
Abstract
Background and Purpose:
Over the past 50 years, there has been an upward shift in the age of peak incidence of stone disease, yet less is known regarding how the urinary biochemical profile changes with aging. Therefore, we sought to examine the relationship between age and 24-hour urine composition.
Methods:
We retrospectively reviewed a database of our tertiary care stone clinic patients seen from March 2002 to February 2012. Analysis of pretreatment 24-hour urine collections across age groups was performed using univariate analysis of variance and multivariate linear regression models adjusting for clinical and demographic factors and 24-hour urine parameters.
Results:
A total of 1115 patients were broken down into age groups consisting of <45 years (221; 19.7%), 45–54.9 years (270; 23.8%), 55–64.9 years (270; 24.6%), and ≥65 years (356; 31.9%). Univariate analysis found significant ascending trends with aging for mean body mass index, while mean urine pH, 24-hour calcium, uric acid (UA), ammonium, creatinine, and supersaturation (SS) of calcium oxalate (CaOx) and calcium phosphate (CaP) decreased with age (all P for trend <0.05). Adjusted multivariate analysis demonstrated that increased age was significantly associated with increased 24-hour citrate and SS UA, whereas increased age was significantly associated with decreased pH, 24-hour UA, creatinine, SS CaOx, and SS CaP (all P for trend <0.05).
Conclusions:
There are numerous age-related changes in the metabolic profile as seen on 24-hour urine collection. This highlights the importance of evaluating stone-forming patients of all ages with 24-hour urine collections because both the type and degree of metabolic abnormality may change with age.
Introduction
R
These studies have helped improve our understanding of the effect of age on nephrolithiasis, yet much remains to be described regarding changes in metabolic characteristics and stone risk profile as patients age. With this as a background, we sought to examine the relationship between age and 24-hour urine composition in stone-forming patients.
Methods
Study population
After obtaining Institutional Board Review approval, data from adult stone-forming patients, 18 years old or older, who had undergone 24-hour urinalysis at our institution between March 2002 and February 2012, were combined into the study database. Patients were under the care of endourologists (ADS and ZO) whose practice is dedicated to treatment of patients with stone disease. The database includes information on patient age, sex, height, weight, body mass index (BMI) comorbidities (including diabetes mellitus [DM], hypertension [HTN], and hypercholesterolemia), the presence of urinary diversion, current medications (including allopurinol, potassium citrate, and thiazides), and stone composition (including calcium oxalate [CaOx] monohydrate, CaOx dihydrate, uric acid [UA], brushite, ammonium urate, struvite, calcium carbonate, and apatite). The database also contains data on 24-hour urinalysis including urinary pH, volume, calcium, oxalate, citrate, UA, sodium, potassium, magnesium, phosphate, sulfate, creatinine, supersaturation (SS) CaOx, SS calcium phosphate (CaP) and SS UA. Only subjects with adequate 24-hour urine collections (defined by 24-hour creatinine excretion ≥600 mg for females and 800 mg for males) were included in the study.
We included only a single 24-hour urine collection for analysis. In those patients who gave more than one 24-hour sample, only the first urinalysis was used. After a review of the electronic medical records, 1115 patients had complete data and were included in the study. Data were collected as of the time of initial metabolic stone evaluation, before treatment at our institution. Twenty-four hour urinalyses were processed by Litholink
Statistical analysis
Patients were divided in four age groups: <45, 45–54.9, 55–64.9 and ≥65 years old. Comparisons of baseline characteristics (including age, sex, and BMI) between age groups were performed using the Fisher exact test for categorical data and analysis of variance (ANOVA) for continuous variables. Univariate analysis of the differences in 24-hour urine composition (including pH, volume, calcium, oxalate, citrate, UA, sodium, potassium, magnesium, phosphate, sulfate, creatinine, SS CaOx, SS CaP, and SS UA concentrations) between age groups was performed using ANOVA. Multivariate comparisons of 24-hour urine composition between age groups of stone formers were performed using linear regression. The multivariate analyses were adjusted for clinical and demographic factors (age, gender, BMI, DM, HTN, urinary diversion, and medication use including allopurinol, potassium citrate, and thiazides) and 24-hour urine components (including volume, pH, calcium, citrate, etc).
