
Abstract
Objective:
To describe the management of the distal ureter during radical nephroureterectomy with the transvesical laparoendoscopic single-site surgery (T-LESS) approach.
Methods:
Between January 2010 and October 2013, five patients underwent laparoscopic radical nephroureterectomy for upper urinary tract carcinoma (UTUC) with the T-LESS approach. Patients were placed in the supine position. A 2.5-cm skin incision was made in the line between the pubis and the umbilicus. The bladder was identified and a multiport was inserted into the bladder. The patients were repositioned to a lateral decubitus position; pneumovesicum was established and the ureteral openings were identified. We marked the bladder cuff with electrocautery all the way through to the extravesical fat. The bladder defect was sealed with sutures. After checking for any leak or bleeding, the multiport was removed and the bladder was closed. At this point, we continued with nephrectomy by standard laparoscopy or LESS. A 18F Foley catheter was placed into the bladder.
Results:
The mean age was 70 years (range 58–81 years), the mean operative time was 198 minutes (range 115–390 minutes), the mean time for the management of the distal ureter was 35 minutes (range 27–45 minutes), the mean estimated blood loss was 234 mL (range 60–850 mL), and the mean hospital stay was 3.8 days (range 2–8 days). In all patients the bladder cuff was free of disease.
Conclusion:
The transvesical laparoendoscopic single-site approach to the distal ureter for UTUC appears safe and reproducible, with faster closure of the bladder defect and improved cosmesis.
Introduction
Upper urinary tract carcinoma (UTUC) accounts for 5% to 10% of urothelial carcinomas, 1,2 with concurrent bladder cancer in about 17% of cases. 1 Radical nephroureterectomy (RNU) with excision of the bladder cuff is the gold standard treatment for UTUC, regardless of the location of the tumor in the upper urinary tract. 1 –7 RNU was traditionally performed on the open approach, until 1991, when Clayman first described the technique of laparoscopic radical nephroureterectomy (LRNU), which was soon replicated by various authors worldwide. 3 The outcomes of different bladder cuff management approaches remained poorly investigated. In 2004, Steinberg and Matin 4 described at least five different techniques of distal ureterectomy during LRNU, which often combined endoscopic, laparoscopic, and open features. They differed not only in technical aspects but also in oncological outcomes as well. Li and colleagues 5 reported no difference in oncologic outcomes among three different approaches to the distal ureter (transvesical, extravesical, and endoscopic) in a retrospective single center. Recently, Xylinas and colleagues reported that the endoscopic approach was associated with higher rates of intravesical bladder cancer recurrence. 6 Cheng and colleagues 7 and, more recently, Zou and colleagues 8 described a method for managing the distal ureter during LRNU using pneumovesicum.
We initially reported our novel technique of a totally endoscopic approach for block dissection of the distal ureter and bladder cuff during LRNU, using a transvesical single-port (T-LEES) device in a patient with UTUC. 9
Herein, we report our experience with transvesical laparoendoscopic single-site surgery (T-LESS) in five consecutive patients with UTUC, with particular emphasis on technical developments, functional, and oncological outcomes.
Patients and Methods
Between January 2010 and October 2013, five patients underwent LRNU for UTUC by one surgeon (Rene J. Sotelo). In the initial four cases, we did the technique that we described in 2011, 9 and in the last case we did some modifications, including the use of a running barbed suture to closure the bladder defect, and changes in the sequence of the surgery. All patients were evaluated peroperatively and no concomitant bladder tumors were found. We will focus on describing the last technique, which we believe is more efficient.
