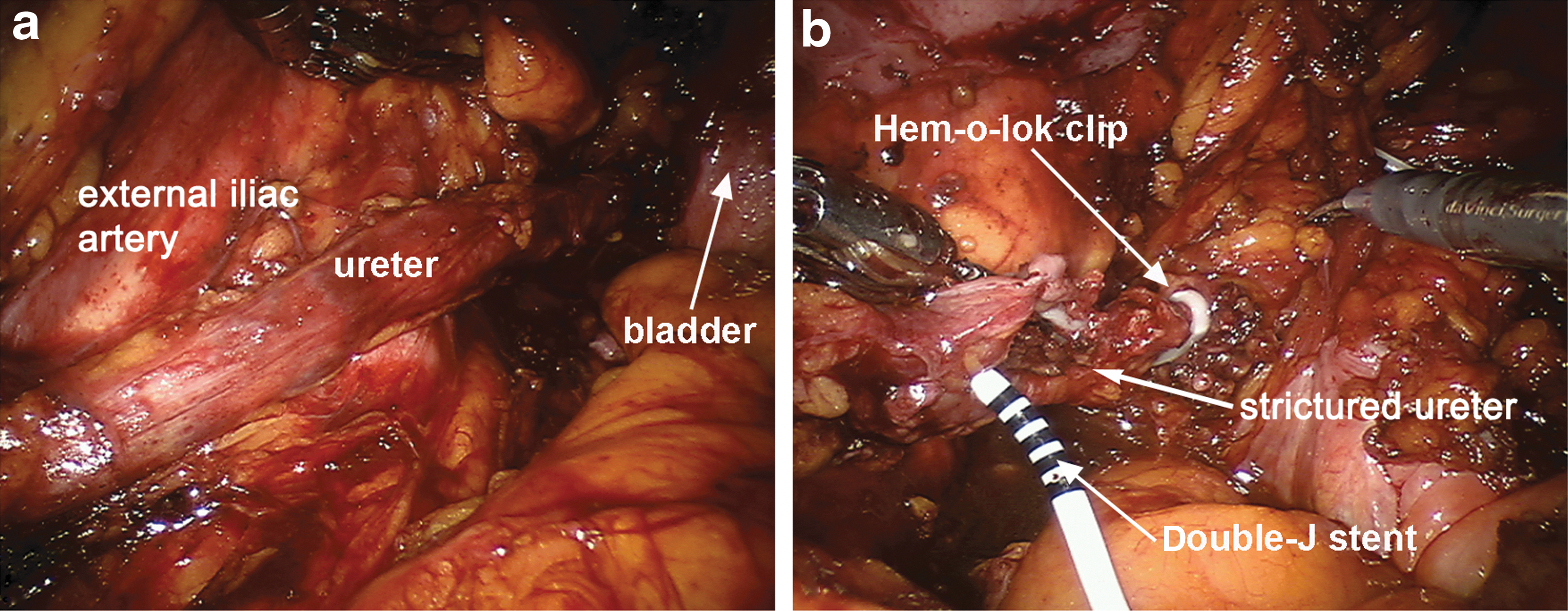
The Boari flap is formed by an incision with a 2:1 proportion in length and width. The ureter is spatulated and implanted through a submucosal tunnel in the apex of the Boari flap (Figs. 4a, b). The implantation of the ureter replicates the technique described by Politano and Leadbetter 13 in the open surgical approach. The ureter is retracted through the submucosal tunnel (Fig. 5a), and the ureteral adventitia is sutured to the mucosa of the flap using 5-0 polyglactin suture (Fig. 5b). At this point, a Double-J stent is inserted in the ureter over a guidewire (Fig. 6a, b) through an 18-gauge needle after the abdominal wall is punctured by a needle appropriate for percutaneous procedures. The flap is then tabularized (Fig 7a).
