
Abstract
Introduction:
The role of surgical approach on functional outcomes recovery in prostate cancer (PCa) patients treated with bilateral nerve-sparing radical prostatectomy (BNSRP) is still debated. In this study, we examine the association between the surgical approach and functional outcomes after BNSRP.
Patients and Methods:
The study included 609 patients treated with robot-assisted radical prostatectomy (RARP) or open radical prostatectomy (ORP) between June 2008 and January 2011. Erectile function recovery was defined as an International Index of Erectile Function-Erectile Function domain (IIEF-EF) score ≥22. Urinary continence recovery was defined as being completely pad-free over a 24-hour period. Patients were stratified according to their probability of postoperative erectile dysfunction and urinary incontinence, according to previously published predictive models. Multivariable logistic regression tested the association between the surgical approach and functional outcomes recovery in the overall population after stratifying patients according to their risk of erectile dysfunction and urinary incontinence.
Results:
Patients treated with RARP had higher 2-year erectile function (52.1% vs 67.8%; P<0.001) and urinary continence (72.0% vs 87.4%; P<0.001) recovery rates as compared to their ORP counterparts. After stratification according to the erectile dysfunction risk, RARP led to higher erectile function recovery rates in the low- and intermediate-risk erectile dysfunction groups (all P<0.001).This did not hold true, however, in patients at high risk of erectile dysfunction (P=0.5). Similarly, when patients were stratified according to their urinary incontinence risk, RARP was associated with a higher probability of urinary continence recovery in the very low, low, and intermediate risk groups only (all P<0.001). This did not hold true, however, in the group of men at high risk of postoperative urinary incontinence (P=0.8).
Conclusions:
RARP leads to higher urinary continence and erectile function recovery rates compared with ORP. Not all patients benefit from this approach to the same extent, however. Accurate preoperative patient selection would result in substantial savings for the health care system.
Introduction
P
After the introduction of minimally invasive approaches, such as robot-assisted radical prostatectomy (RARP), many authors from referral centers reported better functional outcomes after RARP as compared with open radical prostatectomy (ORP). 4 –8 On the contrary, large population-based studies failed to show an association between the surgical technique and improved long-term functional outcomes. 9,10 None of these retrospective studies, however, compared the outcomes of the two approaches according to preoperative characteristics, such as age at surgery, comorbidity status, and preoperative functional status, which represent key determinants of postoperative functional outcome. 11 –13 Identifying the best candidate for minimally invasive approaches would be important for two main reasons: 1) optimizing economic resource for heath care systems, given the higher costs of RARP as compared with standard ORP, and 2) accurate patient counseling.
To address this void, our study was aimed at reassessing the association between the surgical approach (RARP vs ORP) and functional outcomes recovery in patients treated with bilateral nerve-sparing radical prostatectomy (BNSRP). Particularly, we hypothesized that the extent of the benefit related to the adoption of minimally invasive surgery might depend on preoperative patient characteristics. We evaluated the impact of RARP on erectile function and urinary continence recovery in the overall population after stratifying patients according to their preoperative risk of erectile dysfunction and urinary incontinence. 12,13
Patients and Methods
Study population and surgical technique
The current study evaluated prospectively collected data from 609 patients with clinically localized PCa treated with BNSRP at a single tertiary referral center between June 2008 and January 2011. All patients included in the study had complete preoperative, pathologic, and follow-up data. All men were treated with either open or robotic BNSRP with or without pelvic lymph node dissection by five surgeons. The nerve-sparing surgical technique has been previously described. 14 –16 The indication for bilateral neurovascular bundle preservation was based on the clinical judgment of each treating physician, regardless of preoperative erectile status. It was strongly recommended that all patients attempt sexual intercourse as soon as possible after catheter removal, and all patients were offered phosphodiesterase type 5 inhibitors to encourage the recovery of erectile function. No patient received adjuvant therapies after BNSRP.
Covariates
For each patient, age at surgery, body mass index (BMI), clinical stage, preoperative prostate-specific antigen levels, biopsy Gleason score, surgical approach, pathologic stage, pathologic Gleason score, nodal invasion, surgical margin status, and the Charlson comorbidity index (CCI) were assigned. All patients included in the study were preoperatively fully continent (defined as no pad use). Preoperative erectile function was assessed using the erectile function domain of the International Index of Erectile Function (IIEF-EF).
