
Abstract
Purpose:
To determine the occurrence of flank symptoms, flank muscle atrophy, bulge, and hernia formation after open and laparoscopic partial nephrectomy (LPN).
Patients and Methods:
Our prospective Institutional Review Board-approved database was queried to identify 50 consecutive patients who were treated with open partial nephrectomy (OPN) and 50 consecutive patients who were treated with LPN between September 2006 and May 2008. Study patients had: Solitary clinical T1 renal tumor, preoperative and ≥6 month postoperative CT scan performed at our institution, and a confirmed renal-cell carcinoma on the final pathology report. Patients with previous abdominal surgery and neuromuscular disorders were excluded. Oncocare software was used to measure abdominal wall musculature on preoperative and postoperative CT scan. Bilateral flanks were compared for muscle volume, bulge, and hernia. Patients were administered a phone questionnaire to assess postoperative flank symptoms.
Results:
No statistical significant difference was found in the demographics between the two groups. Median age (range) was 59.9 years (20.6–80.7) in the OPN group and 57.5 years (25–78) in the LPN group (P=0.89). Median (range) body mass index and American Society of Anesthesiologists scores were similar between the two groups. On CT scans, median percent variation (range) in abdominal wall muscle volume was significantly greater in the OPN group: −1.03% (−31.4–1.5) vs−0.39% (−5.2–1.8) (P=0.006). The median extent of flank bulge on CT scans (range) was also greater in the OPN group: 0.75 cm (−1.9–7.6) vs 0 cm (−2.7–2.8) (P=0.0004). The OPN group was also more symptomatic, including paresthesia 48% vs 8% (P=0.0053); numbness 44% vs 0% (P=0.002); and flank bulge 57% vs 12% (P=0.007).
Conclusions:
Minimally invasive partial nephrectomy has lesser deleterious impact on flank muscle volume compared with OPN with fewer symptoms of flank bulge, paresthesia, and numbness.
Introduction
C
One of the advantages of LPN over OPN is the decreased trauma of access that results in decreased incisional pain and quicker recovery. In addition, incisional morbidity is reduced with the laparoscopic approach, because the flank incision used for OPN can frequently be associated with intercostal nerve injury and resultant flank bulge in almost 50% of patients. 8 Limited data are available within the literature discussing the actual extent of this bulge, volume change in the abdominal musculature, and the patient perception of flank deformity and symptoms.
The purpose of this study was to compare the objective and subjective impact of OPN via a flank incision vs LPN in terms of flank bulge, flank symptoms, and changes in flank muscle thickness and volume.
Patients and Methods
Our prospective Institutional Review Board-approved database was queried to identify 100 consecutive patients who underwent a partial nephrectomy (50 open and 50 laparoscopic) at the Cleveland Clinic between September 2006 and May 2008 and who satisfied study inclusion and exclusion criteria.
Inclusion criteria consisted of: A solitary ipsilateral T1 tumor, patients with both preoperative and ≥6 month postoperative CT scan performed at our institution, and specimen confirmed to be RCC on pathologic evaluation. Exclusion criteria consisted of: Patients who did not have both preoperative and ≥6 month postoperative CT scan at our institution, any patient with previous abdominal surgery or any neuromuscular disorder, and patients with metastases. Demographic (age, sex, American Society of Anesthesiologists score [ASA], body mass index [BMI]), functional (serum creatinine), operative (tumor size, side of surgery, operative time, estimated blood loss, intraoperative and postoperative complications, length of hospital stay), and pathologic data were collected for both groups.
Surgical technique
The techniques for OPN and LPN have been described previously. 9 OPN was most often performed retroperitoneally using either a 12th rib-tip or transcostal approach with resection of the 12th rib. In cases involving upper pole tumors, the 11th rib was resected instead. For transperitoneal LPN, a four-port approach was used for left-sided tumors, and a five-port approach was used for right-sided tumors. For retroperitoneal LPN, only four ports were used.
Volume measurements
To objectively measure changes in abdominal muscle volume within each group before and after surgery, we used the Oncocare software (Siemens AG, Erlangen, Germany). All measurements from CT scan films (3–5 mm slice thickness) were performed with the observer being blinded to the side and type of surgery (open or laparoscopic). The abdominal wall was reconstructed in three dimensions for each patient, preoperatively and postoperatively. Right and left sides were measured separately (Fig. 1).
Three-dimensional reconstruction of the abdominal wall, preoperative and postoperative.
