
Abstract
Background and Purpose:
Retroperitoneal laparoscopic nephroureterectomy (LNU) is a classic technique for the treatment of patients with urothelial cancer of the upper urinary tract. Management of the distal ureter in patients undergoing this procedure remains controversial, however. We evaluated a new method involving cystoscopic sleeve resection of the distal ureter using a 2-μm continuous wave laser before LNU.
Patients and Methods:
LNU was performed in 38 patients at our hospital between January 2008 and January 2012. The distal end of the ureter was managed by using a 2-μm continuous wave laser to evaporate and excise the ureteral orifice and bladder cuff. A standard technique was applied to keep the ureter intact. The ureter was dissected to the entrance of the bladder, and the distal ureter was easily detached from the bladder.
Results:
The distal ureter was excised completely in all cases using this new technique. The average operative time was 2.4 hours, and the average blood loss was 69.4 mL. At 1 year after surgery, the cause-specific survival rate of the patients was 100%, the bladder recurrence-free rate was 89%, and the extravesical recurrence-free rate was 100%.
Conclusions:
For managing the distal ureter during LNU, the new technique described proved to be a simple, safe, and minimally invasive method.
Introduction
U
Since retroperitoneal laparoscopic nephroureterectomy (LNU) was first reported in 1991 by Clayman and colleagues, 4 the benefits of this procedure have been established. An increasing number of urologists are sharing their experiences with minimally invasive techniques worldwide. 5,6 The optimal technique for managing the bladder cuff has not been established, however.
We reviewed the recent literature regarding management of the distal ureter, for which there is no consensus, and applied a new method of cystoscopic sleeve resection of the distal ureter using a 2-μm continuous wave laser, which is technically easy but still follows traditional oncologic principles.
Patients and Methods
Patients
Thirty-eight patients with urothelial-cell carcinoma of the renal pelvis were treated with LNU using our new distal ureter technique between January 2008 and January 2012. Data on all patients were collected retrospectively, including their demographic characteristics, surgical details, and treatment outcomes.
The protocol for this study was approved by the Ethics Committee of the PLA General Hospital, Beijing, China.
Management of the lower ureter and bladder cuff
In all cases, patients were initially placed in the lithotomy position, and the operations were performed under general anesthesia. A RevoLix 2-μm continuous wave medical laser surgical system (LISA Laser Products, Katlenburg-Lindau, Germany) was used. The wavelength of the laser was 2.013 μm, and the energy was transmitted through a 550-μm optical fiber. 7 The power was set initially to 40 W for the operation. A 26-F, 12-degree laser resectoscope (Storz, Tuttlingen, Germany) and a physiologic saline (0.9%) rinse solution were used intraoperatively.
After insertion of the laser resectoscope into the bladder, we observed the ureteral orifice position on the operative side. After confirming the absence of bladder tumors, the optical fiber probe was inserted into the bladder through the operation channel of the laser resectoscope. The 2-μm laser fiber was used to excise the ureteral orifice circularly while shaping a 1-cm bladder cuff. The excision was performed circumferentially 5 mm around the ureteral orifice. To avoid inadvertent transection of the ureter, the ureteral orifice was then dissected from the upper half of the dissection circle.
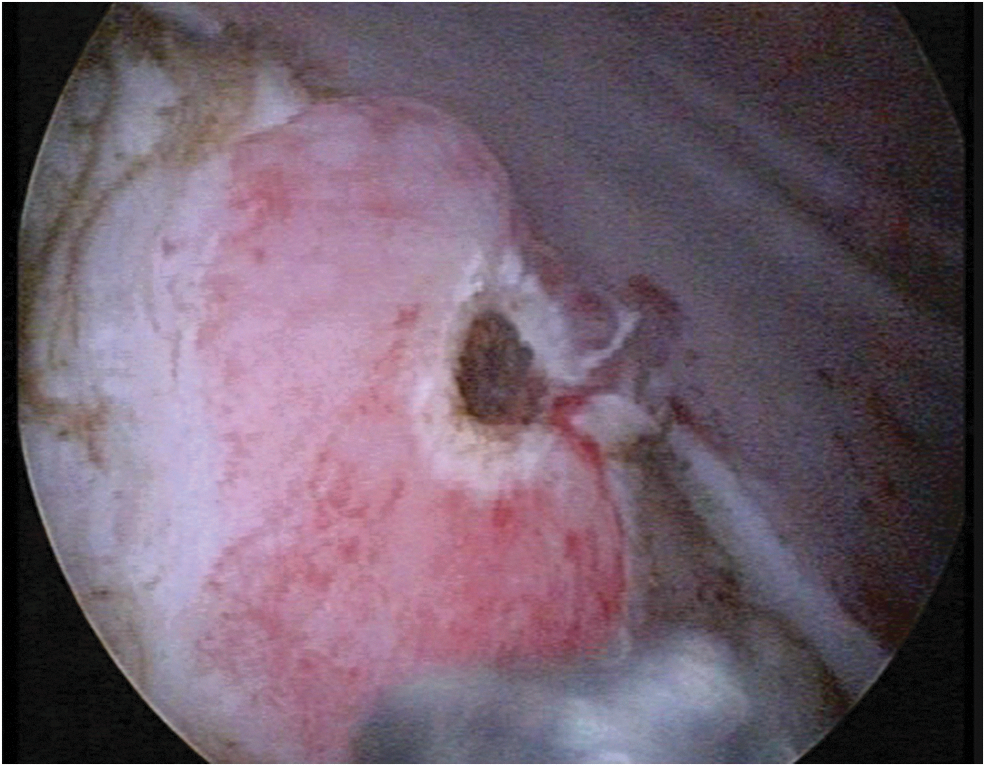