Patients were stratified according to their probability of postoperative erectile dysfunction and urinary incontinence based on two published classifications. 13,14 For erectile function assessment, patients stratification was as follows: low (age ≤65, IIEF-EF ≥26, and CCI ≤1), intermediate (age 66–69 or IIEF-EF 11–25 and CCI ≤1), and high (age ≥70 or IIEF-EF ≤10 or CCI ≥2) risk of postoperative erectile dysfunction, as previously reported. 13 For urinary continence evaluation, stratification consisted of four risk groups of urinary incontinence: very low (IIEF-EF >10, age <65, and BMI <25), low (IIEF-EF >10, age <65, and BMI ≥25), intermediate (IIEF-EF >10 and age ≥65), and high (IIEF-EF 1–10) risk of postoperative urinary incontinence, as previously published. 12
Follow-up and end points
Patients were evaluated every 3 months during postoperative year 1 and every 6 months thereafter. Postoperative urinary continence was assessed by patient-reported 24-hour pad use. Postoperative urinary continence was defined as no pad use over a 24-hour period. Postoperative erectile function was assessed using the IIEF-EF, which was completed during each visit. Postoperative erectile function was defined as an IIEF-EF ≥22. 17
Statistical analyses
Means, medians, and interquartile ranges were reported for continuous variables. Frequencies and proportions were reported for categorical variables.
Our statistical approach consisted of two steps. First, Kaplan-Meier curves assessed the impact of the surgical technique on erectile function and urinary continence recovery in the overall population after stratifying patients according to previously validated risk groups for postoperative erectile dysfunction and urinary incontinence. 12,13 Second, multivariable Cox regression analyses evaluated the association between the surgical technique and functional outcome recovery in the overall population after accounting for age at surgery, year of surgery, CCI, preoperative IIEF-EF domain, and D'Amico risk group. 18 Similarly, the association between type of surgery was assessed separately in each risk group after accounting for year of surgery and D'Amico risk group.
All statistical analyses were performed using the R statistical package system version 3.0.2 (R Foundation for Statistical Computing, Vienna, Austria) and SPSS version 21 (IBM, Chicago, IL). All tests were two sided with a significance level set at 0.05.
Results
Baseline characteristics
Table 1 depicts the baseline characteristics of patients included in the study. Mean (median) age at BNSRP was 61.2 (61) years. Overall, 294 (48.3%) and 315 (51.7%) patients were treated with ORP and RARP, respectively. When patients were stratified according to the surgical approach, statistically significant differences were observed with regard to year of surgery, preoperative IIEF-EF, erectile dysfunction risk group, urinary incontinence risk group, receipt of pelvic lymph node dissection, clinical stage, pathologic stage, and surgical margin status (all P≤0.02). Mean (median) follow-up was 35.2 (28) months. Overall, 340 (55.8%) and 477 (78.3%) patients recovered erectile function and urinary continence during follow-up, respectively.
BMI=body mass index; BNSRP=bilateral nerve-sparing radical prostatectomy; CCI=Charlson comorbidity index; ED=erectile dysfunction; IIEF-EF=International Index of Erectile Function-Erectile Function domain; IQR=interquartile range; ORP=open radical prostatectomy; PCa=prostate cancer; PLND=pelvic lymph node dissection; PSA=prostate-specific antigen; RARP=robot-assisted radical prostatectomy; UC=urinary incontinence.
Kaplan-Meier analyses
Overall, the 1- and 2-year erectile function recovery rates were 52.9% and 60.2%, respectively (Fig. 1A). The 2-year erectile function recovery rates were 82.3%, 58.0%, and 33.0% for patients included in the low, intermediate, and high erectile dysfunction risk groups (P<0.001; Fig. 1B). When patients were stratified according to the surgical technique, the 2-year erectile function recovery rates were 52.1% vs 67.8% for patients treated with ORP vs RARP, respectively (P<0.001; Fig. 2A). When considering patients included in the low and intermediate erectile dysfunction risk groups, individuals treated with RARP had significantly higher erectile function recovery rates compared to their counterparts treated with ORP (all P<0.001, Fig. 2BC). In the high erectile dysfunction risk group, however, no statistically significant differences were observed in the erectile function recovery rates between individuals treated with RARP and ORP (P=0.5, Fig. 2D).