To ensure the volume change that may occur is not from global, entire body changes, the treated, surgical side was measured and compared with the contralateral, untreated side. To standardize the measurements, the CT scan slices were selected between the lower border of the 12th rib and the upper edge of the iliac crest. The muscles selected for volume calculation were: External oblique, internal oblique, transversus abdominis, and rectus abdominis. To provide three-dimentional (3D) volume data, the software requires a selection of the targeted tissue. To exclusively select the muscle, a short range of density corresponding to the muscle density was chosen. If any other organ or tissue was accidentally selected, we used the punching tool to remove it from the final 3D reconstruction. Muscle volume was measured in cubic centimeters.
In addition, to objectively assess the presence and extent of a flank bulge, we used a coronal view of the abdomen, and measured the distance between the line joining the lowest rib and the highest point of the iliac crest and the distance to the outer edge of the external oblique muscle (Fig. 2). The observer also reviewed each CT scan for the presence of a hernia, which was defined as a discrete defect (not just attenuation) in the musculofascial layers of the flank.

Measurement of the abdominal bulge.
Categoric distributions are reported as counts (percentages), and continuous variables are reported as medians and ranges. The nonparametric Wilcoxon test was used to assess differences in distributions among variables. Statistical analysis was performed using IBM SPSS statistics 19.0 (IBM Corp., Armonk, NY).
Interobserver variability in CT-measured parameters among three investigators (SC, KK, and GH) was assessed using the initial 21 patients. None of the observers were aware of the side of surgery or the operative approach. Interobserver difference (investigator 1-investigator 2), (investigator 1-investigator 3), and (investigator 2-investigator 3) was plotted against the mean of the three investigators. Coefficient of variation ([standard deviation of the differences/the mean]×100) was calculated for each parameter to allow comparison of the degree of variability of different parameters. A two-way mixed model was assessed for calculating the overall intraclass correlation coefficients for the three observers. This confirmed the interobserver reproducibility between the three observers (Table 1).
CT=computed tomography; SD=standard deviation; CV=coefficients of variation; ICC=intraclass coefficient; preop=preoperative; postop=postoperative.
All patients were administered a phone questionnaire 6 months or more postoperatively to assess recovery from surgery (Appendix 1; Supplementary Data are available online at
An additional cohort of 12 patients who underwent OPN on one side and LPN on the contralateral side was also evaluated. For the majority of these patients, only the postoperative CT scan was available. Both sides were objectively compared based on the muscle volume and bulge. This group of patients allowed for a direct comparison of the different surgical techniques on the same patient.
Results
Demographics and outcomes data are summarized in Table 2 for the OPN and LPN groups. Median age (range) was 59.9 years (20.6–80.7) in the OPN group and 57.5 years (25–78) years in the LPN group. Median BMI and ASA score were similar between the two groups (P=0.44 and P=0.43, respectively). The percentage of male participants in the OPN and LPN groups was 66% vs 62%, respectively (P=0.68). No significant difference was found between the two groups regarding comorbidities and Charlson Comorbidity Index. Of the 50 patients in the OPN group, 44 (88%) underwent a flank incision, of which 32 (73%) underwent rib resection. Of the 50 patients in the LPN group, 47 (94%) underwent a transperitoneal approach, and 3 underwent retroperitoneal LPN. All cases were completed successfully without any perioperative complications and without the use of any blood transfusions. The median percent variation in abdominal wall muscle volume (range) was significantly greater in the OPN group: −1.03% (−31.4–1.5) vs−0.39% (−5.2–1.8) (P=0.006). The median extent of the flank bulge on CT (range) was also greater in the OPN group 0.75 cm (−1.9–7.6) vs 0 cm (−2.7–2.8) (P=0.0004). Symptomatically, the OPN group experienced more paresthesiae 48% vs 8% (P=0.0053); numbness 44% vs 0% (P=0.002); and flank bulge 57% vs 12% (P=0.007).
BMI=body mass index; ASA=American Society of Anesthesiologists; CT=computed tomography.
