
Abstract
Purpose:
The purpose of this study was to assess the extent of the increased intracranial pressure (ICP) resulting from CO2 pneumoperitoneum and steep Trendelenburg positioning using ultrasonographic measurement of optic nerve sheath diameter (ONSD) in patients undergoing robot-assisted laparoscopic radical prostatectomy (RALRP).
Patients and Methods:
Twenty patients who underwent elective RALRP were enrolled in this study. ONSD and regional cerebral oxygen saturation (rSO2) were investigated noninvasively using ocular ultrasonography and near-infrared spectroscopy before anesthesia (T0), 10 minutes after anesthesia induction in the supine position (T1), 10 and 30 minutes after CO2 pneumoperitoneum with 30-degree Trendelenburg positioning (T2 and T3), and after returning to supine position without CO2 pneumoperitoneum at the conclusion of the RALRP (T4).
Results:
The mean values of ONSD at all time points (T1, T2, T3, and T4) after general anesthesia significantly increased compared with that before general anesthesia (T0). During CO2 pneumoperitoneum with 30-degree Trendelenburg positioning (T2, T3), a significant increase of 12.5% in ONSD was observed in comparison with ONSD after anesthesia induction in the supine position without CO2 pneumoperitoneum (T1). Three patients had an ONSD value equivalent to an ICP above 20 mm Hg, and these patients did not experience a decrease of rSO2 or any neurologic complications.
Conclusions:
In patients undergoing RALRP, the increase of 12.5% in ONSD during CO2 pneumoperitoneum with steep Trendelenburg positioning was observed and thus the increase of ICP corresponding to this change of ONSD could be predicted. In 15% of the enrolled patients, ONSD increased by values equivalent to an ICP above 20 mm Hg without a deterioration of rSO2 or any neurologic complications.
Introduction
R
The increase of intracranial pressure (ICP) has been considered a major cerebrovascular effect, which is caused by CO2 pneumoperitoneum and Trendelenburg positioning either independently or in conjunction. 4 –6 Because the most reliable method for the assessment of ICP is the insertion of an invasive intracranial device, however, monitoring ICP during laparoscopic surgery is almost impossible because of concerns regarding severe complications such as hemorrhage, infection, and equipment malfunction. 7 Hence, the extent and safety of elevated ICP caused by pneumoperitoneum and Trendelenburg positioning are currently unknown.
Optic nerve sheath diameter (ONSD) measurement using ocular ultrasonography is a novel, noninvasive and reproducible technique for the assessment of ICP. 7,8 Previous studies have demonstrated the accuracy of ONSD measurement for diagnosing and assessing elevated ICP from various causes. 7,9 –11 Thus, we hypothesized that the extent of the raised ICP during RALRP could be ascertained without risks of serious complications if ONSD was measured and compared using ultrasonography at regular intervals instead of the invasive technique for assessing ICP.
The purpose of this observational, single-center study was to assess the extent of the increased ICP resulting from CO2 pneumoperitoneum and steep Trendelenburg positioning using ultrasonographic measurement of ONSD in patients undergoing RALRP.
Patients and Methods
After acquiring approval from the Institutional Review Board of Severance Hospital, Yonsei University Health System (4-2012-0287), we registered this study in ClinicalTrials.gov (ref: NCT01641302). Before enrollment, written informed consent was obtained from all participants. Twenty adult male patients who were American Society of Anesthesiologists class I to III and scheduled for an elective RALRP using the da Vinci™ robot system (Intuitive Surgical, Inc., Mountain View, CA) were enrolled in this study. We excluded patients with preexisting ophthalmic or neurologic disease or a history of ophthalmic surgery or neurosurgery.
The participants were not premedicated. On arrival in the operating room, standard monitoring was applied, including electrocardiography, pulse oximetry, and noninvasive arterial blood pressure. General anesthesia was induced with propofol 1.5 mg/kg, and remifentanil 1 μg/kg. Rocuronium bromide 0.6 mg/kg was administered intravenously to facilitate orotracheal intubation. After tracheal intubation, mechanical ventilation was performed with a tidal volume of 8 mL/kg and an adjusted respiratory rate to maintain an end-tidal carbon dioxide (EtCO2) of 35 to 40 mm Hg during surgery.
