
Abstract
Purpose:
To report our experience and the feasibility of transvaginal ureterectomy for refluxing ectopic ureter after laparoscopic ureteroureterostomy. Ureteroureterostomy is a treatment modality for preserving upper pole kidney function in patients with complete duplicated ureters (CDU). Because of the residual ureteral stump, however, the development of urinary tract infection may be a concern.
Patients and Methods:
We retrospectively reviewed the data of patients with a diagnosis of CDU who underwent surgery between 2007 and 2012. Six female patients with CDU were identified. Of these six patients, four underwent transvaginal ureterectomy after laparoscopic ureteroureterostomy.
Results:
No patients experienced intraoperative complications. Total mean surgical time in four patients was 250 minutes. Mean laparoscopic ureteroureterostomy time took 180 minutes, and ureterectomy by vaginal incision took 40 minutes, respectively. Mean blood loss was 150 mL. The first patient experienced postoperative complications of mild urine leak and ureteral stricture in the anastomosed site.
Conclusions:
Our experience suggests that transvaginal ureterectomy after laparoscopic ureteroureterostomy is a minimally invasive modality that may be a technically feasible and effective option for patients who have CDU with refluxing ectopic ureters.
Introduction
D
Because complete duplicated ureters (CDU) usually have complicated anatomy and function, there are a variety of treatments, including reconstruction of the upper and lower urinary tracts. CDU are frequently associated with an obstructed, poorly functioning upper pole moiety. When symptoms of urinary tract infection or flank pain in the poorly functioning upper pole moiety are reported, the standard treatment is upper pole heminephrectomy. 4 –6 Other urinary tract anomalies, including vesicoureteral reflux, ureterocele, and ectopic ureters, are frequently associated with CDU. When symptoms of vesicoureteral reflux and a moderately functioning upper pole moiety are reported, the treatment option is surgical management, including various techniques of surgical reconstruction, such as ureteroureterostomy or pyeloureterostomy. 7,8 Of these techniques, ureteroureterostomy is known to be effective in preserving upper pole moiety function. 9 However, subtotal or total ureterectomy of the distal refluxing ectopic ureter after ureteroureterostomy is still being debated. Because of retained ureteral stumps, urinary tract infection might develop, and an additional surgical procedure could be needed. 10 –13
In the present study, to avoid complete ureterectomy that necessitates an operation at the bladder level, exposing the normal pole ureter to the danger of vascular injury, 14 –16 we present transvaginal ureterectomy on behalf of total ureterectomy for distal ectopic ureteral stump after laparoscopic ureteroureterostomy. Also, we report our surgical techniques for laparoscopic ureteroureterostomy and transvaginal ureterectomy.
Patients and Methods
We retrospectively reviewed the data of patients with a diagnosis of CDU who underwent surgery between 2007 and 2012. CDU was identified in six women. Two patients underwent robot-assisted laparoscopic heminephrectomy because of a poorly functioning upper pole moiety. Heminephrectomy is surgically indicated for patients with poorly functioning upper pole moieties.
The remaining four patients who had a moderately functioning upper pole moiety and refluxing ectopic ureters underwent transvaginal ureterectomy after laparoscopic ureteroureterostomy. Ureteroureterostomy and ureterectomy were the preferred surgical techniques used in the four patients who had moderate upper pole moiety function with about 30% to 40% renal function. Demographic, diagnostic, and procedural data of the patients were recorded (Table 1). All patients had complained of flank pain and urinary incontinence. Cystoscopy was performed in an outpatient clinic, and an ectopic orifice was found in the area of the bladder neck. Intravenous urography, voiding cystourethrography, retrograde ureteropyelography, and dimercapto-succinic acid (DMSA) scintigraphy were needed to demonstrate and reveal CDU with a grade 3 to 5 refluxing ectopic ureter. One woman who presented at her follow-up appointment with flank pain, worsening hydronephrosis, and frequent urinary tract infection.
G/U=genitourinary; VUR=vesicoureteral reflux; VU=vaginal ureterectomy; UU=ureteroureterostomy; SA=stricture in anastomosed site; UTI=urinary tract infection.
In our study, a hybrid technique composed of laparoscopic ureteroureterostomy and open transvaginal ureterectomy on behalf of total ureterectomy was used.
