
Abstract
Purpose:
We present our experience in the design and development of a training program in laparoscopic radical prostatectomy (LRP), and the validation of the first steps of the program by objective measurement of the attendants' skills improvement and subjective evaluation of its contents.
Materials and Methods:
Our training model on LRP has a total duration of 42 hours, divided in two modules of 21 hours each, performed 1 month apart. Data included in the present study were obtained from the first module of our course. It begins with acquisition of basic knowledge in ergonomics and instrument concepts, after which the attendants develop essential laparoscopic dexterities through the performance of hands-on physical simulator tasks. During the second and third day, urologists performed urethrovesical anastomosis also in the physical simulator. Attendants' skills improvement was measured during the first module by registering surgical times and suturing quality of the anastomosis, the latter by means of a leak test. At the end of the training program, a subjective evaluation questionnaire on the different didactic and organizational aspects was handed out to the attendants.
Results:
By comparing first and last anastomosis, we observed a significant decrease in surgical times (minutes) (T1 40.1±4.6 vs T6 24.01±3.34; P≤0.005) and an increase in intraluminal leak pressure (mm Hg) (T1 8.27±7.33 vs T6 21.09±6.72; P≤0.005). We obtained a highly positive score on all questions concerning the different topics and techniques included in the training program (≥9 points over 10). Regarding the attendants' self-assessment of acquired abilities, 78.3% considered themselves capacitated to perform the trained procedures on patients.
Conclusions:
Training obtained during the first module of our training model significantly decreased performance times for ex vivo urethrovesical anastomosis, simultaneously increasing its quality. In addition, validation of the training model was also demonstrated by the highly scored evaluation resulting from the attendants' assessment.
Introduction
S
Laparoscopy presents these advantages, but it also has various drawbacks, which include the need for fine instrument manipulation through rigid and fixed entry ports, monitor guided bidimensional images with loss of haptic sensation and depth perception, and evident difficulty in eye-hand coordination. The combination of all these aspects leads to the demand of completion of a learning curve, which should not be addressed directly on the patient so as not to increase surgical times and complications. 6 –13 This has constituted from the beginning one of the main limiting factors for the implementation of laparoscopy in all fields of urologic surgery, especially when we consider reconstructive procedures.
An ample description of regulated training programs in laparoscopic surgery exists, usually stating marked improvements on surgeons' basic and advanced skills, reducing learning curves and clinical errors in the daily surgical practice. 14 –16 In the same manner, the number of specialized centers providing laparoscopic courses and specialist qualifications is continuously increasing. 17 In this sense, the British Association of Urological Surgeons defined the guidelines for the regulation of laparoscopic surgery training, combining didactic and expert tutored essential content. 18 It is thus recommended that specific laparoscopic training programs be included in the urology residents' curriculum. A recent study, however, showed that only 27% of the European residents in urology have access to a standardized laparoscopic surgery training program. 19
Laparoscopic radical prostatectomy (LRP) is considered one of the more demanding techniques for urologists, with the urethrovesical anastomosis constituting the most time-consuming step, and increasing the surgical learning curve. 20 Our center has developed a training model with modules focused both on the physical simulator and animal model for the acquisition of essential skills in LRP. The compartmentalization in two separate modules favors a gradual learning process for the attendants, centered on the acquisition and consolidation of urethrovesical anastomosis skills.
With the present study, we aim to demonstrate the results of our experience in the design and development of a training program in LRP and the validation of the first stages of such model.
Material and Methods
Data included in the present study were obtained during a course in LRP, which took place at our center in 2013. Sixteen urologists with different previous experience levels completed this training program.
Description of the training model
The proposed training model, with a total of 42 hours, is structured in various phases or levels, in accordance with the learning steps defined by Usón and associates. 5 Total duration of this training activity is divided in two main modules of 21 hours each, which are performed 1 month apart.
Module I
Following the rules included in Level 1 of Usón's training model, this module is centered on the hands-on practice of basic laparoscopic tasks performed on the physical simulator SIMULAP®, with the final objective of acquiring suturing abilities of urethrovesical anastomosis. The program starts with basic theoretical knowledge of laparoscopic equipment and most commonly used instruments, as well as the explanation of different guidelines for ergonomic body positioning and instrument use. This module also includes the performance of different maneuvers on SIMULAP, with special focus on laparoscopic cut, dissection, and, particularly, suturing maneuvers.