Kaplan-Meier analyses depicting time to erectile function recovery
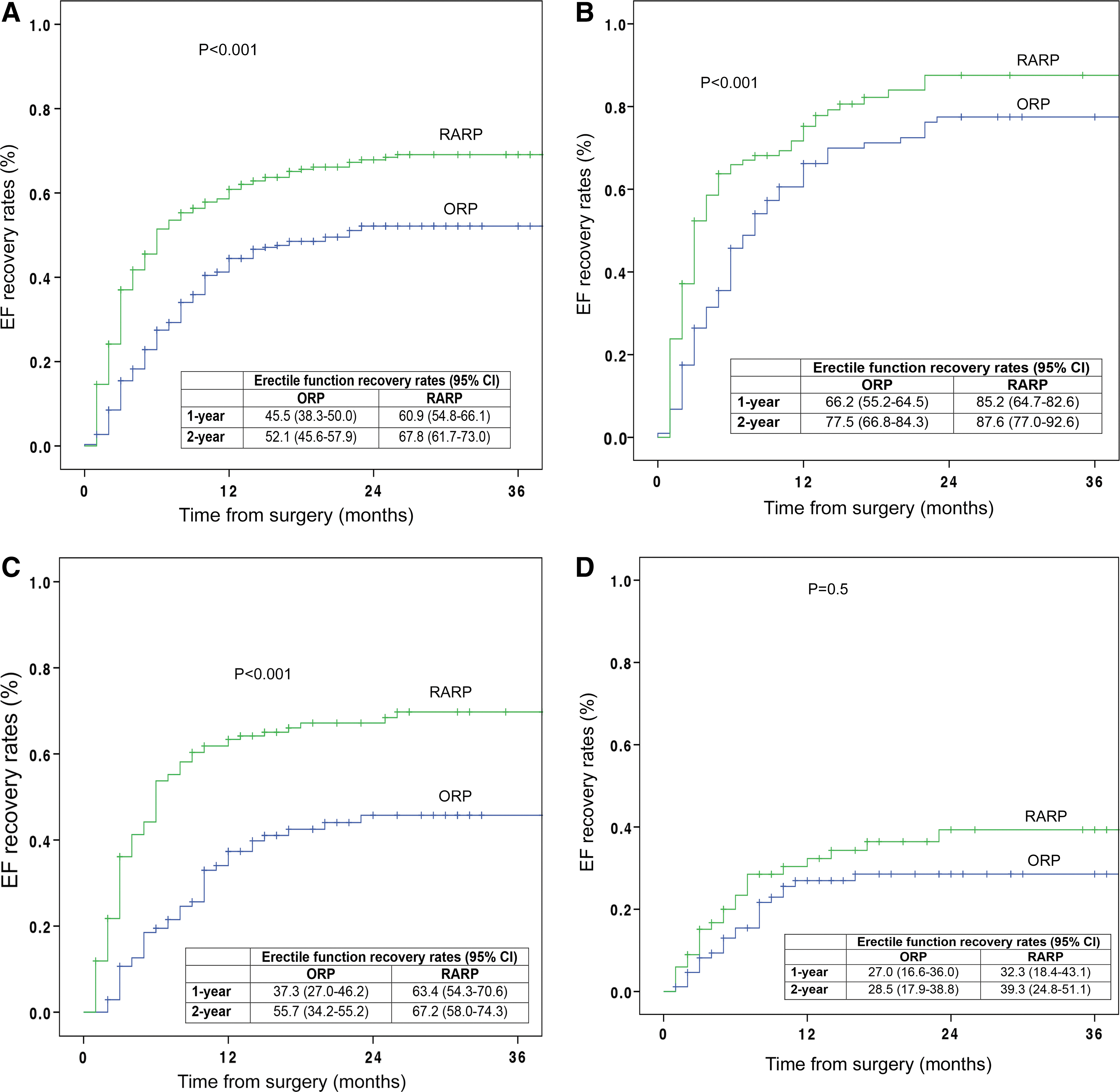
Kaplan-Meier analyses depicting time to erectile function recovery stratified according to the surgical approach (RARP vs ORP)
Overall, the 1- and 2-year urinary continence recovery rates were 76.0% and 80.2%, respectively (Fig. 3A). The 2-year urinary continence recovery rates were 84.4%, 87.4%, 74.1%, and 70.2% for patients included in the very low, low, intermediate, and high urinary incontinence risk groups (P<0.001; Fig. 3B). When patients were stratified according to the surgical technique, the 2-year urinary continence recovery rates were 72.5% vs 87.4% for patients treated with ORP vs RARP, respectively (P<0.001; Fig. 4A). When considering patients included in the very low, low, and intermediate urinary incontinence risk groups, individuals treated with RARP had significantly higher urinary continence recovery rates compared to their counterparts treated with ORP (all P<0.001, Fig. 4BCD). In the high urinary incontinence risk group, however, no statistically significant differences were observed in the erectile function recovery rates between individuals treated with RARP and ORP (P=0.8, Fig. 4E).