Radial artery cannulation was performed for continuous monitoring of arterial blood pressure and analysis of arterial blood gas. Anesthesia was maintained with remifentanil 0.05 to 0.2 μg/kg/min and 1 to 1.5 minimum alveolar concentration (MAC) of desflurane in 50% oxygen/air. A bispectral index score (BIS) monitor (A-2000 BIS Monitor™, Aspect Medical System Inc., Newton, MA) was monitored continuously to maintain an adequate anesthetic depth and was targeted at a range of 40 to 50 during surgery. For assessment of regional cerebral oxygen saturation (rSO2) during surgery, sensors for cerebral oximetry were applied bilaterally at least 2 cm above the eyebrow on the left and right sides of the forehead before anesthesia induction. The value of rSO2 was continuously monitored using near-infrared spectroscopy (INVOS 5100™, Somanetics Corp., Troy, MI). A forced-air warming system (Bair-Hugger™, Augustine-Medical, Eden Prairie, MN) was applied throughout surgery to maintain body temperature at 36.0–37.0°C.
CO2 pneumoperitoneum was achieved with an intra-abdominal pressure of 15 mm Hg using the da Vinci™ robot system while the patient's position was supine and then 30-degree Trendelenburg positioning was applied. During pneumoperitoneum, minute ventilation was controlled to maintain an EtCO2 of 35 to 40 mm Hg by adjusting the respiratory rate.
Ultrasonographic measurement of ONSD was conducted by a single trained investigator (MSK) with more than 30 scans of experience, as described in previous studies. 12,13 A linear 13- to 6-MHz ultrasound probe (Sonosite™, Bothell, WA) was placed carefully on the gel over the closed upper eyelid without exerting pressure on the eye. In the two-dimensional mode, ONSD was measured 3 mm behind the globe using an electronic caliper as illustrated in Figure 1.
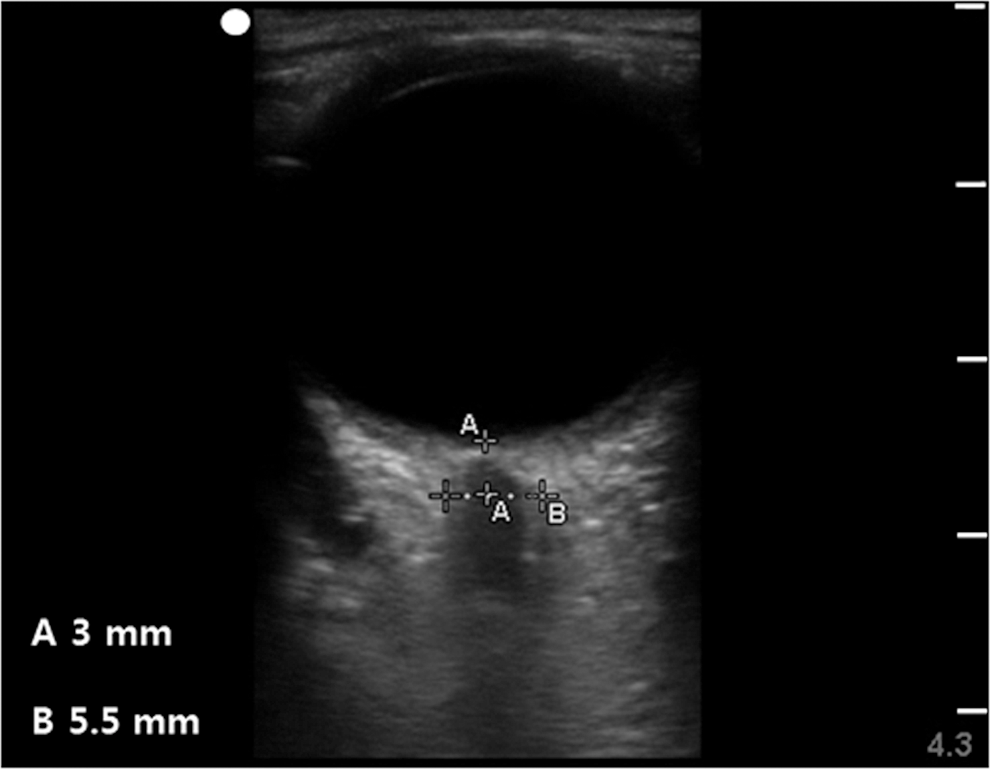
Ultrasonographic measurement of optic nerve sheath diameter.