The learning sequence on the simulator begins with inorganic tissues in which cutting tasks are performed on a series of templates designed at our center that allow for the use of both hands in increasingly difficult exercises. Once these initial tasks are correctly performed, the attendants pass on to organic tissues and perform more advanced techniques of dissection and intracorporeal suturing. Last, and during the second and third day of the course, the attendants perform urethrovesical anastomosis on porcine ex vivo urinary organs (bladders, prostates, and urethras) (Fig. 1).

Physical simulator SIMULAP®, developed at our center for laparoscopic surgical training, using porcine ex vivo bladders (including prostate and urethra).
The first anastomosis are performed with the laparoscopy tower placed in front of the surgeon (“comfortable position”) (Fig. 2A). After the fourth “comfortable” anastomosis, the tower is set in the standard clinical position by displacing it to the feet of the surgical table, forcing the surgeon to mimic the necessary positioning when operating on real patients (“uncomfortable position”) (Fig. 2B). All anastomosis are considered complete when a total of eight interrupted sutures are performed, with four placed on the posterior side and four on the anterior surface. All attendants are instructed to begin from the posterior side, placing each suture according to the following hourly positioning: First suture at 5 o'clock, second suture at 7 o'clock, third suture at 4 o'clock, and fourth suture at 8 o'clock. After the posterior side is completed, they proceed to the anterior surface, placing the interrupted sutures at 10 o'clock, 2 o'clock, 11 o'clock, and finally at 1 o'clock.

Detail of the attendants performing urethrovesical anastomosis in comfortable
Module II
This module also lasts for 21 hours and takes place 1 month later than Module I. It is centered on the practice of LRP on an animal model, included in Level 2 of the training model described by Usón and associates. 5 Attendants start by performing two “uncomfortable” urethrovesical anastomosis on the physical simulator, as described above. The remainder of the second module entails performance of several LRPs on a porcine animal model, applying the surgical technique described by Usón and colleagues. 21
During the entire hands-on practice, attendants are constantly tutored by surgeons of renowned expertise. Before each task, didactic video sequences of compared anatomy and the step-by-step surgical technique are shown. Similarly, at the end of each day, small theoretical sessions are included, so that attendants learn about the most adequate surgical protocol and possible complications of an LRP.
In the last phase of the training model, 5 and although not included in the course program, the attendant should apply acquired knowledge to the human patient, operating under supervision of a certified expert during the earlier procedures. This way, attending expert tutors provide each attendant with the possibility of completing an additional training period in their work centers.
Validation of the training model
During the first module, we registered total completion times of six hands-on simulator urethrovesical anastomosis. For better understanding of the validation method, we numbered these anastomosis and made the following correspondence: T1, first comfortable anastomosis; T2, fourth comfortable anastomosis; T3, first uncomfortable anastomosis; T4, fourth uncomfortable anastomosis; T5, last anastomosis performed in the comfortable position during the last day of the course; and finally T6, last anastomosis performed in the uncomfortable position during the last day of the course.
Also, on the same urethrovesical anastomosis, we performed an analysis on suturing quality by performing a leak test at the end of the procedure. This test is completed by immersing the ex vivo porcine bladder in saline and insufflating it with CO2 with the help of a mechanical insufflator and determining the intraluminal pressure at which the first gas bubble is released at the suture line.
At the end of the first module, the attendants were handed an anonymous inquiry for the subjective assessment of the different didactic and organizational aspects of the course.
Statistical analysis
All statistical analyses were performed with statistics software SPSS 15.0 for Windows (SPSS Inc., Chicago, IL). Descriptive statistics for time and leak test variables were obtained by calculation of characteristic parameters: Average, standard deviation, and maximum and minimum values.
In every case, a Kolmogorov-Smirnov test was performed to determine the normal distribution of the samples. Because this condition was verified in all cases, a factorial analysis of variance test with Bonferroni post hoc was performed to compare between tests, with statistical significance set at P<0.05.
Results
Demographic data
Our study sample was composed of 16 urologists, 11 male and 5 female, with an average age of 33.7±5.2, and included 7 urology residents and 9 urologic staff doctors. Of the attendants, 100% declared that they had little experience with the use of physical simulators and none with virtual reality simulation. Regarding performance of laparoscopic procedures, 37.5% had performed less than 50 surgeries as a camera assistant, while all other attendants declared that they had no experience.