The normal mucous membrane, submucosa, muscle layer, and fibrous connective tissues in the outer layer of the bladder were vaporized and incised. Blunt stripping was conducted with the tip of the laser resectoscope along the loose space between the detrusor muscle layer and the outer connective tissue layer. Dissection of the ureteral stump was performed until perivesical fat was found, and the ureter was then detached from the bladder wall (Fig. 1). At this stage of the dissection, overdistention of the bladder might lead to extravasation of the irrigation fluid.
A 2-μm laser fiber was used to score the ureteral orifice circumferentially while maintaining a 1-cm bladder cuff. The mucosa of the ureteral orifice was vaporized and closed by the laser fiber to achieve a closed system in the upper urinary tract.
Finally, the laser power was reduced to 30 W, and the mucosa of the ureteral orifice was vaporized and closed by a laser fiber to achieve a closed system in the upper urinary tract, which minimized the risk of tumor seeding (Fig. 2). The bladder was drained with a 16F Foley catheter.

Cystoscopic sleeve resection of the distal ureter by a 2-mm continuous wave laser ensured complete en bloc excision of the distal ureter and bladder cuff.
Retroperitoneal LNU
Subsequently, the patient was positioned in a standard 90-degree full-flank position for nephrectomy. To maximize the working space between the lowermost rib and the iliac crest, the kidney bridge was elevated and the operating table was flexed. The pressure points were all well padded, and the extremities were placed in a neutral position.
A 2-cm incision was made above the lateral border of the erector spinae muscle and below the 12th rib. A homemade retroperitoneal balloon inflated to 600 to 800 mL was used to create a retroperitoneal space. We then placed a 12-mm port subcostally at the midaxillary line and the lateral border of the erector spinae muscle; a 5-mm port posterior to the tip of the 12th rib; and a 10-mm port at the midaxillary line 3-cm cephalad to the iliac crest. By applying pressure with 12 to 14 mm Hg CO2, a pneumoperitoneum was created, and by dissecting along the psoas muscle, the posterior surface of the kidney was reflected medially. Before exposing the kidney, the ureter was ligated using a Hem-o-lok clip to avoid shedding of tumor cells.
With dissection of the renal artery and vein, the renal pedicle was identified and renal pedicle lymph node dissection was performed when the lymph node was located. The ureter was mobilized beyond the point where it crosses the common iliac vessels, and the lower ureter was separated to the bladder adventitia. The ureter was then easily pulled out, and the laser scar of the distal ureter, a sign of full-length ureteral resection, was found. The dissected specimen was entrapped with an EndoCatch bag (US Surgical Corp., Norwalk, CT) and removed intact through the initial incision. Careful hemostasis was performed, and an indwelling retroperitoneal drainage tube was placed before completion of the surgery.
Results
There were 25 men and 13 women patients with a mean age of 65.3 years (range 54–76 years). Thirty-seven patients had a history of intermittent painless gross hematuria and 1 had a history of lumbar pain. All of the tumors were located in the renal pelvis (15 on the left and 23 on the right).
We achieved cystoscopic sleeve resection of the distal ureter in all cases by using a 2-μm continuous wave laser. The laser scar of the distal ureter, a sign of full-length ureteral resection, was found in all patients. Hydroureteronephrosis was observed in 31 specimens. This sign indicated that the lower end of the ureter was closed by the laser (Fig. 3). The total mean operative time was 126 minutes (range 95–260 min), and the mean time for the cystoscopic part of the operation was 17.0 minutes (range 10–22 min).
