
Abstract
Objective:
Laparoscopic surgery can be harmful to surgeons requiring a prolonged learning curve due to significant ergonomic drawbacks. Based on preliminary clinical experience, we present an experimental evaluation of the second-generation ETHOS™ operating chair by comparing it with two different operating positions of conventional laparoscopic pelvic surgery.
Materials and Methods:
The ETHOS operation platform consists of a seat like a saddle and five more parts that can be adjusted individually to support the surgeon's trunk and extremities. This operation platform was tested in 30 trainees who performed three standard suturing exercises in a pelvitrainer, approximating a linear and a U-shaped incision, made on the skin of a chicken leg, and completing an urethrovesical anastomosis, on a pig bladder specimen model, using interrupted sutures. The trainees performed each exercise in standing laterally to pelvitrainer (torero position) vs standing behind pelvi-trainer and sitting on ETHOS. The mean values, from all times and for each exercise and position, were documented, and the participants filled out a validated questionnaire focusing on ergonomic issues.
Results:
There were no significant differences among the different training modalities, in step 1 and step 2. However, in step 3, which mimics the urethrovesical anastomosis, the mean times were statistically significant significantly less by using ETHOS (p<0.0001). The mean times of training in step 3 were 41.2 minutes in the behind the camera position, 49 minutes in torero position, and 39.7 minutes by using ETHOS. The position that was maintained, during the exercises, was mainly responsible for the improvement noted in the ergonomic scores.
Conclusions:
The new operating platform (ETHOS chair) can significantly improve ergonomics in laparoscopy particularly concerning difficult steps like intracorporeal suturing. This may also improve the urethrovesical anastomosis times in a clinical setting.
Introduction
L
Only recently, ergonomics entered the field of laparoscopic surgery 3,6 as surgeons began to notice that they operated under nonergonomic circumstances. Important parameters, like stress and fatigue, can negatively influence the quality of the operation. 7 Even more, due to its evolution, laparoscopy could be applied in more complicated procedures, leading to increased procedure and anesthesia times. As a result, the negative effects of a nonergonomic posture, the chronic limited body movement without weight shifting, and the nonergonomic design of different surgical instruments, became more apparent, 8 especially when performing complex pelvic procedures such as a laparoscopic radical prostatectomy. 7
Based on previously published preliminary clinical experience using the prototype, 9,10 we present the experimental evaluation of the second-generation operating chair (ETHOS™). This platform is designed to improve the ergonomics of laparoscopic procedures, by comparing it with the two different conventional laparoscopic positions during laparoscopic suturing and vesicourethral anastomosis, in a training room setting.
Materials and Methods
The second-generation ETHOS ergonomic operating platform
The main individually adjustable accessories of the surgical chair (ETHOS-platform, ETHOS-Surgical, Portland, USA) include a seat like a saddle, a chest support, two armrests, and footrests (Fig. 1). A motorlift, remotely controlled, adjusts the height of the seat in a range of 106–152 cm. and allows advancement of the chair in a range of 46 cm. The seat moves automated back and forth each in 15 cm range. The distance between the footrests is 91.4 cm. The open straddle reaches a 53 cm of length and allows an optimal docking to the operating table. The chair is located during pelvic laparoscopic operations over the patient's head. In the training room setting, the chair simply approximates the training box and is adjusted according to the body shape of the trainee.