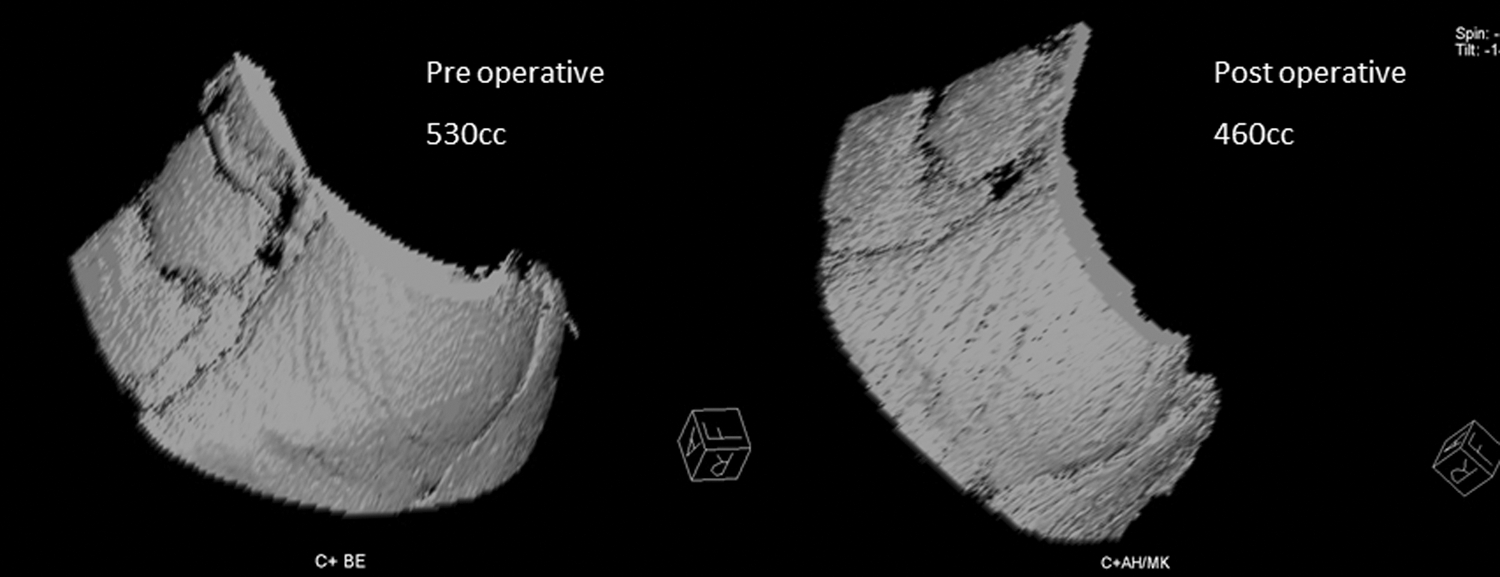
Table 3 summarizes demographics and outcomes of the 12 patients who underwent OPN on one side and LPN on the contralateral side. Median age (range) was 58.2 years in this group (range 48–75) and median BMI and ASA score was 28.6 kg/m2 (range 22.2–35.7) and 2.5 (2–3), respectively. A statistically significant trend was found toward greater flank muscle volume loss on the OPN side than the LPN side: 450 cc (190–713.5) vs 508.3 cc (208.6–808), respectively (P=0.043) (Figs. 3 –5). The OPN side was also found to have a greater flank bulge as well: 4 cm (1.2–6.6) vs 2.7 cm (0.5–4.3), respectively (P=0.003).

Abdominal muscle volume in patients who underwent open partial nephrectomy on one side and laparoscopic partial nephrectomy on the other side.

Postoperative three-dimensional reconstruction of the abdominal wall after an open partial nephrectomy on the right side and a laparoscopic partial nephrectomy on the left side 12.7 months after the procedure showing a bulge on the open side.

Postoperative three-dimensional reconstruction of the abdominal wall after an open partial nephrectomy on the left side and a laparoscopic partial nephrectomy on the right side 9.7 months after the procedure showing a hernia on the open side.
CT=computed tomography.
Discussion
The majority of renal tumors diagnosed today are T1 lesions, with many of these being amenable to nephron-sparing surgery. Multiple studies have demonstrated similar oncologic 6,7 and functional 10 outcomes for minimally invasive and open approaches to partial nephrectomy. Laparoscopic surgery additionally offers the potential for improved cosmesis and decreased wound-related morbidity, particularly with regard to incisional paresthesia, numbness, pain, flank bulge, and herniation. To our knowledge, there are limited data within the literature depicting a detailed comparison of OPN and LPN in these domains. Hence, we sought to quantify the relative impact of the laparoscopic vs open approach on these wound-related factors.
In our analysis of 100 consecutive patients with partial nephrectomy, we found that the patients undergoing LPN demonstrated a statistically significant advantage in hernia rate, preservation of abdominal wall muscle volume, and radiographic extent of flank bulge. Although small by objective measures, these differences translated into a substantial symptomatic advantage in patient-reported rates of flank bulge. Only 12% of the LPN patients noted a bulge; by contrast, 57% of OPN patients reported a permanent flank bulge, which is similar to the literature quoted rate of 49%. 8 A significantly greater proportion of OPN patients also reported temporary peri-incisional parathesiae and lasting peri-incisional numbness. No patient in either group complained of persistent pain or parathesiae. About a 25% rate of chronic peri-incisional pain after OPN, however, has been reported in the literature, suggesting a significant impact on quality of life. 8
Although there is a paucity of urologic literature addressing the long-term morbidity of the flank incision, the vascular surgery and neurosurgical literature provides intriguing insight into the etiology of flank bulge. The anatomic and physiologic basis for the flank bulge is a denervation injury resulting in irreversible muscle laxity and atrophy.