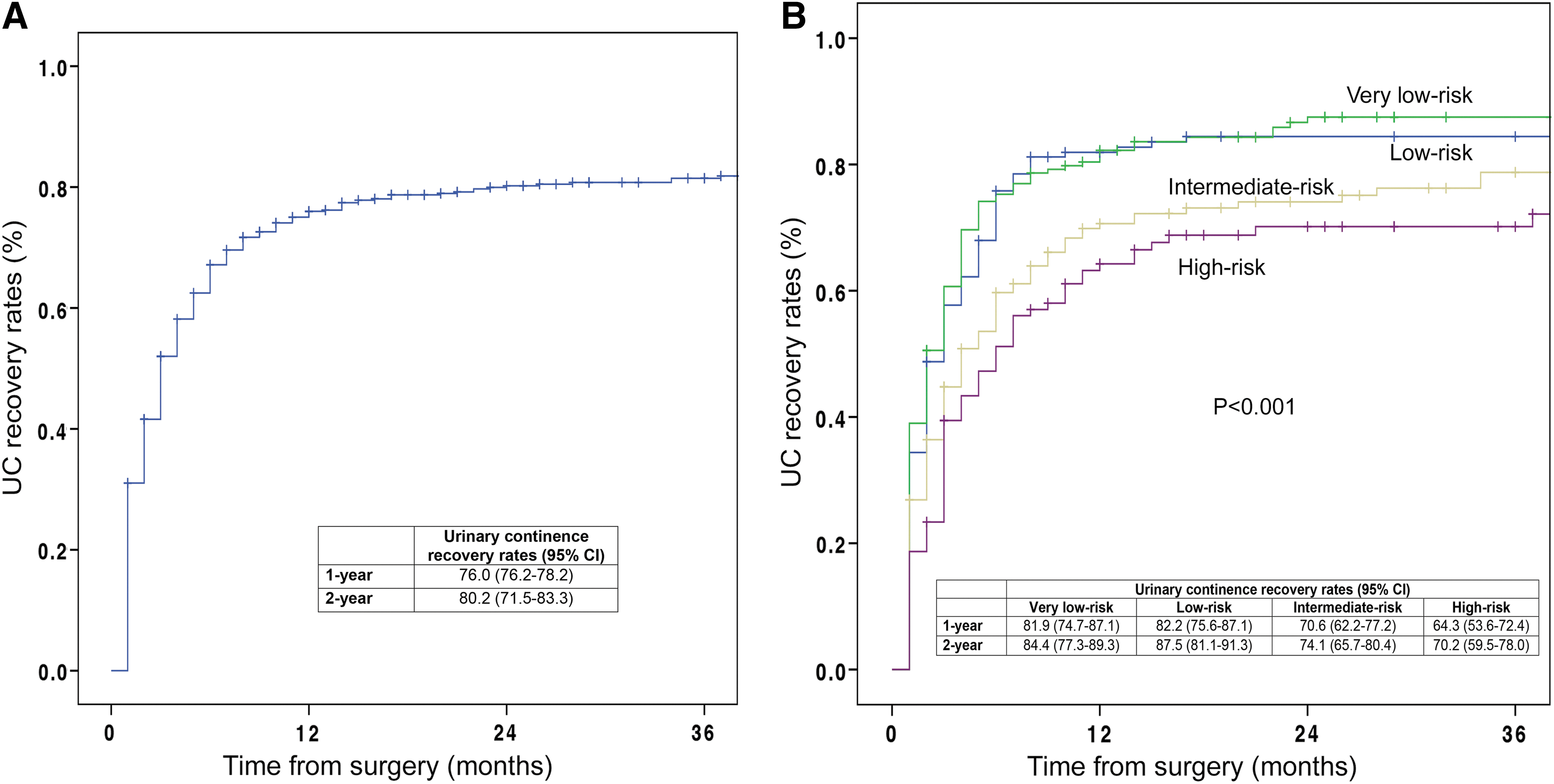
Kaplan-Meier analyses depicting time to urinary continence recovery

Kaplan-Meier analyses depicting time to urinary continence recovery stratified according to the surgical approach (RARP vs ORP)
Multivariable Cox regression analyses
In multivariable Cox regression analyses, patients treated with RARP had higher probability of recovering erectile function, after accounting for confounders (hazard ratio [HR] 1.73; 95% confidence interval [CI], 1.37–2.18; P<0.001; Table 2). This held true when considering patients in the low and intermediate erectile dysfunction risk groups (all P<0.001). When exclusively considering patients in the high erectile dysfunction risk group, however, the surgical approach was not associated with postoperative erectile function even after accounting for confounders (P=0.6). Similarly, patients treated with RARP had higher probability of recovering urinary continence after accounting for confounders (HR, 1.69; 95% CI, 1.36–2.11; P<0.001; Table 3). This held true when considering patients in the very low, low, and intermediate erectile dysfunction urinary incontinence risk groups (all P≤0.001). When considering exclusively patients in the high urinary incontinence risk group, however, the surgical approach was not associated with postoperative erectile function even after accounting for confounders (P=0.8).
