
Abstract
Background and Purpose:
The effect of oral anxiolytics in diminishing patient discomfort and pain perception has been demonstrated in GI endoscopy, percutaneous coronary interventions, and various procedures in the emergency department setting, but has not been prospectively studied in the setting of prostate biopsy. The purpose of this study was to investigate the effect of diazepam on pain perception during and after prostate biopsy.
Patients and Methods:
Sixty patients undergoing prostate biopsy at a single academic institution were enrolled into a prospective, randomized, placebo-controlled study. A questionnaire was administered prebiopsy to determine baseline discomfort and pain history. A visual analog pain scale was used to determine pain associated with each step of the transrectal Ultrasonography-guided prostate biopsy and was administered 20 minutes after biopsy and 1 week later. Responses were compared between groups using the Mann-Whitney U test, Fisher exact test, and Wilcoxon signed rank test as appropriate.
Results:
A total of 60 patients (29 diazepam, 31 placebo) completed pre- and postbiopsy surveys for analysis. The number of cores sampled during biopsy was controlled during analysis and was found to have no correlation with total pain measured. There were no differences between diazepam and placebo groups in age, prebiopsy survey results, immediate and 1 week postbiopsy survey results. There was no difference in the patients' willingness to undergo a repeated procedure in the control and treatment groups. Complications of taking diazepam prebiopsy included drowsiness, chills, and ankle injury.
Conclusions:
Diazepam does not improve patient pain perception immediately after or at 1-week recall after prostate biopsy. Omitting diazepam simplifies the biopsy regimen and allows the patient to drive himself home. Based on these results, routine use of diazepam in prostate biopsy is not recommended.
Introduction
I
Despite the improvements made in this procedure, patients are still subjected to discomfort and pain during prostate biopsy. Recently, modifications in the biopsy technique including increased numbers of biopsy cores, saturation biopsy, and aggressive biopsies performed as part of surveillance protocols have further accentuated the need for improved techniques to control prostate biopsy pain. 5 –9
Oral anxiolytics such as diazepam have been demonstrated to reduce patient perception of pain during gastrointestinal (GI) endoscopy, 10 percutaneous coronary interventions, 11 and various procedures in the emergency department setting. 12 The utility of diazepam before prostate biopsy, however, has never been investigated in a prospective, randomized, double-blind, placebo-controlled trial.
The purpose of this study is to determine whether oral diazepam before prostate biopsy improves patient perception of pain immediately after and 1 week after a prostate biopsy.
Patients and Methods
After approval by the Institutional Review Board, 60 patients undergoing transrectal ultrasonography (TRUS)-guided prostate biopsy were recruited for this prospective, randomized, double-blind, placebo-controlled trial. The indications for biopsy included abnormal digital rectal examination and/or abnormally elevated prostate-specific antigen (PSA) level. Patients >75 years old, with diazepam allergies, requiring narcotics chronically or with a diagnosis of chronic pain syndromes, and those with a history of prostate biopsy were excluded from participation in the study.
The prebiopsy regimen included a 3-day course of oral ciprofloxacin 500 mg every 12 hours beginning the morning before the biopsy and a Fleet enema the morning of the biopsy. Anticoagulants or antiplatelets were routinely stopped 7 to 10 days before biopsy. All study patients were required to be accompanied by a driver because of the possible side effects of cognitive impairment, drowsiness, fatigue, vertigo, and ataxia associated with diazepam.
The physicians performing the biopsy, the staff collecting the pain questionnaires, and the patients were all blinded to the treatment status. All pain surveys were conducted using the 11-point visual analog scale (VAS) (see Index—supplementary data are available online at
Sixty medication bottles were prepared by a pharmacist containing either a 10 mg diazepam pill or a placebo. A random number generator was used to distribute the diazepam and placebo medications to the 60 study subjects undergoing prostate biopsy. Bottles labeled 1 to 60 were given to the patients 1 hour before TRUS-guided prostate biopsy.
All TRUS-guided prostate biopsies were performed using the Hitachi HIGH VISION 5500 ultrasound machine with the UST-675P prostate probe (Hitachi Aloka Medical, Ltd, Tokyo, Japan). In all patients, the procedure was begun by inserting the ultrasound probe into the patient's rectum. Next, 20 mL of 2% lidocaine was injected to the periprostatic neurovascular bundle using a 7 inch, 22 gauge Chiba needle under TRUS guidance in the standard fashion as reported previously. 3 Next, prostate measurements were performed in three dimensions to determine prostate volume. All biopsies were performed with the patient in the left lateral decubitus position. The number of prostate biopsy cores was based on the glandular volume and abnormal findings on physical/sonographic examination and ranged from 13 to 28 (Table 1). The patients' age, PSA scores, TRUS findings, and number of biopsy cores were recorded and compared.