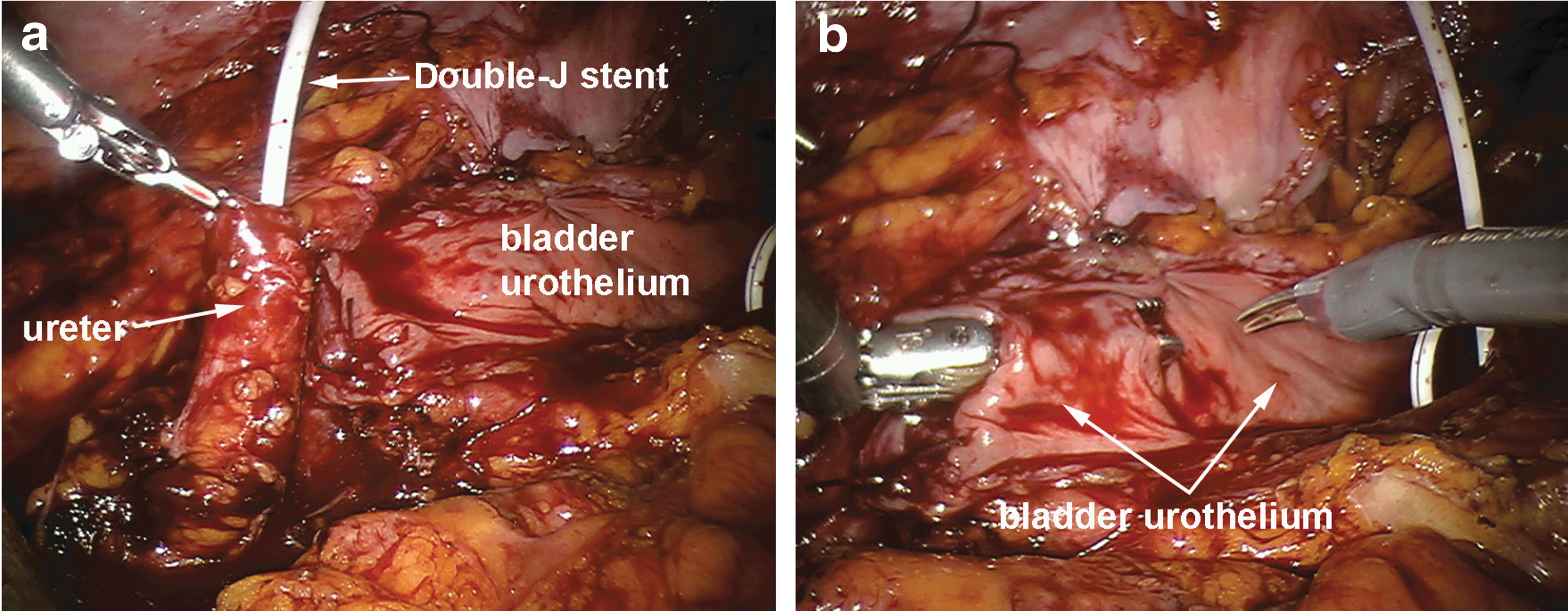



For this purpose, 3-0 polyglactin sutures are used in two layers. The bladder opening is then closed in two layers using 3-0 polyglactin sutures. The bladder is then filled with 200 mL saline to exclude any extravasation. A drainage tube is inserted through the contralateral to the side of the treated ureter 8-mm ports.
Recorded parameters and postoperative management
All cases were recorded in a prospective database. A variety of parameters were recorded including the time for robot docking and total operative time as well as catheterization and drainage time. The drainage was removed on the second postoperative day. If the drainage was associated with high output, the fluid was examined for the presence of creatinine, and the removal or not of the drainage tube was decided. A cystographic examination of the bladder took place on the sixth postoperative day, and the healing of the bladder incision as well of the ureteral anastomosis was assessed. When no leakage was observed, the catheter was removed. The Double-J stent was removed after at least 4 weeks.
The follow-up of the patients included the performance of renal ultrasonography 4 weeks after the removal of the ureteral stent or earlier if symptomatology was present. Renal ultrasonography was repeated at 3, 6, and 12 months after the procedure. Cases suspicious for inefficient drainage were further evaluated with computed tomography urography or MAG3 scintigraphy at the discretion of the treating physician. Patients with malignancy were followed according to the indicated schedule for their disease and were evaluated with the above protocol if it was deemed necessary. Perioperative, short- and long-term complications were also recorded and classified according to the Clavien-Dindo classification of surgical complications. 14
Results
Patient characteristics and perioperative results are presented in Table 1. The current series included five male and three female patients with a mean age of 50.8 (range 39–62) years and mean body mass index of 26.2 (range 23.22–29.29) kg/m2. Operative time ranged between 115 and 240 (mean 171.9) minutes. Mean blood loss was 161.3 (50–250) mL. Conversion to open surgery did not take place in the current series. No intraoperative complications were observed.
SD=standard deviation; BMI=body mass index.
The catheter was removed according to schedule in all patients (Fig. 7b), except for one patient. In the latter case, a prolonged anastomotic leakage was diagnosed during the cystography examination on the sixth postoperative day. The urinary leakage gradually decreased, while the drainage tube was already removed on the fourth postoperative day. The patient had prolonged catheterization (grade I complication). The 12-month follow-up of the patients did not show any significant complication associated with the procedure.
Discussion
Reconstructive surgery of the upper urinary tract represents a challenging field necessitating delicate suturing and an operative field extending from the bladder to the proximal ureter. The large incision, which is usually necessary, is balanced by the functional outcome for the patient. The emergence of the laparoscopic approach allowed the performance of reconstructive ureteral surgery without the performance of large incisions and minimized the incision-related morbidity. In fact, the laparoscopic approach was associated with lower blood loss, less pain, improved visualization and cosmesis in comparison with the open approach. 15 –17 The robot-assisted approach combines the advantages of the laparoscopic approach with improved dexterity from the increased degree of freedom of robotic instruments, improved field magnification, and three-dimensional visualization. These characteristics result in a shorter learning curve for the experienced open surgeon in comparison with the laparoscopic approach. 18,19
Reconstructive robot-assisted surgery of the upper urinary track is currently evolving, and cases of ureteral reimplantation, psoas hitch, and Boari flap have been published. 2 Nevertheless, the experience with robot-assisted Boari flap ureteral reimplantations is usually limited to a few cases presented along with a larger series of the aforementioned reconstructive procedures 3,8,11 (Table 2). Musch and associates 3 have reported their results from a series of 16 cases of distal reconstructive ureteral surgery. Their study included five cases of Boari flap ureteral reimplantation that represent the highest number of cases so far. The operative time for the above five cases ranged between 230 and 320 minutes. One case of prolonged anastomotic leakage and one case of bladder wall insufficiency with urinary leakage and peritonitis were encountered.