Preoperative preparation
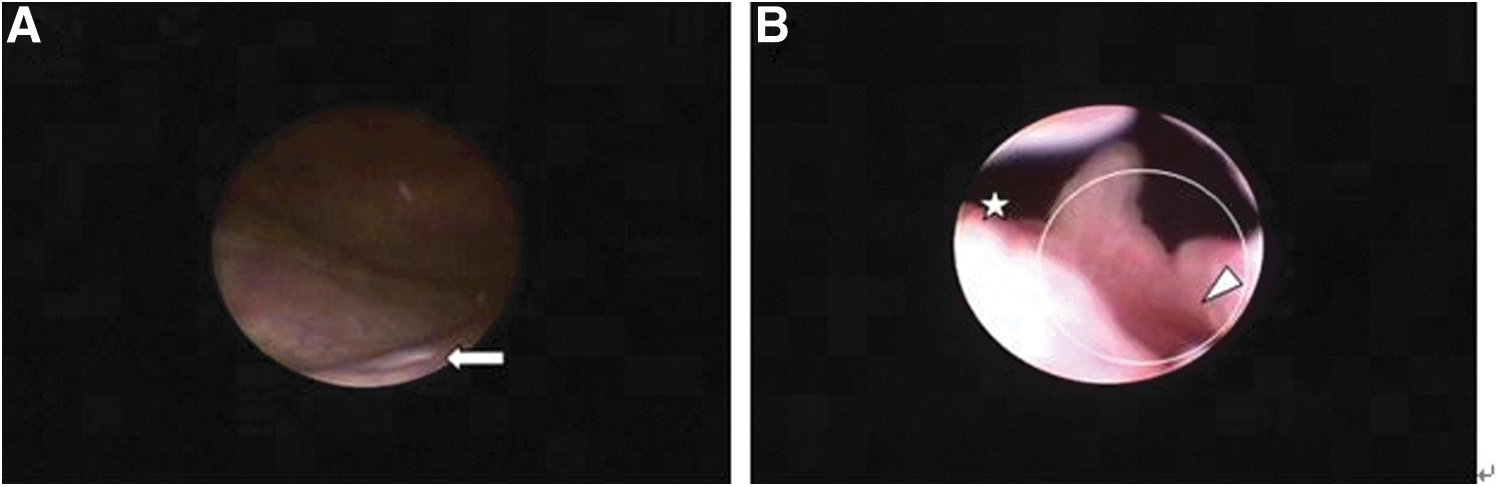
Under general anesthesia, a nasogastric tube was inserted at the beginning of surgery, and patients were placed in the lithotomy position. The location of the ureteral orifices and characteristics of the bladder and ectopic ureter were assessed using cystoscopy and ureteroscopy before performing laparoscopic ureteroureterostomy (Fig. 1). Intraoperative retrograde ureteropyelography was performed to check the course of the double ureters (Fig. 2). Then a 6F open-ended ureteral catheter was inserted into the ectopic ureter using ureteroscopy, and a guidewire was inserted into the normal lower pole ureter.

Complete duplicated ureters in retrograde ureteropyelography. E indicates ectopic upper pole moiety; N indicates normal lower pole moiety.
Surgical techniques of laparoscopic ureteroureterostomy
Before beginning laparoscopic ureteroureterostomy, the position of the patient was changed to semilateral. A urethral Foley catheter was inserted at the beginning of the surgical procedure. Pneumoperitoneum was established using a Veress needle, and an 11-mm camera port was positioned above the upper umbilical margin. Two 5-mm ports for laparoscopic instruments such as an electrosurgical scissor and an atraumatic dissector were inserted at the upper and lateral areas of the umbilicus, respectively. After completion of port insertion, the patient was placed in a moderate semilateral position.
After incision of the Toldt line, the dilated ectopic ureter was easily identified and separated from adjacent tissue using a blunt and sharp dissection. Next, it was mobilized cranially and caudally. The normal lower pole ureter was also identified and mobilized cranially and caudally (Fig. 3). At this time, a third 5-mm port was inserted for traction. A stay suture was placed in the refluxing ectopic ureter to clamp and divide it obliquely. A distal ureteral stump was kept unclipped as low as possible to avoid the development of distal ureteral stump collection and the risk of a pelvic abscess.