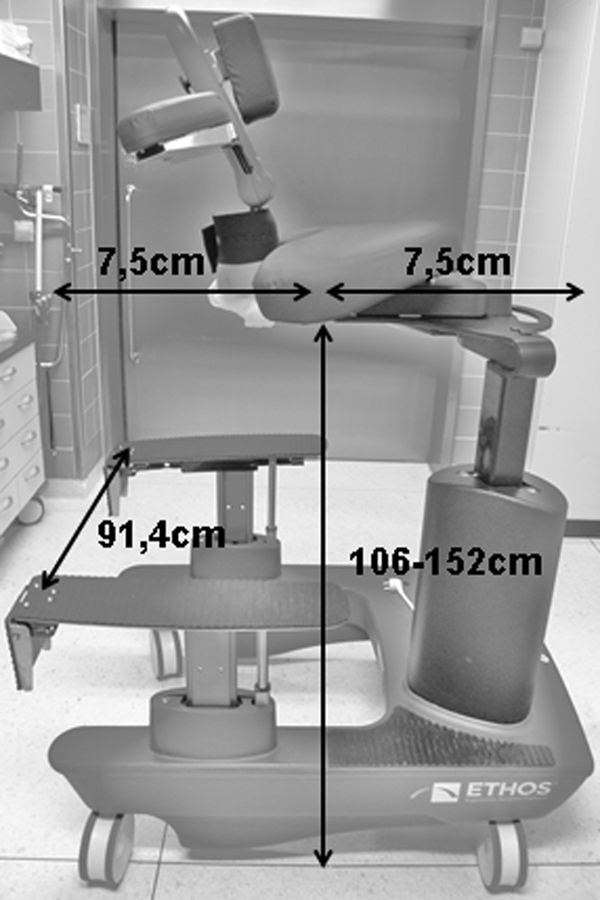
The main individually adjustable accessories of the surgical chair (ETHOS™ Platform, ETHOS Surgical, Portland, USA) include a seat like a saddle, a chest support, two armrests, and footrests. The height and back and forth moves of the seat are adjusted and remotely controlled with an electric motor.
Experimental evaluation in the training room setting
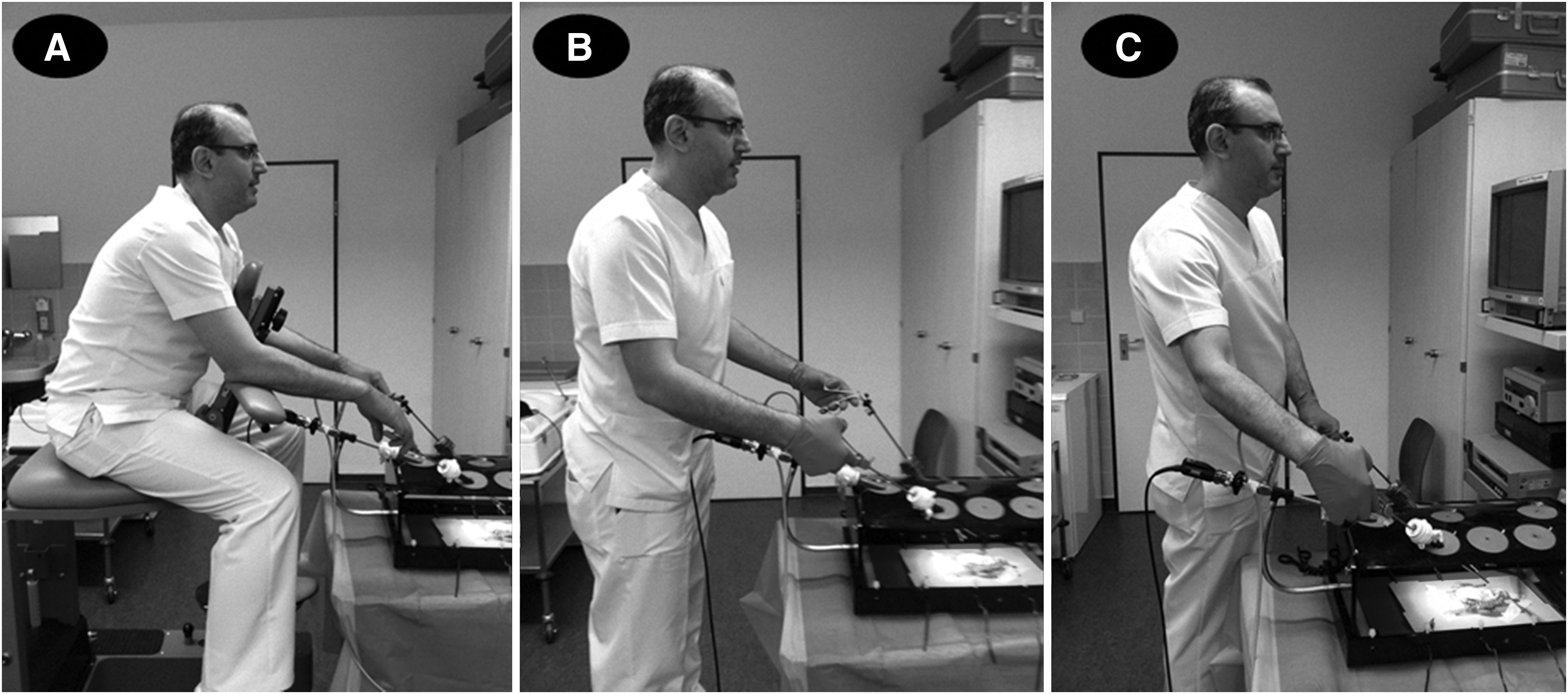
Thirty trainees (clinical fellows), with a similar laparoscopic training level and during their first training month, were included in the study. The trainees performed the following three steps of the standardized Heilbronn laparoscopic training program 11 in three different positions, respectively; standing behind the pelvitrainer, standing laterally to the pelvitrainer (torero position), and sitting (ETHOS position) (Fig. 2A–C).