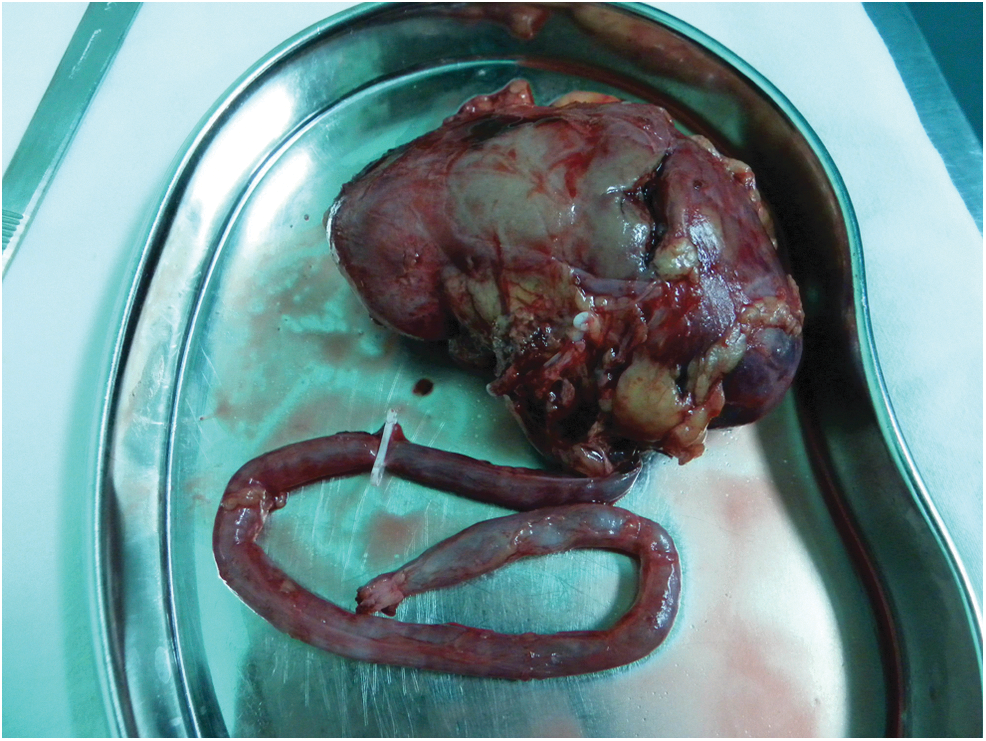
Hydroureterosis was found in 31 specimens. This indicated that the lower end of the ureter was closed by the laser.
Pathologic findings included 15 high-level and 23 low-level urothelial carcinomas. Renal pedicle lymph node dissection was performed in 12 patients, and no lymph node metastases occurred. Histopathologic analysis of the distal cuff was negative for cancer cells in all 38 patients (Table 1). Irrigation fluid extravasation was minimal during the cystoscopic procedure, and hyponatremia developed intra- or postoperatively in none of the patients. Cystography was performed intraoperatively in the first 16 patients just after management of the lower ureter and bladder cuff.
The volume of meglumine diatrizoate was 300 mL, and no obvious contrast medium extravasation was detected. The cystoscopic dissection was associated with minimal blood loss, and the patients' mean total blood loss was 69.4 mL. The mean duration of drainage was 2.6 days (range 2–3 days). None of the patients needed a blood transfusion.
Complications occurred in one patient in whom an infection developed at the incision site in the postoperative period. The mean postoperative indwelling catheter time was 6.4 days (range 6–7 days), and urinary leaks did not develop in any patient. The mean duration of hospital stay was 9.6 days (range 5–20 days). Because patients are hesitant to leave the hospital with an indwelling Foley catheter, this duration of hospital stay is common in our healthcare system, and most patients were discharged after successful catheter removal. Intravesical chemotherapy of the bladder using epirubicin or pirarubicin instillations was administered while removing the catheter.
Postoperatively, the patients were followed for 12 to 60 months (mean 36.5 mos). Thirty-one patients underwent cystoscopy, and bladder tumor recurrence in the ipsilateral hemibladder close to the ureteral scar/orifice was noted in 4 (12.9%). No recurrent tumors were detected at the ureteral scar/orifice or in the perivesical space, however, and none of the patients had a metastasis at a port site.
Discussion
Urothelial-cell carcinoma of the upper urinary tract is a serious condition. With the development of laparoscopic techniques in urology, LNU has become a commonly used procedure for the treatment of patients with renal pelvic and ureteral urothelial-cell carcinoma. LNU can achieve shorter hospitalization, decreased perioperative morbidity, and good oncologic outcomes and survival rates compared with open nephroureterectomy. 8 In recent years, this technique has undergone numerous modifications, and LNU is now performed using the same surgical principles as radical nephrectomy by laparoscopy.