The current study presents a series of 8 cases of complex ureteral reimplantation by replicating the Boari flap technique of open surgery in the robot-assisted approach. To our knowledge, the number of cases is one of the largest in the literature (Table 2). The operative time of the current study compares favorably with the presented operative time in the literature while the blood loss is also minimal. The complication rate was low and included a case of anastomotic leakage that was detected by cystography on the sixth postoperative day. The latter time point is considered to be early in comparison with the literature, which usually refers to the removal of the catheter on the 7th to 10th postoperative day after the performance of cystography. 1,2,4 The current experience showed that the catheter could be removed 1 day earlier in the cases of Boari flaps probably because of the robot assistance allowing high precision during suturing and the combined performance of cystographic evaluation.
Currently, there is no study comparing open, laparoscopic, and robotic approaches for the performance of Boari flaps ureteral reimplanatation. Nevertheless, there is one study with data on open, laparoscopic, and robotic approaches for ureteral implantation with a psoas hitch. 7 The latter study showed that the robotic approach was associated with lower blood loss and hospital stay in comparison with the conventional laparoscopic and open approach. The above results should be interpreted with care because of the retrospective nature of the above comparison. Another study compared a prospective series of 10 reconstructive procedures of ureteral reimplanation with 10 matched retrospective cases of open ureteral reimplantation. 11 The investigators demonstrated significantly less blood loss and hospitalization time for the robot-assisted procedure in comparison with the open approach while the techniques were equally successful in the management of ureteral pathology. Only one and two cases of Boari flap were included in the open and robotic groups, respectively.
An interesting technical aspect of ureteral reimplantation techniques is the use or not of an antirefluxing technique (submucosal tunnel) for the implantation of the ureter in the bladder. The laparoscopic and robotic literature includes series of ureteral implantation using an antirefluxing technique or series with direct ureteral implantation without the performance of any antireflux technique. 4,8 –10,17,20,21 To our knowledge, the literature is lacking comparative studies between the above implantation techniques, and the final selection of the technique for the robotic approach is based on surgeon preference. 1 The more challenging nature of the laparoscopic ureteral reimplantation may dictate the direct anastomosis of the ureter to the bladder. 1,5 Nevertheless, robot assistance provides the necessary degree of movement that allows the replication of the open surgical approach as described by Politano and Leadbedder. 13
Considering the above in conjunction with the experience of the current series, the robotic approach for Boari flap reimplantation is probably an efficient method that is associated with advantages in terms of blood loss, catheterization, and postoperative course in comparison with the open approach. The laparoscopic approach may be related to a higher technical difficulty in comparison with robotics. Nevertheless, only appropriate comparative studies would eventually prove the benefits of the robotic approach.
The limitation of the current experience is the lack of cases performed for malignant disease. Several investigators have proposed the performance of ureterectomy for malignant urothelial tumors of the upper urinary track in carefully selected patients. 2,3,8 As a result, the presented results should be interpreted on the basis of a reconstructive procedure rather than an oncologic procedure. Nevertheless, the described technique could be used for the excision of malignant tumors with technical modifications such as the excision of the intramural ureter and the careful clipping of the tumor-bearing ureter.
Another limitation is the low number of cases, which should be attributed to the rare indication for the performance of a Boari flap for ureteral reimplantation. Moreover, this series of complex reconstructive procedures was performed by surgeons highly experienced in laparoscopy and robotics. Thus, the reproducibility of the same results in terms of the outcome of reconstruction and complications may necessitate significantly higher operative time and probably a similarly high experience.
The follow-up period of the current series is limited to 12 months; the follow-up data for a longer period (ie, 24 mos) are available for very few cases, and these data do not show any complications. Prospective studies including larger patient populations and longer follow-up would probably be more appropriate for the extraction of solid results on the robot-assisted technique for Boari flap ureteral reimplantation.
Conclusion
The robot-assisted approach is efficient in the performance of ureteral reimplantation with Boari flap. Low blood loss, short catheterization time, low complication rate, and excellent reconstructive outcome are associated with the approach. The presented technique is reproducible and efficient. Nevertheless, a higher number of cases and longer follow-up periods would provide additional documentation and may establish the procedure in the urologic practice. Robot assistance seems to be beneficial for ureteral reconstructive surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.