PSA=prostate-specific antigen; TRUS=transrectal ultrasonography.
A pain survey administered 20 minutes postbiopsy evaluated the patients' pain during the various steps of the procedure, including transrectal ultrasound probe insertion, periprostatic anesthetic injection, ultrasonography of the prostate, biopsy of the prostate, as well as the overall pain level postprocedurally. Patients were also asked if they would be willing to undergo a future prostatic biopsy if medically indicated (Index 2—supplementary data are available online at
One week after biopsy, two additional follow-up pain questionnaires were administered. One assessed the patients' pain at the time of contact (Index 3—supplementary data are available online at
Statistical analysis was performed using the SPSS v21.5 for Windows Statistical Software Package. A priori power analysis was performed using the G*Power software. With the standard deviation in each group predicted to be 1 on the VAS according to previous reports, 3,13 and a difference of 2 on the VAS deemed to be a clinically significant improvement in pain, 26 subjects per group were needed to achieve a 95% confidence level. The Mann-Whitney U test was used to compare age, PSA score, TRUS findings, number of biopsy cores, and baseline pain levels preprocedurally, 20-minute postprocedural pain levels, and 1-week postprocedural pain levels between the treatment and control groups. The Fisher exact test was used to compare the rate of patient willingness to undergo repeated biopsy if indicated. Finally, the related-samples Wilcoxon signed rank test was used to compare the patients' recall pain scores at 1 week postbiopsy to their own pain scores 20 minutes postbiopsy. For the preoperative characteristic comparisons, P<0.05 was accepted as statistically significant. The Bonferroni method was used in the statistical analysis of pain levels to account for the multiple comparisons, with P<0.005 deemed statistically significant.
Results
A total of 60 patients were enrolled in the study, with 31 and 29 patients in the control and treatment groups, respectively. Average age, PSA score, TRUS findings, number of biopsy cores and prebiopsy pain scores are shown in Table 1. Statistical analysis demonstrated no difference in any of the prebiopsy parameters between the two groups (Table 1).
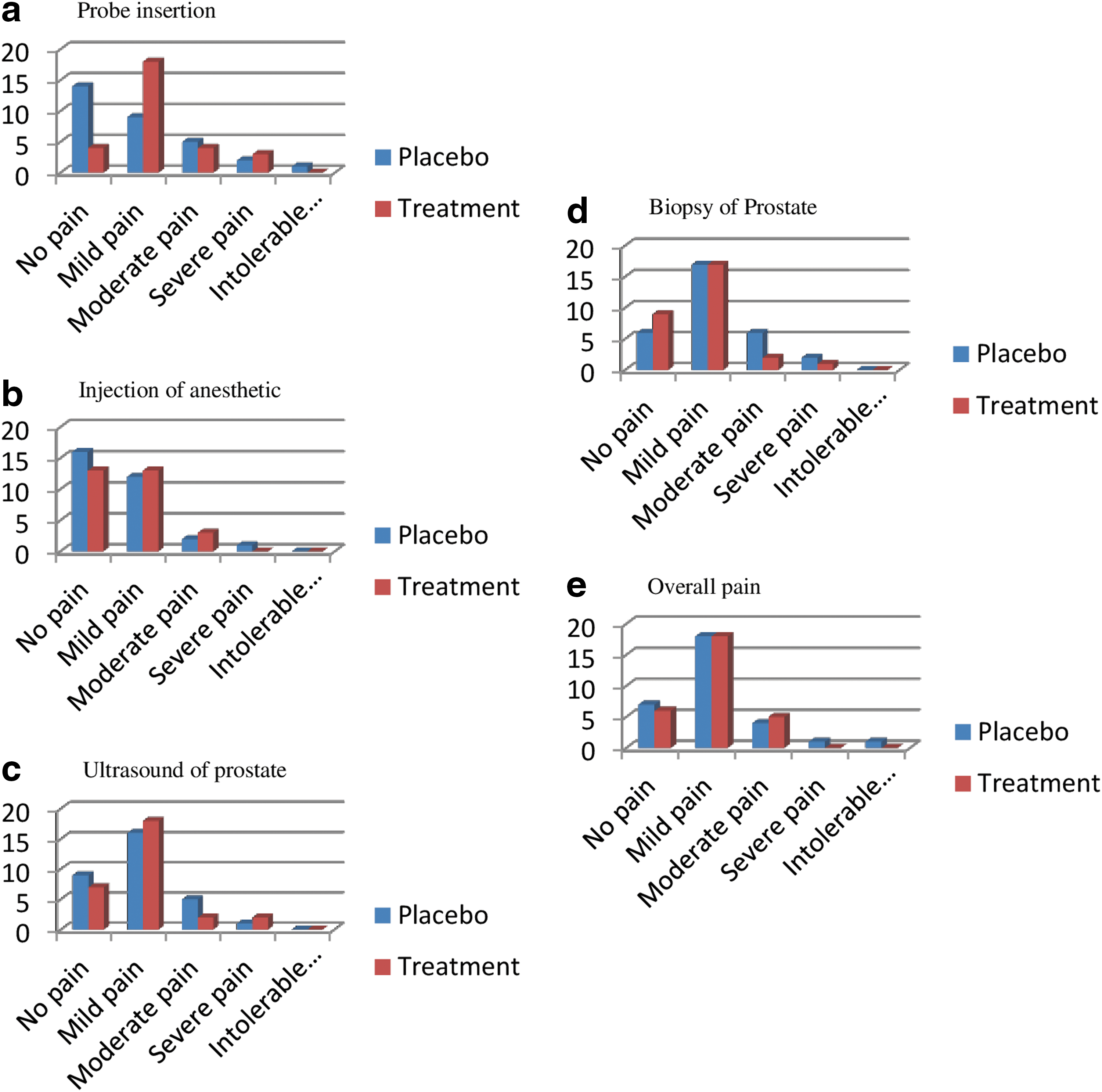