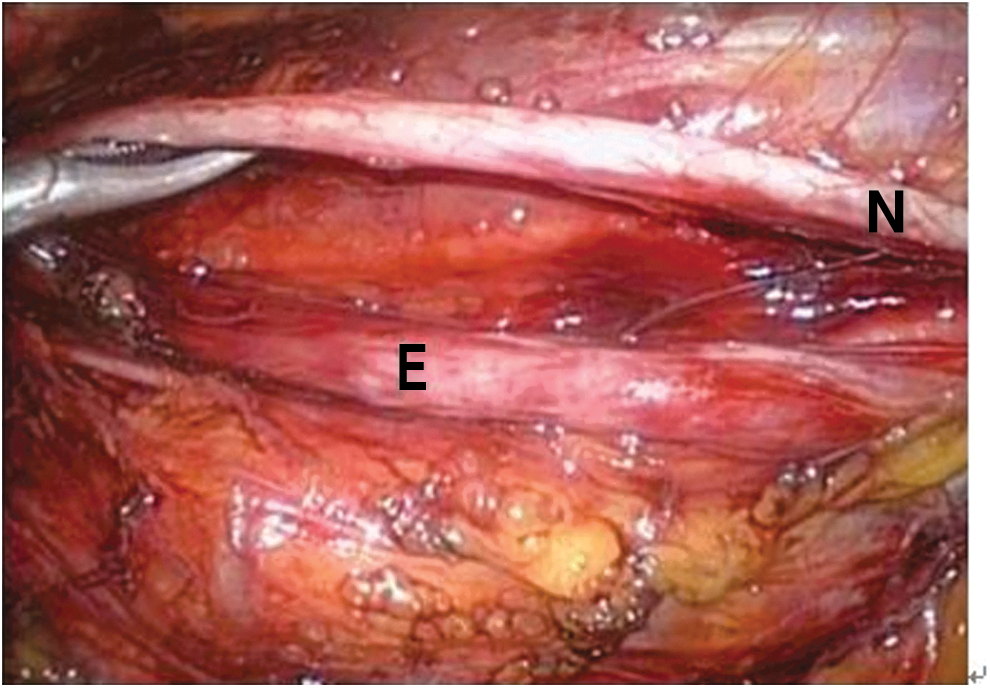
Intraoperative photograph showing normal lower pole ureter and dilated upper pole ectopic ureter. E indicates ectopic dilated ureter; N indicates normal ureter.
If feasible, depending on the size of the dilated ectopic ureter, longitudinal ureterotomy was performed in the normal lower pole ureter. The guidewire that had been placed in the normal lower ureter was moved into the renal pelvis of the ectopic ureter. End-to-side anastomosis was performed in a continuous manner with absorbable polyglactin 4-0 sutures. Before completing suturing, an internal Double-J stent was inserted using a guidewire. The remainder, of the anterior wall was anastomosed in a watertight manner. After the completion of anastomosis, a closed suction drain was placed in the surgical area.
Surgical techniques of transvaginal ureterectomy
After laparoscopic ureteroureterostomy, the patient was placed back in the lithotomy position. An additional ureteral catheter was inserted into the ectopic ureter using cystoscopy. It was considered to enable finding a dilated ectopic ureter more esily through a vaginal small incision. After a weighted vaginal retractor was inserted and the uterine cervix was pulled toward the right and lower direction with tenaculum forceps, a sufficient operative view was achieved. A dilated ectopic ureter was easily identified near the bladder neck by finger feeling. A 2-cm longitudinal vaginal wall incision was performed. Once the ectopic ureteral segment within approximately 1 inch of the bladder neck was freed completely, it was divided and incised with scissors (Fig. 4). After the ureteral segment was dissected vertically, the short ureteral stump adjacent to the bladder neck was closed with polyglactin 3-0 sutures. Then the vaginal mucosa and wall were closed separately. No drain was placed.
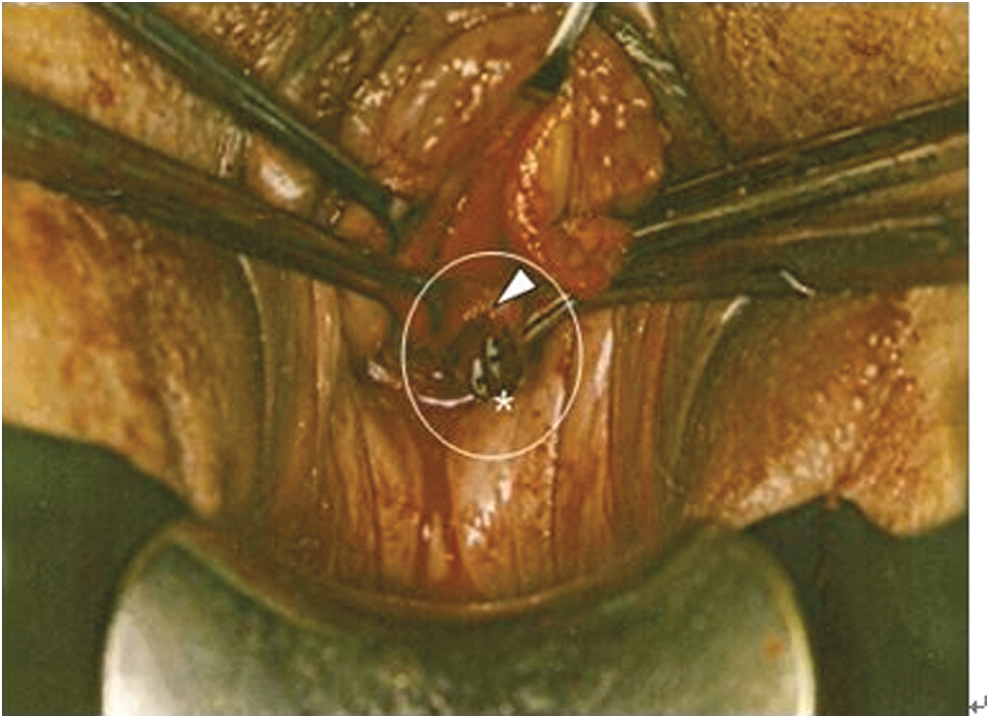
Intraoperative photograph showing ectopic ureteral stump (white arrowhead) containing two ureteral catheters (asterisk) during vaginal ureterectomy.
