
Abstract
Ureteral stent placement may be needed in patients undergoing robot-assisted radical prostatectomy (RARP) in cases of a large median lobe or previous transurethral surgery to prevent damage to the ureteral orifices. Unpredictable anatomic variants or technical difficulties in bladder neck section may necessitate intraoperative stent placement. We describe our original, simple, and feasible transurethral stent placement technique during RARP, which could be a valid option to preoperative technique.
Introduction
B
The placement of ureteral stents may be needed before surgery in high risk patients or during RARP because of unpredictable anatomic variant, difficult neck sections, or even standard sections performed by surgeons during the learning curve. Authors have reported different techniques for intraoperative ureteral stent placement without robot undocking. Katz and associates 6 published a safe technique in two patients by using an angiocatheter that was passed through the abdominal wall via a suprapubic incision. El Douaihy and colleagues 7 reported their strategy in 30 patients, in which the guidewire and stent were passed into the lumen of the suction trocar.
We describe our original technique of intraoperative stent placement by the transurethral approach. A video demonstrating this technique is available online at
Technique
Accurate observation of the bladder-prostate junction is mandatory to sharply identify the incision line. After dissecting the anterior surface of the prostate, the lateral bladder walls are pressed just cranially to the prostate junction, and the urethral catheter is tractioned caudally to assess the borders of the prostate and/or the anatomy of a median lobe. After anterior bladder neck section, the orifices are identified before performing the incision of the posterior neck and without the routine use of diuretics or indigo carmine because of the optical magnification (Fig. 1).

Identification of ureteral orifices.
After posterior incision, if a median lobe is present, we perform a wide excision of the trigone; occasionally, we put a traction stitch when a very large adenoma is found to perform an easier and more precise posterior bladder neck incision. 8 Subsequent steps are the standard ones for RARP.
If needed, we perform a bladder neck reconstruction, which is computed by a longitudinal or transverse technique depending on both size and shape of the incision.
Technical steps of transurethral stent placement
1. Before the anastomosis is performed or, more frequently, after the posterior plane has been reconstructed, a guidewire is introduced into the lumen of the Foley urethral catheter by the assistant.
2. The guidewire is grasped into the Foley catheter tip hole by robotic arms (Fig. 2) and is easily passed through the ureteral orifice and then into the ureter (Fig. 3).
3. The assistant removes the Foley catheter and introduces, over the guidewire, the double-pigtail stent, which is grasped by robotic forceps and then passed in a retrograde fashion (Fig. 4).
4. After the stent has been placed, the guidewire is removed, and the same procedure is then repeated on contralateral side.
5. Postoperatively, the correct stent position is checked by abdominal radiography. The stents are removed in an outpatient setting, which is scheduled 1 to 2 weeks after RARP, according to the level of the task involved in performing the technique.
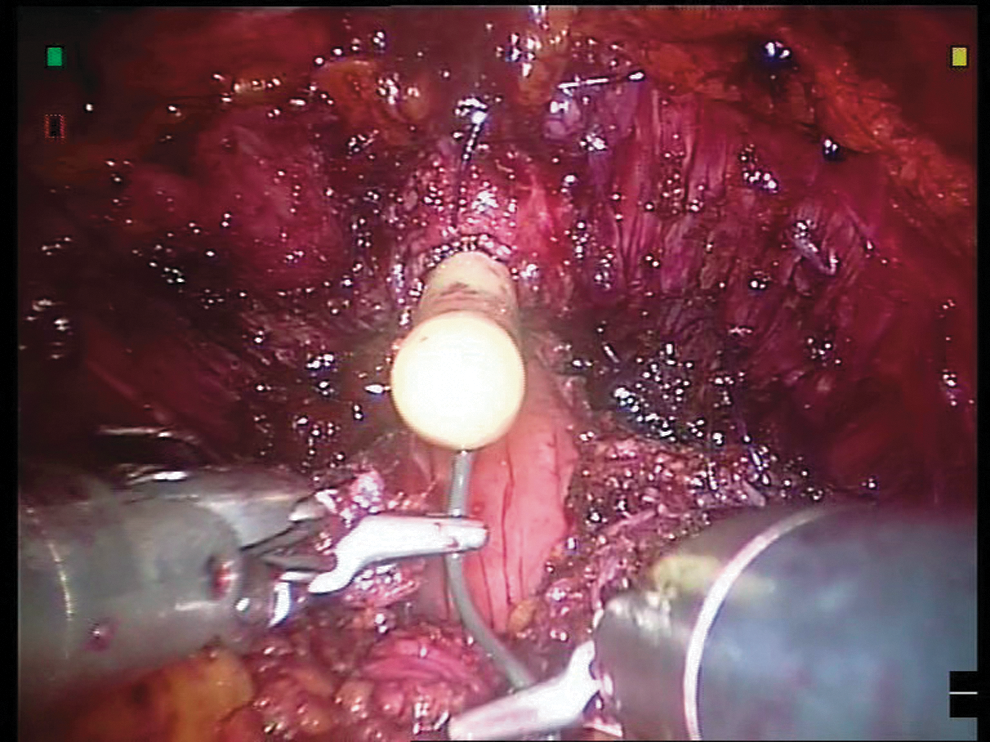
The guidewire introduced in the urethral catheter is grasped into the Foley catheter tip hole.