Two multivariate models were created: The first including age as a categorical variable and the second using age as a continuous variable. The assumptions of linearity of the relationship between the dependent variable and covariates, independence of the errors, homoscedasticity of the errors and normality of the error distribution were verified for all models. For patient with stone composition data available (n=436), we also analyzed the changes in percent stone composition across age groups, including CaOx monohydrate, CaOx dehydrate, UA, struvite, brushite, apatite, calcium carbonate, and ammonium urate. The trends in percent stone composition changes across age groups were tested using linear regression. All statistical analyses were two-tailed and performed using R 2.15.1 (R Foundation for Statistical Computing, Vienna, Austria). A P<0.05 was considered to indicate statistical significance.
Results
Of the 1115 patients in the study database, the age group breakdowns were <45 years (221; 19.7%), 45–54.9 years (270; 23.8%), 55–64.9 years (270; 24.6%), and ≥65 years (356; 31.9%). There were 630 (57%) males and 485 (43%) females in the cohort. A significant difference across groups was seen with mean BMI (27.5±6.3, 30.4±8.0, 30.1±7.1, 29.5±6.1, P<0.001). The number of stone formers with DM and HTN was also significantly different across groups, with greater percentages with increasing age group (DM: 13 [6%], 33 [13%], 50 [18%], 85 [24%], P<0.001; HTN: 28 [13%], 79 [31%], 122 [44%], 214 [59%], P<0.001), where older patients were more likely to have DM and/or HTN. The only other demographic difference at baseline was the number of patients receiving potassium citrate, with greater percentages with increasing age group (P=0.009). No significant differences were seen in thiazide use, allopurinol use, or the presence of a urinary diversion. Demographic data can be seen in Table 1.
Fisher exact test for categorical variables and analysis of variance for continuous variables.
SD=standard deviation.
Univariate analysis of 24-hour urine parameters can be seen in Table 2. We found significant ascending trends with aging for mean BMI, potassium, and urine volume, while mean pH, calcium, UA, phosphate, creatinine, protein catabolic rate, SS CaOx, and SS CaP decreased with age (all P for trend <0.05).
All values are displayed as mean (±standard deviation).
SS=supersaturated; CaOx=calcium oxalate; CaP=calcium phosphate; UA=uric acid.
Multivariate analysis was adjusted for age, sex, BMI, comorbidities, medication use, urinary diversion, and 24-hour urine parameters. The results broken down by age group demonstrated that increased age was significantly associated with increased 24-hour citrate, potassium, sulfate, phosphate, and SS UA, whereas increased age was significantly associated with decreased pH, 24-hour UA, creatinine, SS CaOx, and SS CaP (all P for trend <0.05). These results can be seen in Table 3.
All differences are referent to group <45 years.
SS=supersaturation; CaOx=calcium oxalate; CaP=calcium phosphate; UA=uric acid.
When the multivariate adjusted analysis was performed for age as a continuous variable, these same significant associations remained: Each additional year of age was associated with increased citrate (difference [d]=1.97 mg, P<0.001), potassium (d=0.26 mEq, P<0.001), sulfate (d=0.11 mmol, P<0.001), phosphate (d=0.001 g, P<0.026), SS UA (d=0.005, P=0.01), whereas each additional year of age was associated with decreased pH (d=−0.006, P<0.001), UA (d=−0.009, P=0.024), SS CaOx (d=−0.02, P=0.002), and SS CaP (d=−0.012, P<0.001). There was no significant association between age and 24-hour calcium, oxalate, sodium, magnesium, or urine volume (Table 4).
Difference is change in value for each unit increase in age (1 year).
CaOx=calcium oxalate; CaP=calcium phosphate; SS=supersaturation; UA=uric acid.