Results
No intraoperative complications or significant bleeding occurred in all of the patients. The total mean surgical time in four patients was 250 minutes. Mean laparoscopic ureteroureterostomy time was 180 minutes, and transvaginal ureterectomy by vaginal incision was 40 minutes, respectively. Mean blood loss was 150 mL. The urethral catheter was removed 48 hours after surgery, and the drains were removed 1 day after catheter removal.
In the first patient, Clavien grade IIIb postoperative complications including mild urine leak and ureteral stricture in the anastomosed site occurred. The patient presented on postoperative day 6 with abdominal pain and fever. CT demonstrated a mild urinoma. On postoperative day 8, percutaneous nephrostomy (PCN) was performed in the renal pelvis of the normal lower pole moiety and an additional Double-J stent was inserted through the PCN antegradely. In addition, a percutaneous drainage (PCD) tube was inserted for urinoma drainage. On postoperative day 15, the additional Double-J stent and PCD were removed, and balloon dilation was performed after confirming the stricture site by retrograde ureteropyelography. On postoperative day 30, the PCN was removed, and the patient was discharged. An internal Double-J stent that had been placed on the ectopic upper pole moiety was removed after 8 weeks.
In patient 3, there was persistent mild left flank pain at follow-up. Examination failed to reveal an anatomic cause for the pain, and she reported no recurrent urinary tract infections. Her painful symptom gradually resolved after approximately 6 months.
All patients were evaluated by ultrasonography and DMSA scintigraphy for 6 to 12 months. Postoperative imaging in all patients showed a maintenance of function of the upper pole moiety. Postoperative DMSA scintigraphy, however, did not reveal significant improvement in hydronephrosis in all patients (Fig. 5).

The mean length of follow-up was 26.5 months (median 18.0, range 12–78). A follow-up evaluation with history, physical examination, and CT were performed on all patients.
Discussion
Both CDU and refluxing ectopic ureters are common congenital anomalies of the urinary tract; however, they seldom occur in combination. Because there are limited publications reporting on CDU and refluxing ectopic ureters in duplicated collecting systems, the exact incidence is not known.
Many surgical procedures have been introduced for the management of ectopic ureters in patients with CDU. 4,7 Procedures for the management of ectopic ureters can use a bladder level approach or an upper tract approach, depending on the level of the operation. 17 The upper tract approach, such as ureteroureterostomy and heminephrectomy, have the advantage of not damaging the bladder and, thus, can be performed in young patients. 1 The surgical treatment of these patients depends on anatomic features and the degree of renal function in the affected segment of the each patient. If there is a massive hydronephrosis with no function in the parenchyma, heminephrectomy of the affected pole may be selected. 4 –6
If the upper pole moiety function is moderate, however, then ureteroureterostomy may be considered. 7,8 Shelfo and associates 8 reported that end-to-side ureteroureterostomy is a successful technique with a low complication rate for managing CDU. 8 It has been shown that ureteroureterostomy is a safe and effective reconstructive surgical technique for managing CDU. Ureteroureterostomy is one of the surgical techniques available to manage duplex systems with a functioning upper pole moiety. 9 Furthermore, robotic or laparoscopic ureteroureterostomy has recently been reported to be an effective and minimally invasive option. 18,19
Ureteroureterostomy and heminephrectomy are the main techniques that use the upper tract approach, and there have been no clear-cut indications for the decision to perform one over the other. Therefore, this decision tends to be based on surgeon preference. 1 Compared with heminephrectomy, ureteroureterostomy has the advantages of upper pole renal function preservation, and no risk of lower pole damage. It also has the disadvantages of possibly leading to high blood pressure and complications related to anastomosis, however. 1,2 Because there have been only a few reports on ureteroureterostomy with short postoperative follow-up, these risks are difficult to demonstrate.