Model adjusted for age at surgery, year of surgery, Charlson comorbidity index, preoperative International Index of Erectile Function, and D'Amico risk group.
Model adjusted for year of surgery and D'Amico risk group.
CI=confidence interval; HR=hazard ratio; ORP=open radical prostatectomy; RARP=robot-assisted radical prostatectomy.
Model adjusted for age at surgery, year of surgery, Charlson comorbidity index, preoperative International Index of Erectile Function, and D'Amico risk group.
Model adjusted for year of surgery and D'Amico risk group.
CI=confidence interval; HR=hazard ratio; ORP=open radical prostatectomy; RARP=robot-assisted radical prostatectomy.
Discussion
Although the introduction of RARP rapidly raised enthusiasm in the urologic community regarding the possibility of improved results in terms of perioperative morbidity and long-term functional recovery after surgery, 4,8,19 the advantages of the robotic approach over traditional open surgery are still a matter of debate. 9,10 This is particularly true when considering postoperative erectile function and urinary continence recovery. Indeed, while previous studies reporting the initial experience of high-volume centers showed that RARP might lead to higher erectile function and urinary continence recovery rates compared to open surgery, 4,8 the validity of these observations was questioned by the lack of association between minimally invasive surgery and better continence or sexual function recovery observed by large population-based studies. 9,10 Such a discrepancy might be related to differences in preoperative patient characteristics, as individuals included in population-based studies are typically older and sicker compared with their counterparts treated at high-volume referral centers. 20 These considerations further highlight the importance of baseline characteristics, such as age at surgery, comorbidity status, and preoperative erectile function and urinary continence, on functional outcomes after surgery regardless of the approach used. 11 –13 Under this light, we aimed at reassessing the impact of RARP on the recovery of erectile function and urinary continence in a large contemporary cohort of PCa patients treated with BNSRP. Particularly, we sought to evaluate the role of the surgical approach (ORP vs RARP) on functional outcomes according to the preoperative risk of erectile dysfunction and urinary incontinence. Specifically, patients were stratified according to previously validated risk groups assessing the risk of erectile dysfunction and urinary incontinence after surgery. 12,13,21
The results of our study are severalfold. First, we found that RARP was associated with higher erectile function and urinary continence recovery rates in the overall population. Particularly, patients treated with the minimally invasive approach had a 73% higher probability of recovering erectile function compared with their ORP counterparts, and RARP patients had a 69% higher probability of experiencing urinary continence recovery after surgery compared to patients treated with open surgery. These observations might reflect the technical advantages related to minimally invasive surgery. Particularly, reduced surgical stress, intuitive movements, less intraoperative bleeding, and optical magnification might allow a better preservation of the neurovascular bundles and a more accurate and gentle dissection, 22,23 which represent key steps for optimal functional preservation. 14 –16,24
Second, our investigation shows that the benefit of RARP on functional outcomes recovery substantially varies according to preoperative erectile dysfunction and urinary incontinence risk. Indeed, while minimally invasive surgery was associated with improved postoperative erectile function and urinary continence recovery in patients included in the low and intermediate risk groups, no statistically significant differences were observed between ORP and RARP when considering patients at high risk of erectile dysfunction and urinary incontinence. These results were confirmed in multivariable analyses, where the magnitude of the association between RARP and functional outcomes recovery was greater in patients at low risk of postoperative erectile dysfunction and urinary incontinence, and the magnitude decreased according to the probability of long-term functional impairment. Additionally, the robotic approach was not associated with higher probability of recovering erectile function and urinary continence in patients included in the high erectile dysfunction and urinary incontinence risk groups after accounting for confounders. These findings indicate that preoperative patient characteristics, such as age at surgery, BMI, baseline comorbidities, and preoperative functional status, are more strongly correlated to the postoperative recovery of erectile function and urinary continence than the surgical approach itself.