There are two LNU approaches that can be chosen—transperitoneal or retroperitoneal. Although the retroperitoneal approach is commonly used because surgeons are generally more familiar with it, management of the distal ureter with this approach is difficult. 9 While many endoscopic distal ureteral management techniques have been described, 10 the most oncologically appropriate method is still the open technique. The open technique includes two approaches—transvesical and extravesical. The distal ureter and bladder cuff may not be excised completely by the extravesical approach. Also, in patients with a history of pelvic surgery and radiotherapy and those with obesity, the open technique may be difficult to perform. In some patients, urine spillage may lead to vesical or paravesical recurrences.
A focus of nephroureterectomy is avoidance of extravesical transfer of tumor-containing urine when managing the bladder. 11 By using the “pluck” technique, which refers to transurethral resection of the distal ureter down to the perivesical fat, the distal ureter can be readily plucked during LNU. 12 Because urine extravasation from the detached ureter may transfer tumor cells to the perivesical space, there have been reports of tumor recurrences in the perivesical space. 13,14 Blind pulling of the distal ureter may result in avulsion of the ureter and cannot achieve a complete ureter.
Transvesical laparoscopic detachment and ligation of the distal ureter using two transvesical ports was described by Gill and associates 15 and Agarwal and coworkers, 16 who reported a modified method of detachment of the distal ureter under cystoscopy using a Collins knife. Subsequently, Mueller and associates 17 improved the method of Agarwal and coworkers 16 by injecting Tisseel® and indigo dye into the ureter to confirm the presence of ureteral blockage. Shalhav and colleagues 18 described a method of stapling the distal ureter by laparoscopy, and Lambert and coworkers 19 reported on a sealed bladder cuff technique during LNU using the LigaSure electrosurgical device.
Each method has its own advantages and disadvantages. The best choice is the surgeon's own preference as long as basic oncologic principles are preserved, including complete resection of the ureter and bladder cuff and avoidance of tumor planting.
In cases of incomplete upper urinary tract removal, the tumor recurrence rate is between 30% and 64%, with recurrences invariably being observed in the residual ureteral stump/periureteral meatal region. 20 –22 Consequently, it is necessary to completely excise the whole ureter (including the distal ureter with its intramural part), the ipsilateral ureteral orifice, and the bladder cuff. After blocking of the ureteral orifice, total excision can be achieved by removal of an en bloc closed-system specimen. Provided the distal ureter is ligated and divided at a tumor-free location, the continuity of the specimen may be conceded to aid ease of extraction. In the process, it is extremely important to avoid extravesical urine extravasation to reduce the risk of tumor cell seeding.
Our technique is a modification of transurethral resection of the ureteral orifice that provides several advantages. As well as duplicating the oncologic principles of the open technique, it is truly laparoscopic and cystoscopic without any transvesical ports. The technique needs only a short learning time, is more minimally invasive than other techniques, and the cystoscopic dissection saves time. In the patients described, the mean cystoscopic dissection time with the technique was 17.0 minutes, and blood loss was nil. More precise bladder wall anatomy can be obtained by laser vaporization and incision combined with blunt stripping.
The technique can achieve a closed system in the upper urinary tract because of coagulation of the ureteral orifice mucosa. Because the ureter has been completely detached and a little hole in the bladder is open, the little hole through the bladder wall can be closed by the detrusor muscle and adipose tissue near the bladder so it can avoid extravesical urine contact under normal internal bladder pressure.
During the operation, attention should be paid to several aspects. To avoid injury, the distal ureter should be dissected carefully, especially in the upper half of the dissection circle, and care should be taken to avoid detaching the ureter and to continue rinsing the bladder when exposing the perivesical fat to avoid extravasation of irrigation fluid. Sometimes, the ureteral stump can be dissected with the aid of a catheter. Before dissecting the ureter, it should be ligated using a Hem-o-lok clip to avoid shedding of tumor cells. The ureter should be stretched gently to avoid fracturing, and the completeness of the distal ureter should be checked. The Foley catheter should be retained for at least 6 days postoperatively before intravesical chemotherapy is administered.
Comparatively, our method is simpler than other techniques. In all patients treated, complete excision of the intramural ureter and bladder cuff was achieved, and the distal and outer surgical margins were clear. During follow-up, the oncologic outcomes appeared satisfactory, and recurrences were not found at the ureteral scar or in the perivesical space. Additional long-term, prospective, randomized studies are needed to evaluate outcomes with this new technique, however.
Conclusion
Although the optimal approach to managing the distal ureter during LNU has not been determined, our technique of cystoscopic sleeve resection of the distal ureter by using a 2-μm continuous wave laser method ensured complete en bloc excision of the distal ureter. This technique is minimally invasive and needs only a short learning time. We recommend this procedure for the management of the distal ureter during LNU. Randomized, controlled studies with a longer follow-up time are needed to confirm these findings, however.
Footnotes
Disclosure Statement
No competing financial interests exist.