Four measurements were performed for each optic nerve—two in the transverse plane and two in the sagittal plane. The final ONSD corresponded to the average of the eight values measured in both eyes of each patient. The ONSD and additional data, including vital signs, the values of BIS and rSO2, the parameters regarding respiratory mechanics, and arterial blood gas analysis, were examined at five discrete time points as shown in Table 1. In addition, we assessed the duration of Trendelenburg positioning, operation and anesthesia times, intraoperative blood loss, and the volume of administered fluid.
rSO2=regional cerebral oxygen saturation; BIS=bispectral index score; ONSD=optic nerve sheath diameter; RALRP=robot-assisted laparoscopic radical prostatectomy.
A calculation of sample size was performed on the basis of a previous study comparing the differences in ONSD between patients with elevated ICP (6.4±0.7 mm) and normal adults (4.6±0.3 mm). 13,14 Given a 5% two-tailed significance level (α=0.05) and a power of 90%, 20 patients were needed to detect a mean difference of 0.4 mm between ONSD in the supine position before anesthesia and that in Trendelenburg position with CO2 pneumoperitoneum after anesthesia.
Statistical analysis was conducted using the Statistical Package for the Social Sciences 18.0 for Windows (SPSS Inc., Chicago, IL). All data were reported as mean±standard deviation or median (range) as appropriate. A linear mixed model with an unstructured type as repeated covariance structure was used to compare ONSD values and other continuous variables, which were assessed at each time point. If there were overall differences between values at each time point, post hoc multiple comparisons were performed using the Bonferroni correction. A P value less than 0.05 was considered statistically significant.
Results
A total of 20 patients participated according to the study protocol without any exclusions or withdrawals. Patient characteristics and intraoperative data are described in Table 2.
Results are given as mean±standard deviation, median (range).
The mean values of ONSD, rSO2 score, and hemodynamic variables at each time point are presented in Table 3. The mean values of ONSD at all time points (T1, T2, T3, and T4) after general anesthesia significantly increased compared with that before general anesthesia (T0). During CO2 pneumoperitoneum and 30-degree Trendelenburg positioning (T2, T3), a significant increase of 12.5% in ONSD was observed compared with ONSD in the supine position without CO2 pneumoperitoneum after induction of general anesthesia (T1). Three patients had a value of ONSD above 5.8 mm (the cutoff value for prediction of ICP above 20 mm Hg in a previous study), 7,9 and these patients did not experience a decrease of rSO2 or any neurologic complications. Among these three patients, one patient with an ONSD of 6.6 mm in T2 and T3 had an ONSD of 5.3 mm in T0 as a baseline value. The ONSD values in T2 and T3 of the remaining two patients were less than 6.0 mm. Figure 2 shows the distribution of the ONSD values measured at each time point. The mean scores of rSO2 at all time points (T1, T2, T3, and T4) after general anesthesia also increased significantly in comparison with that before general anesthesia (T0) without a reduction of the rSO2 scores during the period of pneumoperitoneum or Trendelenburg positioning.