Of note, these observations are consistent with observations made in the context of large population-based investigations. 9,10 Particularly, when evaluating a cohort of Medicare beneficiaries aged 65 and older Hu et al. 10 showed that men undergoing minimally invasive radical prostatectomy were more likely to be diagnosed as having postoperative urinary incontinence and erectile dysfunction. Barry and colleagues 9 used a rigorous survey instrument and reported no differences between RARP and ORP with regard to postoperative functional outcomes in Medicare-aged men, which usually represent sicker and older patients. Moreover, in these patients minimally invasive surgery did not lead to lower rates of perioperative morbidity, further questioning the benefits of RARP in this subset of men. 10 It is also noteworthy that the advantages related to the adoption of robotic surgery are greater in younger and healthier patients. Indeed, these men represent individuals who would suffer the most from the physical impairment and the consequent detrimental effect of erectile dysfunction and urinary incontinence on health-related quality of life related to the long-term side effects of radical prostatectomy. 25,26 Conversely, ORP and RARP had similar impacts on urinary continence and erectile dysfunction among older and sicker patients. Taken together, these findings suggest that preoperative patient selection is crucial in order to identify the best candidate for the robotic approach.
From a clinical standpoint, the results of our study have important implications. Although RARP seems to have oncologic results comparable with ORP at intermediate term, 27 recent studies evaluating large population-based cohorts of contemporary PCa patients questioned the advantages of robotic surgery in terms of perioperative outcomes and long-term functional results. 9,10 In this context, the evaluation of the comparative effectiveness of RARP and ORP is crucial, given substantially higher costs related to the adoption of the minimally invasive approach. 28,29 For example, it has been shown that RARP is associated with excess spending of approximately $4 million per year in the United States alone. 29 In this context, adoption of this technique only in patients who might benefit the most from minimally invasive surgery would result in substantial savings for the heath care system. The open approach would lead to comparable results with respect to erectile function and urinary continence recovery in patients included in the high erectile dysfunction and urinary incontinence risk groups; therefore, these older and sicker individuals may be properly counseled about the comparable outcomes between the two surgical approaches. To our knowledge, this investigation represents the first study showing that the advantages related to the adoption of robotic surgery depend on validated risk categories for functional outcomes recovery. These results may help clinicians select the best candidate for minimally invasive surgery.
Despite several strengths, our study is not devoid of limitations. First, our study is limited by its retrospective nature. Indeed, patients treated with RARP had better clinical and disease characteristics compared to their ORP counterparts. Although our multivariable analyses were adjusted for preoperative patient characteristics, we cannot rule out the possibility of other unmeasured variables influencing our results. On the other hand, we circumvented this limitation by stratifying patients according to their preoperative probability of erectile dysfunction and urinary incontinence. Second, all patients were treated at a tertiary referral center by experienced surgeons. Results obtained in this setting might not be generalizable to other clinical scenarios, where patient selection might be less rigorous. Third, all patients were treated with BNSRP. Consequently, our findings are not applicable to patients receiving a non-nerve sparing approach. Our study is also in part limited by the lack of adjustment for surgical volume or the surgeon's learning curve. This has to be acknowledged, as five different surgeons contributed to the present series; however, we should emphasize that all patients included in our study were treated by high-volume experienced surgeons at a single tertiary referral center. It is certainly possible that results may differ in other clinical settings, including those with single surgeons. For all of these reasons, external validation of our findings is required before suggesting the adoption of our stratification tools in everyday clinical practice. Ideally, this should be performed in the context of a prospective multi-institutional series.
Conclusions
RARP leads to higher urinary continence and erectile function recovery rates compared with ORP. Not all the patients benefit from the minimally invasive approach to the same extent, however: in patients with worse preoperative characteristics (i.e., older and sicker patients), RARP is not associated with better functional outcomes compared with ORP. Our findings indicate that, in order to achieve a more rational use of health care resources, patient selection is crucial for identification of the best candidates for RARP.
Footnotes
Disclosure Statement
No competing financial interests exist.