Four hundred thirty-six stones composition analyses were present in the database. Univariate analysis of stone composition according to age found an increasing percentage of UA content with increasing age (<45 years [6.55%], 45–54.9 [13.69%], 55–64.9 [28.03%], 85 [30.78%], P for trend <0.001), while the percentage of CaOx dihydrate (<45 years [15.41%], 45–54.9 [10.72%], 55–64.9 [6.35%], 85 [4.23%], P for trend <0.001) and apatite decreased with increasing age (<45 years [30.31%], 45–54.9 [20.99%], 55–64.9 [11.43%], 85 [16.42%], P for trend <0.001). No significant trends were seen for CaOx monohydrate, brushite, ammonium urate, struvite, and calcium carbonate (Fig. 1).
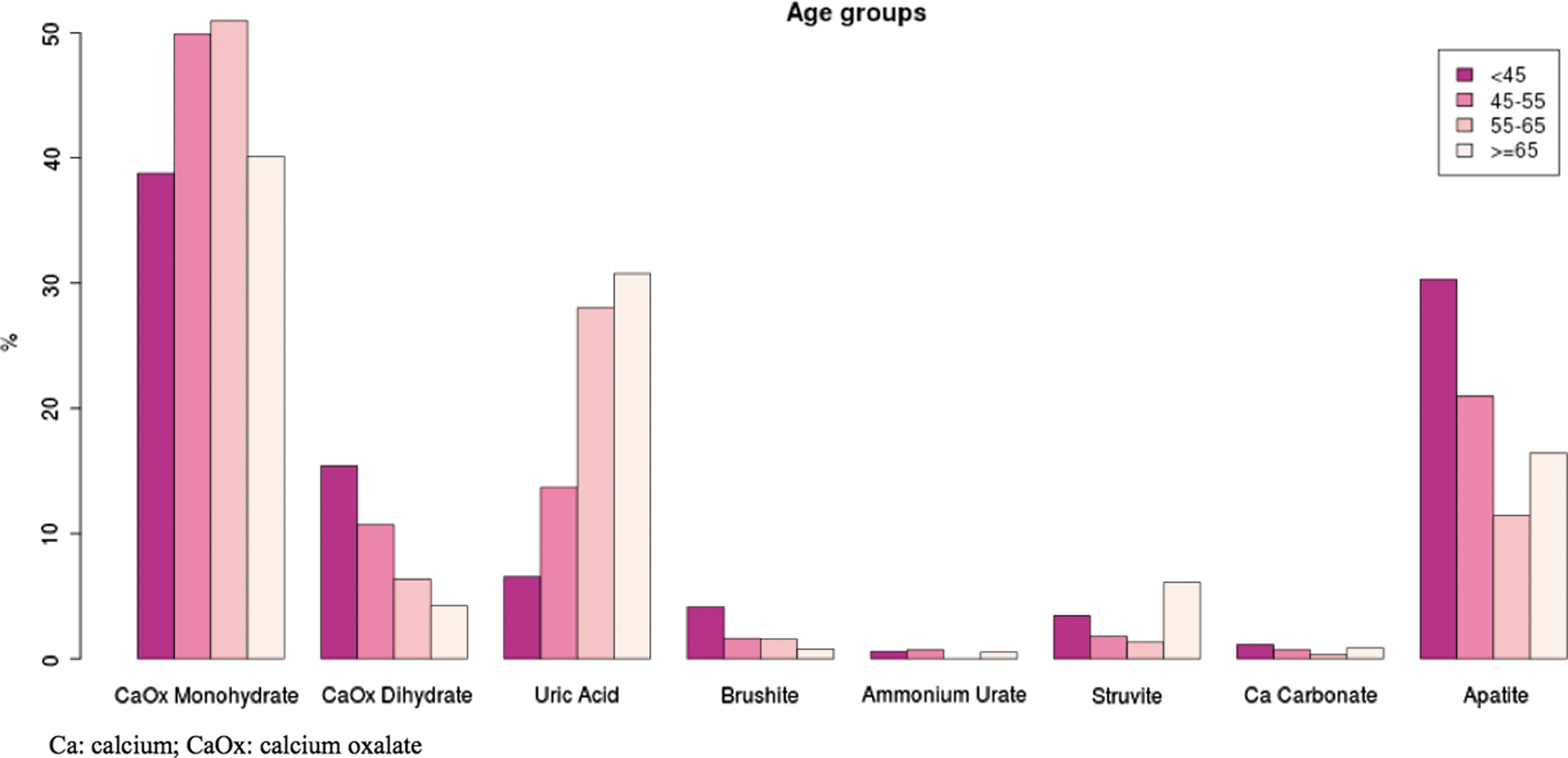
Stone composition percentage according to age group.