Training in different positions:
Step 1: Approximating a 5 cm incision made on the skin of a chicken leg using five interrupted sutures (Vicryl 3/0 SH needle).
Step 2: Approximating a U-shaped incision made on the skin of the chicken leg, using five interrupted sutures (Vicryl 3/0 SH needle).
Step 3: Completing a bladder to urethra anastomosis on a pig bladder specimen model by placing seven separate sutures (Vicryl 3/0 SH needle) between the urethra and bladder neck.
Each exercise was performed five times, and the average time was calculated. Primary results of the parameters were time to accomplish the exercise and quality of performance (controlled by ASG and JTK). The trainees filled, by the end of each step, a validated questionnaire that focused on ergonomic issues (musculoskeletal discomfort) (Table 1).
 no complaints
no complaints little pain
little pain 2
2 3
3 4
4 severe pain
severe painStatistical significant p-value.
The Statistical Package for the Social Sciences (SPSS) for Windows 16.0 (SPSS, Inc., Chicago, IL) was used for statistical analysis. The independent-samples t test was used to compare measurable values. The one-way ANOVA test was used to compare the mean values. Statistical significance was accepted as p<0.05.
Results
Evaluation of times to accomplish each step
The comparison of the time periods for the three different steps and in the three different positions is summarized in Table 2. There was no significant difference in step 1 and step 2 among groups (Table 2). Step 3 was mimicking urethrovesical anastomosis. Also, in step 3 (urethrovesical anastomosis), no significant difference was noted between the standing behind the pelvitrainer position and the torero position (41.2 vs 49 minutes; p=0.29). However, the difference became significant when trainers sat on the ETHOS chair (39.7 minutes, p<0.0001; Table 2).
Statistical significant p-value.
Evaluation of questionnaires
The musculoskeletal complaints were significantly less after ETHOS-assisted laparoscopic training, when these were compared to training in conventional laparoscopy positions (Table 3) Ergonomic parameters like musculoskeletal pain, neck pain, shoulder stiffness, hand pain, wrist stiffness, back and leg pain greatly improved with ETHOS. The ergonomic platform offers an optimal sitting position during the procedure. The armrests provide stability and better control of the instruments during suturing and suppress a possible tremor. The chest support secures and stabilizes the sitting position and the direct close view to the monitor. The total ergonomic scores and statistical analysis are shown in Table 3.
Statistical significant p-value.
Discussion
Studies concluded that laparoscopic surgical modalities cause greater strain on the surgeon's body than open surgery, and surgeons suffer from high levels of mental and physical stress during laparoscopic operations. 2,7,8 Park et al. reported that 87% of surgeons who regularly perform minimally invasive surgeries suffer from symptoms of physical pain or discomfort. 12
The energy expended to control laparoscopic instruments can be six times greater compared with that needed for open surgery. 13 Moreover, during laparoscopy, surgeons stay for an extended time in a standing and fixed position, which is determined by the trocar placement. This may lead to a static head, neck, and spine strain, when looking at the screen. In addition, the surgeon suffers from pain or stiffness of the joints of the knee, foot, and shoulder. 2,4,6 –8,12 Some of these factors contribute to a nonergonomic situation during laparoscopy and might be positively influenced by a surgical platform such as an operating chair.