Surgical times
The evolution of urethrovesical anastomosis total completion times registered at different study times is depicted on Fig. 3A. On the first urethrovesical anastomosis (T1), we obtained an average completion time of 40.12±4.67 minutes. On the fourth anastomosis (T2), we observed a decrease without statistical significance in completion times (30.61±4.38 minutes) when compared with T1.

Graphic representation of obtained results at the different study times.
A nonsignificant increase in average completion times was observed at T3 (first “uncomfortable” anastomosis). Nevertheless, in the last three study times (T4: 25.44±8.66 min; T5: 28.81±7.88 min; T6: 24.01±3.34 min), there was a marked decrease in surgical times with significant differences in every case (P≤0.005) when compared with T1.
Leak test
The variation of the urethrovesical anastomosis intraluminal leak pressures over time is reflected on the curve of Fig. 3B. On the first three tests, we obtained similar CO2 pressure values (T1: 8.27±7.33 mm Hg; T2: 9.45±6.87 mm Hg; T3: 8.72±6.10 mm Hg), with no statistical differences observed between them. On T4, we observed a more evident increase in intraluminal leak pressures (15.54±6.33 mm Hg), but still without statistical significance compared with T1. In the last two study times, leak pressures gradually increased (T5: 20.63±4.54 mm Hg; T6: 21.09±6.72 mm Hg), with significant differences (P<0.005) compared with T1.
Subjective evaluation questionnaires
All attendants filled in the subjective evaluation questionnaire at the end of the first module of the training program (100% response). The different topics and techniques included in the program obtained a very positive score (more than 9 points of 10), as can be observed in Table 1. The highest rated aspect was the practice of urethrovesical anastomosis on the simulator (9.89±0.51). On the other hand, the topic with the lowest obtained score was the cutting task completed on a predrawn template (9.09±0.44).
Of the attendants, 93.61% considered physical simulators a useful tool for the acquisition of basic skills before the completion of surgical procedures on the animal model (Fig. 4). On the self-assessment questions, 78.33% of attendants considered themselves able to apply the learned techniques on the human patient.
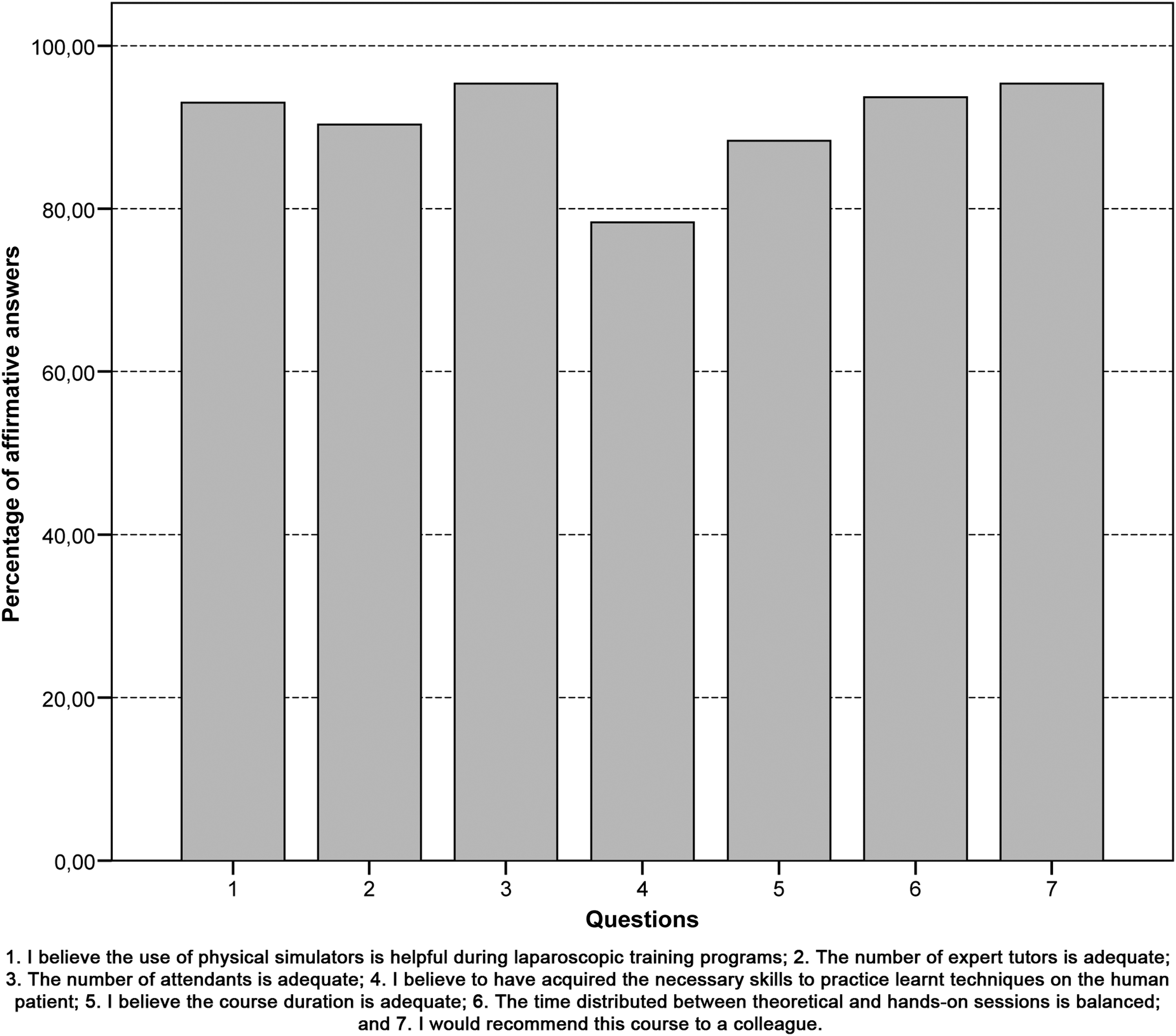
Evaluation of organizational and didactic aspects of the training program.
Considering organizational aspects of the course, 88.5% of attendants were in agreement with the duration of the course, while 11.5% thought it should be extended. Furthermore, 93.69% found the balance between theoretical and hands-on sessions correct. Lastly, 96.83% stated they would recommend this course to other urologists, and 95.62% considered that the number of tutors in the wet lab was balanced and correct (Fig. 4).
Discussion
With the present study, we aimed to demonstrate the results of our group's experience in the design and development of a training program for LRP. Also, we proposed to complete a preliminary validation of the first phases of the program through a series of self-assessment steps completed by the attendants at the XV Course on LRP, as well as an analysis of the degree of skills acquisition during the first module of the course. Obtained results showed a very positive evaluation of the different didactic and organizational aspects of the training model, as well as a significant decrease in average completion time, along with a significant increase in the performance quality during the completion of urethrovesical anastomosis.