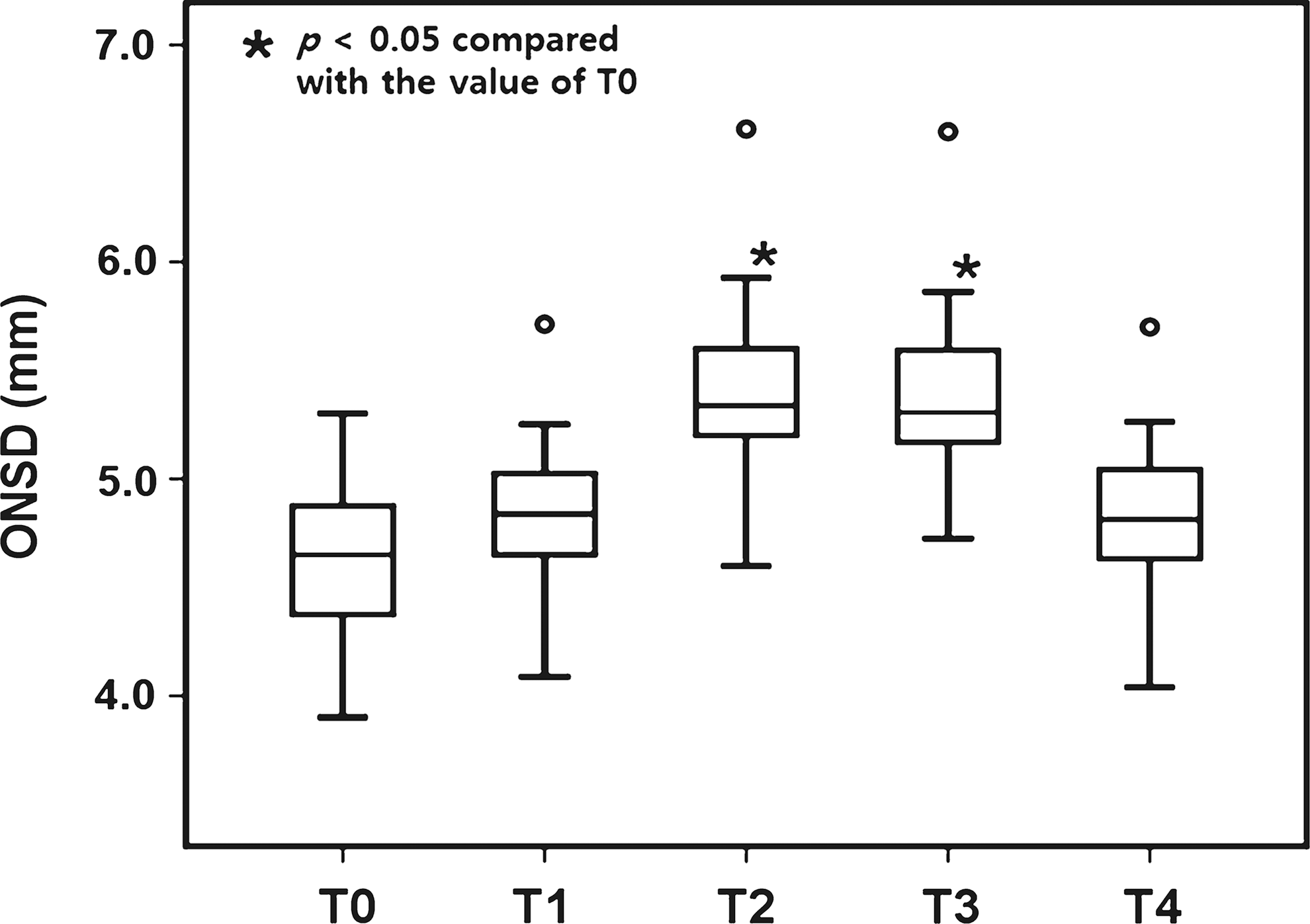
Distribution of optic nerve sheath diameter (ONSD) values measured at each time point. The box includes the middle 50% of the data, and the line inside the box is the median of the data set. The top and bottom of the box are the third and first quartiles of the data set. The range of the middle two quartiles represents the interquartile range. The ends of the whiskers that can extend to a maximum of 1.5 times the interquartile range indicate the minimum and maximum values of all the data, if outliers are not present. Outliers mean any cases that are not contained between whiskers, that extend maximally, and were plotted using a circle.
P<0.05 compared with the value of T0.
P<0.05 compared with the value of T1.
Results are given as mean±standard deviation.
ONSD=optic nerve sheath diameter; rSO2=regional cerebral oxygen saturation; HR=heart rate; BP=blood pressure.
The variables regarding respiratory mechanics and arterial blood gas analysis data are presented in Table 4. After establishing CO2 pneumoperitoneum in the 30-degree Trendelenburg position (T2, T3), both the peak inspiratory pressure and plateau pressure were significantly higher than those in the supine position without CO2 pneumoperitoneum (T1). The EtCO2 and arterial partial pressure of CO2 (PaCO2) increased significantly after CO2 pneumoperitoneum compared with the baseline values.
P<0.05 compared with the value of T1.
Results are given as mean±standard deviation.
EtCO2=end-tidal carbon dioxide; PaCO2=arterial carbon dioxide partial pressure; PaO2=arterial oxygen partial pressure.