Motivated by patient dissatisfaction with the asymmetric cosmetic deformity created by flank bulge after spine surgery via an anterolateral retroperitoneal approach, Fahim and colleagues 11 performed a comprehensive cadaveric study and electrophysiologic investigation to explain the development of flank bulge. They determined that the 11th and 12th intercostal nerves are the predominant innervation to the anterolateral abdominal musculature. They defined three anatomic zones along the course of these nerves and proposed mechanisms for nerve injury during retroperitoneal surgery.
Zone 1 includes the portion of the nerves that travels in the intercostal groove. Injury in this zone might occur as a result of rib resection or re-approximation with large sutures. Zone 2 includes the segment of the 11th intercostal nerve traveling along the distal-most part of the 11th rib and the segment of the 12th intercostal nerve just beyond the tip of the 12th rib. Thus, an incision involving the region off the tip of the 12th rib might cause nerve injury. This is relevant for both the subcostal and 12th transcostal approach to OPN. Finally, zone 3 encompasses the segment of the nerves curving anteroinferiorly around the abdominal wall. Injuries in this zone result from direct transection or indirect thermal damage from electrocautery, as might occur during medial extension of the OPN incision or during extension of a trocar site to extract a specimen after LPN.
A longer flank incision and higher BMI have been implicated for increased risk of incisional bulge. 12 Based on the aforementioned anatomic and electrophysiologic studies, however, it appears that incisional length is only relevant insofar as how much of the incision traverses the nerve zones. In patients with a higher BMI, the incision is more likely to be extended anteriorly for improved exposure, thereby possibly increasing the risk of nerve injury.
Several studies have looked at morbidity after an open incision for kidney surgery. Kumar and associates 13 compared the outcomes between the use of a thoracoabdominal vs a flank incision for radical nephrectomy. They found no statistically significant difference between either group in terms of incisional pain, analgesic requirements after discharge, and time to return to normal activities. This study demonstrated the effects of a different type of incision whereas we discussed the effects of different types of surgical procedure (open vs laparoscopic).
Another study done by Kumar and coworkers 14 sought to determine the short- and long-term outcomes of morbidity of flank incision for radical nephrectomy. This study found that open donor nephrectomy via a flank incision is safe via validated questionnaires. In our study, we sought to observe the changes in muscle volume after open vs laparoscopic techniques in addition to patient morbidity outcomes. Kobayashi and colleagues 15 in 2004 demonstrated the changes in body image using a 3D body surface laser scanner on 27 patients who underwent renal surgery. Their cohort consisted of patients who had a flank, laparoscopic, or transabdominal approach, as well as patients who underwent many different types of surgical procedures, ranging from radical nephrectomy to nephrolithotomy. The study found that the body surface area and volume of the operative side were significantly greater than those of the contralateral side. While this study is promising, a larger cohort is needed.
In our cohort, the majority of OPN patients underwent a transcostal approach with 12th rib resection, while the majority of LPN patients underwent a transperitoneal approach. Thus, one would expect a larger proportion of OPN patients to sustain intercostal nerve injury and have greater incisional morbidity, as confirmed by our data. Occurrence of flank bulge and hernia in a small number of LPN patients can be explained by probable nerve injury during specimen extraction and/or incision closure. Nonetheless, as expected, incisional morbidity is clearly reduced with the laparoscopic approach. Further decreasing the incisional morbidity after LPN may be achieved by respecting the zones of potential nerve injury during extraction and closure.
Our study is not without limitations. The software used for this study, specifically Oncocare, is not readily available to everyone and needs a steep learning curve for use. In addition, the response to our phone questionnaire was low (40%). As a tertiary referral center, many of the patients included in this study came from different states and even countries. Follow-up on them was difficult and is a limitation to this study. While we found no statistically significant difference in median percent change in the abdominal muscle volume between the responders and nonresponders, −4.38% vs−4.76% (P=0.67), respectively, more follow-up in a larger cohort is needed to further validate our findings.
Conclusions
The laparoscopic approach to partial nephrectomy is associated with decreased rates of flank hernia and objective and subjective flank bulge compared with the open approach. Flank incision morbidity is fundamentally a denervation problem. It is important to discuss this potential complication with every patient when discussing OPN.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.