All patients answered the postbiopsy survey 20 minutes after TRUS biopsy. When all patients (n=60) were combined to determine the most painful portions of the procedure, probe insertion (mean 2.19), biopsy (mean 1.98), and anesthetic injection (mean 1.93) were felt to be most painful. The control and treatment groups experienced similar levels of mild pain overall (2.24 vs 2.0 respectively, P=0.886) and with probe insertion (2.06 vs 2.32; P=0.88) (Table 2). In addition, no difference was found in the pain levels associated with anesthetic injection (1.94 vs 1.93; P=0.235), ultrasonography of the prostate (1.26 vs 1.43; P=0.94), or biopsy of the prostate (2.26 vs 1.67; P=0.326) in the control vs treatment groups (Figure 1). More than 90% of the patients in each group expressed willingness to undergo repeated biopsy (90.3% control vs 96.4% treatment; P=0.613).
Immediate postbiopsy visual analog scale score.
Statistical significance with Bonferroni correction: P<0.005.
At 1-week follow-up, the average pain felt by the patients over the last 24 hours was 1 for the control group and 0.21 for the treatment group (P=0.270). There was no difference in pain scores between the two groups in each of the parameters asked.
On the recall survey, the overall pain for the control and treatment groups were 2.09 vs 3.04, respectively (P=0.191) (Table 2). Specifically, the levels of pain for anesthetic injection (2.3 vs 1.86, P=0.885), ultrasonography of the prostate (1.36 vs 1.79, P=0.532), and biopsy of the prostate (2.27 vs 2.75, P=0.47) were similar in the control and treatment groups, respectively. The difference between recalled pain associated with probe insertion in the control and treatment groups (1.52 vs 2.93, P=0.014) trended toward but did not achieve statistical significance. Again, there was a high rate of willingness to repeat the biopsy in the control and treatment groups (100% vs 93% respectively, P=0.389).
The recall pain scores were also compared to the immediate pain scores for both the treatment and control groups (Table 3). Interestingly, patients in both groups generally recalled higher pain scores at 1 week, but no comparison reached statistical significance.
VAS=visual analog scale.
The oncologic outcomes of the biopsies were similar between the two groups. Fourteen patients received a diagnosis of prostate cancer in each group (45.2% control, 48.3% diazepam; P=0.802). There was also no difference in the distribution of clinical stage between the control and treatment arms (P=0.143). Among the patients in the control group with a diagnosis of prostate cancer, five (35.7%) were stage cT1c, seven (50%) were cT2a, and two (14.3%) were cT2c. In the diazepam group, 11 patients (78.6%) were stage cT1c, two each (14.3%) were cT2a and cT2c. In the control group, nine patients had Gleason 6 disease, two had Gleason 7, and one each had Gleason 8 and 9. In the diazepam group, eight patients had Gleason 6 disease, four had Gleason 7, and one had Gleason 8.