Neurologic complications were not observed in any of the enrolled patients during the intraoperative or postoperative periods.
Discussion
With the increasing frequency of RALRP, the impact of CO2 pneumoperitoneum and steep Trendelenburg positioning on ICP warrants careful consideration. The results of our study reveal that an increase of 12.5% in ONSD was observed during CO2 pneumoperitoneum and steep Trendelenburg positioning and 15% of the enrolled patients had ONSD values equivalent to an ICP above 20 mm Hg without a reduction in cerebral oxygenation or abnormal neurologic signs.
In contrast to other surgical procedures, in RALRP, the increase in arterial CO2 tension (PaCO2), the increased intra-abdominal pressure under CO2 insufflation, and the effect of steep Trendelenburg positioning can be considered to be possible precipitating factors of elevated ICP. 5,6 Cerebral blood flow (CBF) changes 1.8 mL/100 g/min for each 1 mm Hg change in the PaCO2. 15 CO2 insufflation to induce pneumoperitoneum increases the CBF, and the ICP is accordingly elevated. 4,16 In this study, the values of PaCO2 analyzed after pneumoperitoneum were slightly increased compared with those after anesthesia induction. Hence, the increased PaCO2 might partially contribute to the elevated ICP, although the levels of both EtCO2 and PaCO2 were close to normocapnia after adjusting the respiratory rate.
Previous research by Halverson and associates 5 showed that the direct physical effects of CO2 pneumoperitoneum could raise the ICP, independent of other factors such as PaCO2 and mean arterial pressure. In their research performed in pigs with CO2 pneumoperitoneum, the impairment of cerebrospinal fluid drainage at the level of the lumbar venous plexus caused by increased intra-abdominal pressure was proposed as the mechanism leading to the elevated ICP associated with CO2 pneumoperitoneum. This animal research additionally reported that the increase in ICP caused by CO2 insufflation could be exacerbated in the Trendelenburg position and could not be mitigated in the reverse Trendelenburg position. Hence, a greater increase in ICP can be predicted in RALRP because of simultaneous use of CO2 pneumoperitoneum and the Trendelenburg position in comparison with other surgical procedures using only CO2 pneumoperitoneum in the supine position.
The effect of steep Trendelenburg positioning on ICP has been investigated in human and animal studies. A human study conducted in neurosurgical patients under general anesthesia reported that the head-down position and head rotation and/or flexion could increase ICP. 6 In animal studies investigating the effects of head-down tilt (HDT) on ICP in conscious or anesthetized rabbits, HDT resulted in an initial small elevation of ICP accompanied by a further gradual increase in the first 12 hours of HDT in conscious rabbits. In contrast, in anesthetized rabbits, HDT created an initial, remarkable elevation of ICP, which was accompanied by a gradual decrease during 8 hours of HDT. 17 –19 These previous studies proposed fluid shift and venous engorgement in the head-down position as well as impediment of cerebral venous drainage by the increase in central venous pressure as causes of the increase in ICP. 17,19,20 Given these results from animal studies, it can be predicted that in humans, steep Trendelenburg positioning, especially in the anesthetized state, may raise ICP more rapidly than in the conscious state.
Volatile anesthetics have intrinsic cerebral vasodilatory activity, resulting from direct effects on vascular smooth muscle. 21 Because this vasodilatory activity predominates under anesthesia beyond 1.0 MAC, cerebral blood flow increases significantly during general anesthesia and, consequently, an increase in ICP can occur. 22 –24 In the present study that used desflurane as a volatile anesthetic, the ONSD measured after anesthesia induction without pneumoperitoneum and Trendelenburg positioning slightly increased compared with that before anesthesia induction. Because more than 1 MAC of volatile anesthetic is generally administered during anesthesia induction and maintenance, a modest increase in ICP can be expected during anesthesia regardless of pneumoperitoneum or posture changes; however, the effect of inhalation agents on ICP was well controlled in the current study, because anesthesia in all enrolled patients was identically maintained with a 1 to 1.5 MAC of desflurane. In addition, the ONSD values measured during pneumoperitoneum and Trendelenburg positioning were significantly increased compared with those measured after anesthesia induction.