In our study, we reviewed the data of patients with a diagnosis of CDU who underwent a surgical procedure between 2007 and 2012, and identified six women. Two patients who had poorly functioning upper pole moieties with nonrefluxing ectopic ureters underwent robot-assisted laparoscopic heminephrectomy. Heminephrectomy is surgically indicated for patients with poorly functioning upper pole moieties. The distal ureteral stump was kept open to avoid the development of a distal ureteral stump collection and the risk of a pelvic abscess. Also, we performed end-to-side laparoscopic ureteroureterostomy in four patients. All patients had moderate postoperative outcomes. Although immediate complications such as mild urine leak and stricture in the anastomosed site were noted, no long-term complications were observed, and no further surgical procedures were needed.
In the literature, upper tract approaches may be associated with a risk of urinary tract infection at the residual ureteral stump, often necessitating additional surgery, particularly in the event of a refluxing ectopic ureter. 10 –13 In patients with a refluxing ectopic ureter, ureterectomy would be recommended as low as possible to prevent a refluxing diverticulum and another possible source of urinary tract infection. There were a few reports concerning this complication after using an upper tract approach. Persad and colleagues 10 reported that a dual approach is recommended when complete excision of the kidney and ureter is needed to prevent infection above the vesicoureteral junction. Plaire and coworkers 17 reported that after the treatment of 32 patients with ectopic ureters, 4 (12.5%) needed repeated surgery at the bladder level.
In addition, Lee and colleagues 13 reported that an additional operation was performed in nine (12.2%) patients after proximal ureteroureterostomy, because of the development of a urinary tract infection at the residual ureteral stump. They revealed that, whether noted preoperatively or postoperatively, reflux into an ectopic ureter may be an indicator for residual ureteral stump removal. De Caluwe and associates 11 reported that five (10%) patients needed residual ureteral stump removal after upper pole heminephrectomy. Of these five patients with residual ureteral stump infection, four demonstrated reflux into the residual ureteral stump. Long-term follow-up, however, suggested that the majority of patients who have residual ureteral stumps after upper pole heminephrectomy would not need stump resection. 11,12
In our study, to avoid the above-mentioned approximately 12% repeated surgery and urinary tract infection from retained ureteral stumps, we successively performed transvaginal ureterectomy on behalf of total ureterectomy after laparoscopic ureteroureterostomy and prevented urinary tract infections in four patients with a diagnosis of CDU and refluxing ectopic ureters. The presence of ureteral reflux would dictate the need for removal of the distal ureteral stumps in these patients.
Traditionally, a refluxing ectopic ureter might necessitate total ureterectomy, best performed at the time of ureteroureterostomy, rather than waiting for symptoms to indicate that the procedure is necessary. If total ureterectomy is needed, it is hazardous to resect the entire ureter of an upper moiety because it shares a common wall and blood supply with its normal mate. 14 –16 Therefore, we considered the transvaginal approach on behalf of total ureterectomy for this procedure. Also, considering that laparoscopic ureteroureterostomy is a minimally invasive surgery in relative young women and that impacted lower ureteral stone surgery was performed by a vaginal small incision a few decades ago, 20,21 we decided to perform transvaginal ureterectomy by its small incision after laparoscopic ureteroureterostomy.
During the follow-up periods, we monitored whether there is a concern for future malignancy in excluded ectopic ureter. No malignant change in the ureteral stump was seen in 5 years of CT follow-up.
Although it has been reported that ureteroureterostomy is effective in the preservation of upper pole kidney function, Vates and coworkers 22 reported no difference in postoperative renal function between the ureteroureterostomy group and heminephrectomy group. In our study, postoperative DMSA scintigraphy did not demonstrate a significant improvement in hydronephrosis in four patients who had undergone ureteroureterostomy. Perhaps it is thought that the patients had upper pole kidney function of 30% to 43%, which indicates relatively poor function in the preoperative DMSA scintigraphy.
Conclusions
Our experience have demonstrated that transvaginal ureterectomy after laparoscopic ureteroureterostomy could be a minimally invasive modality. It seems to be a technically feasible and effective option for patients who had CDU with refluxing ectopic ureters.
Footnotes
Disclosure Statement
No competing financial interests exist.