Discussion
The rise in incidence and prevalence of nephrolithiasis has generated studies investigating the association of commonly found disease entities with stone disease. Thanks to this work, there now exists well-established associations between DM, 5,6 HTN, 7 –11 and BMI, 12,13 and nephrolithiasis. With regard to stone disease and age-related effects, much of the adult stone literature has been large general population epidemiologic studies. Less data are available on specific age-related differences in metabolic factors that may affect the management and prevention of stone disease with aging.
Early work on the effects of age on stone formation was conducted by Goldfarb and associates. 2 The authors evaluated pre- and post-treatment 24-hour urine samples in stone forming patients over a 24-year period. In comparing pretreatment values for men and women more than 60 years old (277) and <60 years old (2100), they found significantly lower 24-hour calcium and uric acid, lower urinary pH, and lower SS CaOx and SS CaP for older compared with younger patients. They speculated that there might be a need to manage more modest urinary calcium and SS values in older patients.
Krambeck and colleagues 3 recently studied age differences in the clinical presentation and management of incident stone disease in Olmstead County in Minnesota. Review of their database uncovered a number of interesting findings. Specifically for stone composition, CaP stones were significantly associated with younger age, while UA and atypical stones were associated with older age (both P<0.001). Our study demonstrated a similar trend, as did Kadlec and coworkers, 14 who found an inverse correlation between UA content and estimated glomerular filtration rate (eGFR), as well as a direct correlation between CaP content and eGFR (both p<0.001).
In our large study of stone-forming patients, our analysis demonstrated significant trends with associated with aging. Consistent with the findings of Goldfarb and associates 2 was our finding that urinary calcium decreases with age. This trend was significant on univariate analysis, and while not statistically significant on multivariate analysis, the trend still held and should certainly be considered clinically relevant. We hypothesize that this decline in urinary calcium with age is from age-related changes in calcium handling, either because of intestinal absorption, or renal mechanisms, or a combination of both. The relationship to renal mechanisms is supported by a study by Gershman and colleagues, 15 who compared 24-hour urine composition by GFR quintile. Multivariate analysis showed that decreasing GFR was associated with significant decreases in 24-hour urinary calcium.
We demonstrated, as did Goldfarb and associates, 2 significant decreasing SS CaOx and SS CaP with increasing age, which held its significance on multivariate adjusted analysis. This is likely driven by the decline in urinary calcium, because our results demonstrate that oxalate and phosphate both increase with age. When taken in the context of increasing incidence of stone disease and a change in the age of peak incidence of stones, our findings give credence to the idea that lower SS values in older stone-forming patients are likely sufficient to increase the risk of stone formation, and normal ranges may need to be age-adjusted to more appropriately counsel and treat patients. 2 It also suggests that clinicians consider more aggressive treatment of lesser levels of urinary calcium in older patients to prevent stone recurrence. A reason for these findings may be the possibility of changes with age in levels of urinary inhibitors of calcium stone crystallization, which would alter the stone risk profile for calcium stone formers. Decreased renal function may also play a role. 15 These mechanisms need further investigation.