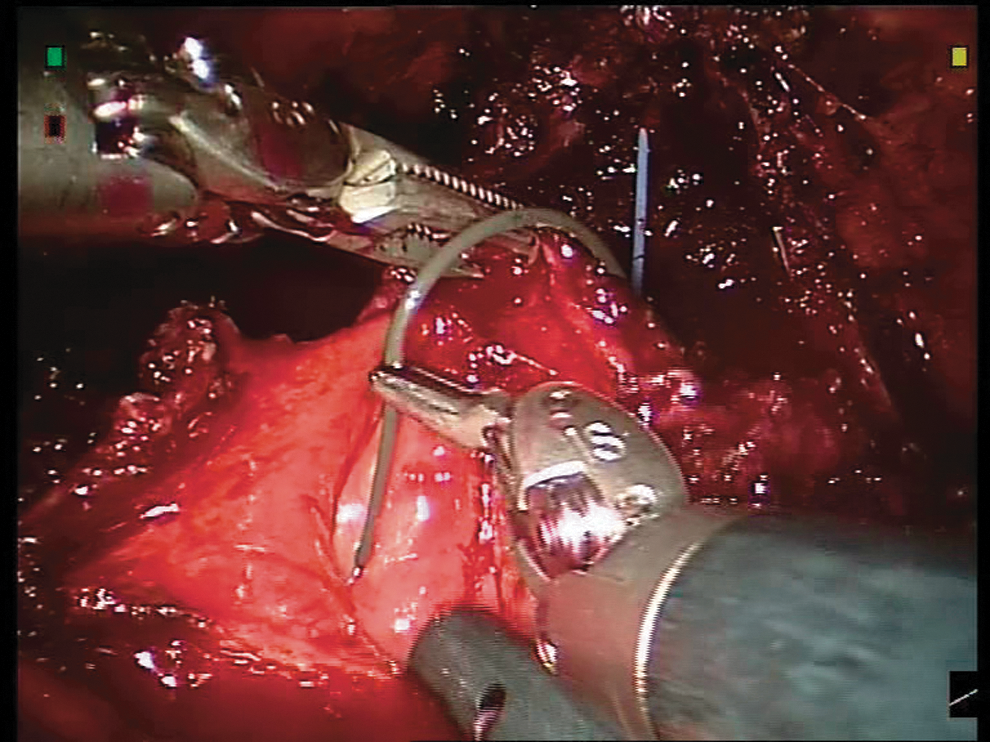
The guidewire is passed through the left ureteral orifice.

The double pigtail stent is passed over the guidewire.
Equipment
• Nitinol guidewire with hydrophilic straight tip (0.035 in×150 cm)
• Double Loop 6F ureteral stents (height-adjusted)
Role in Urologic Practice
This original technique reproduces the endoscopic stent placement procedure. The advantage of “natural” anatomic axis between the urethra and ureteral orifices and the robot Endowrist® extreme ease of movement make this step simple, feasible, and not at all time consuming (5–7 minutes on average for the bilateral procedure). Our technique, when compared with other reported procedures, 6,7 has been shown to be easier to perform and less invasive because it avoids further abdominal incision.
In our institution, since 2007, the reported technique has been used in 2% of cases (15 of 700 RARP). Before developing the technique, we did not have any complications related to the anastomosis; however, when bladder neck dissection is close to the orifices, the reported technique prevents the potential complications related to obstruction of the ureters. As a result, the surgeon feels more confident with stent placement in the upper urinary tract.
In our opinion, when the technique is indicated, bilateral stent placement is the gold standard because edema after anastomosis may involve both orifices. Going into technical details, we stress that it is not necessary to move the stents back and forth after performing the posterior portion of the anastomosis because, in our hands, the technique has been simple and effective. Moreover, the stents do not get in the way of the anastomosis.
As a theory, more bladder instability incontinence related to stent placement could be expected; however, we did not investigate this point because of its not being the main aim of the study.
One month after stent removal, according to our protocol, patients were followed by ultrasound investigation of the upper urinary tract. As a result, patients did not have any complication including upper urinary tract obstruction, bladder neck stricture, or anastomotic leakage.
El Douaihy and coworkers 7 reported some concerns about preoperative placements of stents by cystoscopy because large median lobes may not allow the identification of ureteral orifices. In our opinion, the reported technique could be a valid option to preoperative stent placement, which, however, may become a very difficult task when a large median lobe of the prostate is present. Moreover, our technique may avoid unnecessary preoperative placement of stents, which may be a time consuming procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviation Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.