Three patients in the control group reported minor side effects including nausea, dizziness, and ataxia, while drowsiness was reported by two patients in the treatment group, and another patient reported chills postprocedurally. In addition, one treatment patient twisted his ankle leaving the biopsy visit resulting in a sprained ankle.
Discussion
The technique of TRUS was first introduced by Takahashi and Ouchi in 1963. 14 Initially, efforts were made to biopsy the prostate transperineally. The pain associated with this procedure restricted its use, however. 2 It was not until 1989 that the first transrectal biopsy of the prostate under TRUS guidance was performed using an 18-gauge needle. 15 Better tolerance was noted with the transrectal approach because of the relative insensitivity of the rectal mucosa. Despite the improvement, 65% to 90% of patients continued to report discomfort with TRUS biopsy. 16 The pain of biopsy is usually attributed to the rich autonomic nerve innervation arising from the prostatic capsule.
In 1996, Nash and associates 3 reported their innovative technique to anesthetize the prostate using injection of 1% lidocaine at the vascular pedicle of the prostate gland under TRUS guidance. The authors reported significantly improved VAS scores associated with treatment from a mean score of 2.9 to a score of 1.6 (P<0.0001). Sixty-eight percent vs 41% of the treatment and control group patients answered affirmatively that they would undergo a repeated procedure, respectively (P=0.05). The initial positive findings for nerve block by Nash and colleagues 3 have been validated subsequently in other studies. 17,18 In these early studies, the mean number of cores biopsied ranged from 4 to 10.
Subsequent to these original descriptions of adjunctive local anesthesia to prostate biopsy, modifications in the biopsy technique have been incorporated into clinical practice including increased numbers of biopsy cores, saturation biopsy, and aggressive biopsies performed as part of surveillance protocols. Unfortunately, the increase in number of biopsy cores is accompanied by increased pain and anesthetic requirement. 18
In an attempt to further reduce the morbidity of prostate biopsy, several drugs have been used in combination with periprostatic nerve blockade for additional analgesia and sedation. Pendleton and coworkers 19 showed that combining oral tramadol and acetaminophen with periprostatic lidocaine injection significantly improved the pain during prostate biopsy. Cesur and colleagues 20 used “walking” caudal anesthesia to help reduce anal tone to facilitate rectal probe insertion and noted improved pain control, perianal anesthesia, and patient satisfaction. The authors noted, however, that placement of the walking caudal necessitates a separate procedure associated with its own morbidities. Peters and associates 21 used propofol in addition to periprostatic lidocaine injection and found that the combination reduced patient anxiety during the procedure.
Previous authors have reported on effects of using the short-acting, rapid-onset intravenous (IV) benzodiazepine midazolam for sedation before TRUS biopsies. 13,22 Shrimali and coworkers 22 used IV midazolam to provide sedation and analgesia and noted favorable results with fewer patients experiencing pain during the procedure. In a prospective randomized trial, Turgut and colleagues 13 noted decreased numbers of patients experiencing moderate or severe pain on the VAS with midazolam administered preprocedurally, although there was no significant improvement in the overall VAS (1.4 for the midazolam group vs 2.0 for the control group; P=0.05. These authors concluded that IV midazolam is an effective way to sedate patients before prostate biopsy and provided added analgesic effect to periprostatic lidocaine injection. The patients who receive IV midazolam, however, need anesthesia monitoring periprocedurally as well as postprocedurally. In the Turgut study, the patients' vital signs were monitored up to 2 hours postoperatively. Together, the perioperative, postoperative anesthesia monitoring and the high cost associated with using IV midazolam make it impractical for routine use in the outpatient setting.
Diazepam is a benzodiazepine that has been shown to act as a muscle relaxant, sedative, and anxiolytic. It produces its effects through interactions with γ-amino butyric acid receptors as well as the benzodiazepine receptors to produce amnesia and sedation. 23 When administered orally, it is rapidly absorbed, has a fast onset of action, and is 100% bioavailable. Peak plasma levels occur at 30 to 90 minutes after oral administration.