The main limitation of the performance of most laparoscopic procedures is usually related to reconstructive maneuvers, as these imply the use of and ability in advanced intracorporeal suturing techniques. 22 Thus, an adequate training model is compulsory for the safe application of procedures such as radical prostatectomy on the human patient. Today it is fully accepted that minimally invasive surgical training in laparoscopy must begin by hands-on practice on inanimate models, with physical simulation constituting an essential tool in these first training steps. 23,24 The use of ex vivo animal organs on physical simulators entails numerous advantages, which include low cost and dissection maneuvers similar to those on live tissue. Moreover, physical simulators provide an ample space, without the need for the establishment of pneumoperitoneum, where the ex vivo organs can be placed in adequate anatomic positioning for the performance of various procedures and surgical maneuvers.
Based on these assertions, we determined that 55% of wet lab hands-on practice was to be performed on organic ex vivo tissues placed inside the physical simulator SIMULAP®, developed at our center. This box trainer allows the surgeon to practice on inorganic as well as organic tissues and has previously been demonstrated to have constructive validity. 25 It provides all course attendants with a safe platform for the acquisition of basic laparoscopic skills and specific abilities, as in the case of urethrovesical anastomosis, reducing the number of errors during hands-on animal model procedures. This led to a very positive attendants' evaluation, of more than 9 points over 10, regarding the different hands-on simulator tasks. Also, at the end of the training activity, 93.61% of attendants considered that the use of physical simulators constituted a helpful step in the acquisition of basic laparoscopic skills. These results thus present evidence regarding general acceptance toward the use of these tools among novice urologists.
With the results obtained in this study, we saw that with the completion of the first module of the described training model, attendants significantly reduced surgical times on the simulator. This reduction has also been observed in other published studies that have similarly focused on the practice of urethrovesical anastomosis on a simulator during regulated training. 26,27
Like Frede and coworkers, 26 we determined the quality of each anastomosis by means of an intraluminal leak pressure at suture level. To perform the leak test, we submerged the bladder and anastomosed urethra in saline and performed a controlled insufflation with CO2. We registered the pressure value at which the first bubble exits the anastomosis to define this objective assessment parameter. In our analysis, we observed a significant increase in the quality of the urethrovesical anastomosis at the end of the first module of the training program.