Previously, studies have shown contradictory results for citrate excretion, with some finding decreased excretion with age, 16 while others showed increases in urinary citrate with age. 17,18 Given that our study is the largest to date evaluating stone metabolic assessment in relation to age, we feel that it tips the scales in favor of rising urinary citrate with age in stone-forming patients.
Our analysis also demonstrated age-related decline in urine pH. While our study and others 2,3 have identified this decline in pH with age, we saw this in the face of rising 24-hour urine citrate, and, in fact, none of the mean levels of 24-hour citrate even qualified as hypocitraturia (<320 mg/day). 19 It could well be that the decline in pH is because of kidney aging. Classic work by Homer Smith 20 then Davies and Shock 21 demonstrated a decline in GFR with aging is thought to start between 30 and 40 years. This has been supported by a longitudinal study of normal male subjects showing a 31% decline in GFR from age 30 to 80 years 22 and cross-sectional studies of living donors of kidney allografts that consistently demonstrate a progressive decline in GFR with age, even with the exclusion of donors with chronic kidney disease and its risk factors. 23 –25
To determine the effect of renal function on urinary mineral stone excretion and stone composition, Kadlec and coworkers 14 stratified 158 patients by eGFR (calculated by preoperative Modification of Diet in Renal Disease equation) and found that urine pH on 24-hour urinalysis was significantly lower for patients in the lower eGFR group (>90 mL/h: 6.25±0.62 vs 60–89 mL/h: 6.16±0.50 vs 30–59 mL/h: 5.73±0.63; P<0.01). 14 The study by Gershman and colleagues 15 also demonstrated a trend of declining pH with decreasing GFR, however, it was not statistically significant. This suggests that age-based physiologic decline in renal function may be one of the forces behind lower urinary pH seen with aging.
Another important effector of pH is BMI, with multiple studies having demonstrated that higher BMI is associated with decreased pH. 12,13,26 Our study found that increased age was significantly associated with increased BMI, so it is likely that higher BMI, likely in the context of metabolic syndrome, in older patients also contributes to decreased pH, and highlights a need for weight control as part of overall medical management. Thus, the rise seen in urinary citrate may be the body's attempt to compensate for decreased urinary pH, especially because ammonium excretion, one of the important urinary acid buffers, was found to decrease with age. This is in line with the idea that low urine pH in advancing stages of chronic kidney disease is because of impairment in ammoniagenesis, which results in metabolic acidosis. 27 It appears that aggressive measures to correct pH may be needed in older patients to prevent stone recurrence.
Our study has inherent limitations. First, it is a retrospective study. Also, our study reflects patients in a specific geographic region treated at a tertiary referral center, two factors that may limit the external generalizability of our results. We did not have data on race or ethnicity because it was not available for all patients, nor did we have data on symptomatic vs asymptomatic presentation or number of stone recurrences for the same reason; thus, the results may not be applicable to all patient populations. Our database was also limited to specific demographics, and absence of other variables such as diet, lifestyle, and other comorbidities and medications may have led to different results. Last, these data reflect stone-forming patients and may not be relevant to non–stone-forming patients. Despite these factors, this is a large, contemporary cohort and one of the few available studies on age not restricted to only a pediatric or geriatric population.
Conclusions
We found numerous age-related changes in stone biochemical profile that highlight the importance of evaluating stone-forming patients of all ages with 24-hour urine collections. Increasing age was significantly associated with decreasing urinary pH. This occurred in the face of a rise in BMI and urinary citrate and fall in ammonium. This suggests that alkalinization therapy in combination with dietary limitation and medical therapy to combat uric acid production may be necessary to prevent stone recurrence for older patients, along with weight control strategies. With increasing age, we identified a decline in urinary calcium and accordingly lower SS CaOx. It is possible that lower SS CaOx values in older patients are sufficient for stone formation; however, additional prospective studies evaluating stone recurrence are needed before this conclusion can be drawn.
Footnotes
Disclosure Statement
No competing financial interests exist.