Diazepam has been successfully used for upper GI endoscopy and colonoscopy. A meta-analysis reported high satisfaction rate (80%) and adequate patient cooperation (69%) while using diazepam during these procedures. There was also a high rate of willingness to repeat the examination with the same sedation (84%). 10
The use of diazepam before prostate biopsy has been reported anecdotally in the literature. 24 Our study, however, is the first prospective, randomized, double-blind, placebo-controlled trial to investigate using diazepam for sedation and analgesia before TRUS-guided prostate biopsy in naïve prostate biopsy patients.
Several interesting findings were demonstrated in our study. Overall, pain levels (2.24 vs 2.0) experienced by the control and diazepam groups were mild and similar to previously reported VAS scores (0.7–3.0) associated with prostate biopsy performed with local anesthesia injection. 13,25 –31 There was no difference in the pain perception associated with any of the steps of the prostate biopsy or the overall procedure between the placebo and treatment groups on the 20 minute postbiopsy survey. Similar to our study, Turgut and colleagues 13 found no significant improvement in overall pain perception in their prospective randomized study comparing patients receiving IV midazolam prebiopsy with patients receiving periprostatic injection of local anesthetic only (VAS 1.4 vs 2.0).
Our study is the first to our knowledge that reports the VAS score associated with each step of the prostate biopsy. Similar to previous reports, 21,32 our results showed that rectal probe insertion consistently incurred mild levels of pain/discomfort. Moreover, the administration of diazepam preprocedurally failed to improve the VAS score on rectal probe insertion (2.06 in control, 2.32 in treatment, P=0.88). This finding disproves previous authors' postulate that the myorelaxative and antianxiolytic properties of benzodiazepines will loosen anal tone, thus reducing discomfort experience on rectal probe insertion. 13
The recall VAS survey was also designed to assess the amnestic effects of diazepam. Interestingly, there was a consistent trend of increasing levels of pain reported by patients in the diazepam group on the 1-week follow-up compared with the 20-minute postbiopsy survey. None of the comparisons reached statistical significance, however. Nonetheless, these results demonstrate the ineffectiveness of diazepam to provide antegrade amnesia.
Overall, very few adverse events were reported by patients in the treatment group, consistent with the relative safety of prescribing diazepam in the outpatient setting. One patient suffered a sprained ankle, however, that can be partially attributed to the drowsiness induced by diazepam as he stepped off the curb leaving the biopsy appointment. A high percentage of patients in both groups also indicated willingness to undergo biopsy on the 20-minute as well as the 1-week postbiopsy surveys.
Although diazepam appears to have a low side-effect profile, our study suggests that there is no added benefit compared with periprostatic nerve block alone before TRUS prostate biopsies and, therefore, routine use of diazepam cannot be recommended.
Despite being a prospective, randomized, double blinded, placebo-controlled trial, there are some potential weaknesses in this study. Although not specifically validated to assess pain after TRUS prostate biopsies, the VAS has been previously used to measure pain in this specialized situation. 3,13,21,25,29,31 Because of varying patient pathologic findings at the time of the biopsy, there were differences in the exact number of biopsies performed. When the data were studied using a Pearson correlation analysis, however, the number of biopsies taken within the range seen in this study did not affect pain outcomes.
Another weakness of this study is that only prostate biopsy naïve patients were included in the study and subsequently the effect of diazepam on repeated biopsy cannot be determined. It was thought that a previous biopsy could cloud the patient's perception of this single biopsy event and subsequently that patients with a previous biopsy should be excluded. Because patients with chronic pain syndromes and narcotic dependence were excluded in this study, it is not possible to determine the effect of diazepam in this subgroup. Future studies may be designed to specifically assess the benefits of administering diazepam before prostate biopsies in these subgroups. For the general population undergoing prostate biopsies, preprocedural diazepam does not seem to provide additional benefit to the local anesthesia routinely provided before biopsy.
Finally, the power analysis was performed using a predicted standard deviation of 1 for the reported pain values based on previous reports. 3,13 The actual standard deviations obtained during the study were higher (Table 2), thus increasing the risk of missing a statistical difference between the two groups. The mean differences in primary and secondary outcomes between the two groups were small, however, such that a clinically significant difference was unlikely.
Conclusion
Our study presents the first prospective, randomized, double-blind, placebo-controlled trial investigating the effects of diazepam used before TRUS-guided prostate biopsy. This study demonstrates that diazepam does not decrease pain perception or improve patients' willingness to undergo repeated biopsy. For this reason, routine use of diazepam cannot be recommended before prostate biopsy.
Footnotes
Acknowledgment
The authors would like to thank Udochukwu Oyoyo for his assistance with statistical analysis.
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.