The precise measure of the physical stress to which, every time, a laparoscopist is subjected appears to be more than complicated. A variety of modern techniques have been used, most of which are not really applicable in everyday clinical practice. 4,14 Thus, until now, ergonomic studies are mainly performed in a dry laboratory setting. Undoubtedly, although being subjective, validated questionnaires are the only practical tools in evaluating physical stress during laparoscopy. In a survey based on questionnaires sent out to surgeons performing laparoscopic surgery, 56% of them reported back, neck, hand, and lower extremity symptoms. 7 Similarly, in our study group, the predominant complaints, during the torero position, were musculoskeletal, back, and leg pain.
The use of an ergonomic chair, as a tool in laparoscopy, was first introduced by Schurr et al. 15 In 2007, Albayrak et al. presented the first ergonomic platform consisting of foot pedals and remote control technology. 16 By applying electromyography, the authors showed a significant reduction of erector spinae, semitendinosus, and gastrocnemius muscle stress.
The ETHOS was originally designed to improve the ergonomics of the laparoscopic pelvic procedures effectively, by positioning the surgeon in the center of the patient's body. More specifically, the surgeon rides over the patient's head avoiding the uncomfortable torero position during the whole procedure. As a result, a common line connects the surgeon to the working field and the monitor, which remains between the legs of the patient. Two adjustable armrests and footrests can create an optimal sitting ergonomic position, reducing the harmful effects of laparoscopy and, in that way, simplifying the procedure. Its clinical feasibility was initially proved, by Kim et al., in a limited number of laparoscopic pelvic urological procedures. 9 Rassweiler et al. 10 using also the ETHOS prototype extended its clinical evaluation by comparing 53 consecutive ETHOS-assisted laparoscopic radical prostatectomies with 53 robotically assisted radical prostatectomies and 53 conventional laparoscopic radical prostatectomies, in a matched-paired analysis, according to different ergonomic parameters. The questionnaires proved the superiority of robotic pelvic surgery. Nevertheless, ergonomics as well as operating times were significantly improved by using the ETHOS chair in comparison with conventional laparoscopy. Moreover, the ETHOS chair was additionally used in 36 partial nephrectomies, 22 pyeloplasties, and a variety of difficult or, even, extremely difficult procedures, like ureteral reimplantations, sacrocolpopexies, and postchemotherapy retroperitoneal lymph node dissections, demonstrating improved ergonomic outcomes.
In the current experimental study, the ETHOS second-generation device was tested for the first time. Its differences with the prototype include more comfortable supports, more adjustment options, as well as a remote control system. The complaints of the trainees were significantly reduced after ETHOS-assisted motorized laparoscopy, when it was compared with conventional laparoscopy (standing laterally to the patient: torero position). The lack of a control group during the real operations could be a potential limitation. Furthermore, the cost cannot be easily assessed, as the platform is currently not commercially available on the market. However, purchase and maintenance costs have to be clearly less compared with the surgical robot.
Unfortunately, suturing during a laparoscopic radical prostatectomy can only be accomplished in a standing inconvenient torero position. We have mimicked this position, during suturing and while performing a bladder to urethra anastomosis, on a pig bladder specimen model. There was no significant difference between standing behind the pelvitrainer and sitting on ETHOS in anastomosis time periods. The difference became significant by comparing the sitting on ETHOS with the torero position, which was mimicking the clinical scenario (p<0.001). Maintaining an ergonomic position, by working on the chair, might facilitate the anastomosis procedure during laparoscopic surgeries.
Conclusion
Ergonomics in laparoscopy may be significantly improved by the new operating platform (ETHOS), which supports the sitting position of the surgeon with armrests and integrated foot pedals. Thus, ETHOS can improve urethrovesical anastomosis times and quality in a clinical setting. Furthermore, if accompanied by improved optic systems and ergonomic-designed instrumentation, it can potentially play an important role in an ergonomic laparoscopic setting, demonstrating outcomes that may approximate those of robotic surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.