The best way to reliably measure ICP is the placement of an invasive ventricular catheter 7 ; however, the risk of severe complications related to coagulation disorders and the absence of neurologic surgeons are limitations of using this invasive modality to actively assess the ICP. 11 In particular, considering its serious complications, such as cerebral hemorrhage, the use of such an invasive procedure for monitoring ICP may be very burdensome for patients undergoing other nonneurosurgical procedures, even though these patients have a risk of elevated ICP during procedures. Therefore, a noninvasive and easy-to-use technique of assessing ICP for these patients is needed during the intraoperative period.
ONSD measurement using ocular ultrasonography is a noninvasive and simple technique for assessing elevated ICP. 14 The subarachnoid space surrounding the retrobulbar portion of the optic nerve is distensible and can accordingly expand when cerebrospinal pressure increases. 7 Geeraert and colleagues 7,9 reported that ultrasonographic measurement of ONSD was correlated with ICP as measured by the insertion of an invasive catheter, and ONSD enlargement greater than 5.8 mm was likely to be associated with an ICP of >20 mm Hg, the point at which therapy to reduce ICP may be needed. 25
In the present study, mean values and 95% confidence intervals of ONSD measured in pneumoperitoneum with steep Trendelenburg positioning were less than 5.8 mm, and three patients had an ONSD value above 5.8 mm. From these results, it can be assumed that the extent of the elevated ICP in most patients undergoing RALP is less than 20 mm Hg. In addition, considering the maintenance of adequate cerebral oxygenation without a reduction in rSO2, the impact of this modest elevation of ICP may be limited; however, ICP in patients having lesions such as brain tumors or injury may increase abruptly with the establishment of pneumoperitoneum. Josephs and coworkers 26 demonstrated that there was a significant increase in ICP from 22.6 to 27.4 mm Hg when applying artificial pneumoperitoneum in an animal model with intracranial injuries. Therefore, special care regarding raised ICP is needed in patients with brain lesions undergoing RALRP.
The present study has some limitations. First, the lack of experience with ocular ultrasonography may be a possible limitation of this method. Tayal and colleagues 12 showed that, for physicians without previous experience in ocular ultrasonography, 25 scans may be needed to get an adequate image of ONSD, suggesting that the learning curve is fairly steep. In this study, the examiner performed measurements of ONSD only after sufficient experience of more than 25 scans.
Second, variability in ONSD values measured by ultrasonography should be considered. As reported by Ballantyne and associates, 27 ultrasonographic measurement of ONSD is an easily learned and reproducible modality and its observer variation (0.2–0.3 mm) is similar to the innate variability of the ultrasound machine. In addition, the difference between ONSD after CO2 pneumoperitoneum with Trendelenburg positioning and that after induction is approximately 0.6 mm greater than the reported values of observer variation. Therefore, the differences in ONSD obtained from this study can be fully meaningful results despite an intraobserver variation.
Third, the effect of CO2 pneumoperitoneum itself on change in ICP was not ascertained in this study because ONSD under CO2 pneumoperitoneum and supine position was not measured. This period, however, for inserting instruments of robotic surgery was so short that we could not measure and evaluate ONSD adequately. In addition, if the progress of the surgery was stopped for adequate assessment of ONSD, the operation and anesthesia time could be unnecessarily prolonged, and this practice could not be beneficial to the enrolled patients.
Last, a sample size of 20 patients seems to be somewhat small, although a power analysis for sample size was performed on the basis of the results of previous studies. In addition, the possibility of variation and fluctuation in ICP during the intraoperative period should be considered to interpret our results. Hence, additional studies including a large number of participants should be planned and performed under consideration of this possibility.
Conclusion
Given that the increase of 12.5% in ONSD was observed during CO2 pneumoperitoneum with steep Trendelenburg positioning, the increase of ICP corresponding to this change of ONSD could be predicted in patients undergoing RALRP. Only 15% of the enrolled patients, however, had ONSD values equivalent to an ICP above 20 mm Hg, and these patients did not experience a deterioration of rSO2 or any neurologic complications. Therefore, the elevated ICP during CO2 pneumoperitoneum with steep Trendelenburg positioning is not likely to adversely affect patients undergoing RALRP. The clinical relevance of the elevated ICP during RALRP still needs to be ascertained through further evaluation.
Footnotes
Disclosure Statement
No competing financial interests exist.