Once all basic tasks were completed on the simulator, the development of more advanced laparoscopic skills, such as vascular dissection, demand the use of animal models that provide a more realistic scenario for the different clinical situations. 10,15,28 Thus, on our training model, we included a second module of hands-on animal model practice for LRP. We opted for the porcine model after taking into consideration anatomic similarities to the human patient, so that the training and the real surgical scenarios were as alike as possible, and also availability of the species. This second module takes place a month after the first phase, which is supported by studies that state the benefits of distributed training over several hands-on sessions over a large period, compared with intensive or massive training. 29 –31
We agree with these statements and consider that the learning of a complex procedure such as LRP is more effective if there is a gradual evolution from the initial hands-on simulator phase followed a month later by the practice on an animal model. Thus, we prevent fatigue and weariness resulting from a more intensive training program that might limit the attendants' learning ability, and allows for the acquisition of greater surgical dexterity.
As described previously by other authors, 13,32,33 our training model follows a steady ascending progression regarding difficulty of the laparoscopic task—i.e., starting with basic coordination, cut and suturing exercises for the development of psychomotor skills, and progressing to more specific and more difficult techniques such as urethrovesical anastomosis. Similarly, and with the intention of increasing the difficulty level, the first anastomosis are performed with the laparoscopic tower in front of the attendant (“comfortable” position), and at the fifth repetition, the tower is displaced toward the end of the surgical table similar to the operating setup for human patients (“uncomfortable” position). This difficulty increase was reflected on our results, with the prolongation of surgical times and a mild reduction in leak pressure from the fourth and last “comfortable” to the first “uncomfortable” urethrovesical anastomosis.
In our LRP training course, we consider that one of the undeniable abilities needed for the suturing of impermeable anastomosis is the correct placement of the needle, adapting it to the different positions needed when following the adequate suturing pattern. 34 Several systems have been used, 28,35 but we believe that the completion of eight interrupted sutures allows for the quick learning of the correct needle orientation and the performance of a gas-tight urethrovesical anastomosis in the early stages of learning. When the attendants show complete mastery on the interrupted anastomosis suturing pattern, they pass on to the more clinically applicable continuous pattern with two united sutures with a needle at each end. 36
Recently, a report was published stating that a regulated course model can effectively relaunch and consolidate the laparoscopic approach, in referral as well as local hospitals. 16 Our results are in accordance with this study, because 78.33% of attendants accounted themselves qualified to perform these techniques on human patients. The usefulness of this self-assessment, however, is not absolutely trustful because significant differences are found if these scores are compared with those obtained by an expert surgeon for the same procedure, 37 and it should be remembered that novice surgeons tend to overrate their abilities. 38 On future studies, we will aim to determine to what extent the attendants have started to apply these techniques for the benefit of their patients in their work centers.
The number of urethrovesical anastomosis completed by the attendants during the XV Course on LRP (8–10 on simulator, 2–4 on animal model) should not be considered sufficient for the application of the LRP technique on the human patient, because some authors state that at least 25 anastomosis on a simulator are needed for the safe completion of the surgical procedure in fewer than 5 hours. 39 We agree with this evidence, and thus advise the presence of physical simulators in every medical center so that surgeons can consolidate the abilities acquired during this type of training course.
One of the limitations in our study concerns the lack of predictive validation of the training model, which could have been achieved by determining the correlation of the performance of urethrovesical anastomosis on the simulator with those performed 1 month later on an animal model. This would have determined the degree of skills transfer from the simulation to the in vivo model. Similarly, we did not complete an evaluation of the cognitive abilities before and at the end of the course. Both aspects will be taken into account when we complete the assessment of the training course's second module.
Conclusions
Results obtained in this study during the first module of our training model, which included hands-on sessions completed exclusively on the simulator, showed a significant decrease in urethrovesical anastomosis performance times, with a simultaneous increase in suture quality. It has allowed us to determine the validation of the designed training model by obtaining a high scored assessment and showing an increase in the attendants' self-confidence for the performance of these techniques in their daily practice.
Footnotes
Acknowledgments
The authors are especially grateful to the Laparoscopy Unit and MISCJU's personnel for their scientific and technical assistance.
Disclosure Statement
No competing financial interests exist.