Surgical technique
The patients were placed in the supine position and a flexible cystoscopy is performed to evaluate the urethra and bladder. After that, we filled the bladder with 350 to 500 mL of physiologic saline, enough to mobilize the bladder dome into the space of Retzius. A 2.5 cm skin incision is made in the line between the pubis and the umbilical scar down the rectus fascia muscle, which is opened. The bladder is identified and cleared of perivesical fat. Two stitches of 2-0 Vicryl are put in the bladder to assist with the introduction of the multiport. The bladder is then incised between these two stitches. A preloaded inner ring of the multiport is inserted into the bladder with an introducer and the excess saline is suctioned. Both inner and outer rings are then approximated, thus creating an airtight access into the bladder lumen. Next, the patient is repositioned to a lateral decubitus position, pneumovesicum is established, and a 5-mm deflectable EndoEye (Olympus Medical System Corp.) is introduced into the bladder through the multiport. After the ureteral openings are identified, we mark the bladder cuff with electrocautery all the way through its thickness, until identification of the extravesical fat (Fig. 1). The distal ureter is pulled into the bladder with a grasper (Fig. 2), a 5 mm Hem-o-Loc® is used to close it, and then the distal ureter is pushed out. The bladder defect is sealed with a V-loc™ closure suture; with the first stitch, the needle is exteriorized and passed through the distal loop of the suture, which was used as an anchor in the bladder. We then continue the suture in a running manner until the defect is sealed. The suture is then cut and locked without any knots. We use an extracorporeal suture segment to maintain traction and help with the intracorporeal suturing (Fig. 3). After checking for any leak or bleeding, the multiport is removed and the bladder is closed. At this point, we continue with the nephrectomy by standard laparoscopy 10 or laparoendoscopic single-site surgery (LESS) 9 as a second stage. The ureter is dissected caudally into the pelvis until identification of the distal segment with the Hem-o-Loc. It is possible to use the tract left by the multiport as a place to insert the trocar for the LRNU, as we did in the first case. An 18F Foley catheter is placed into the bladder for continuous drainage and it is removed 10 days later.
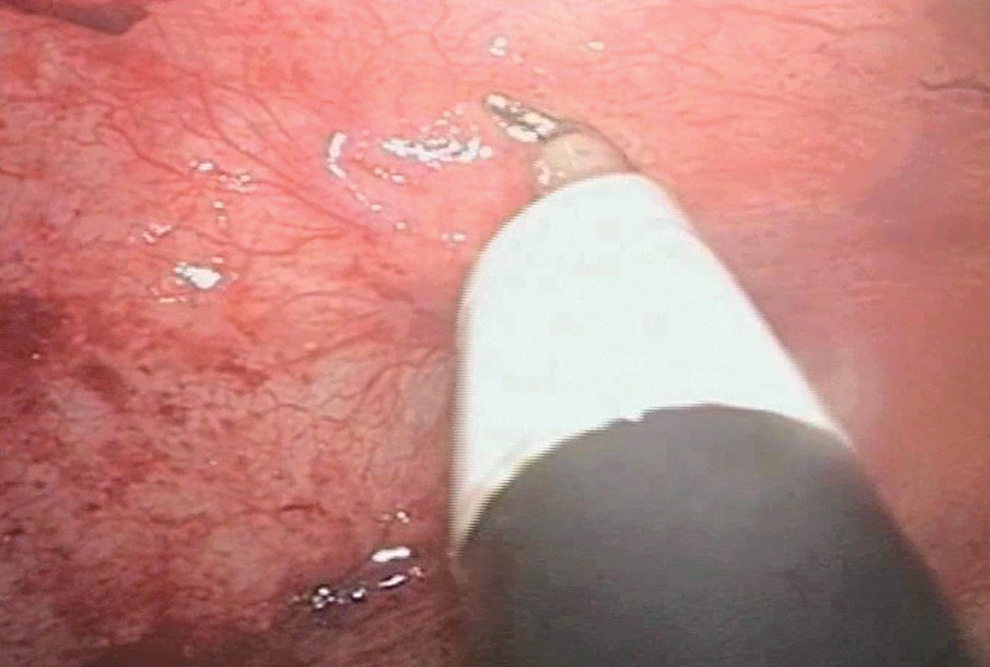
Ureteral opening is identified and marked with electrocautery.

Distal ureter pulled into the bladder.

Trick to close the bladder defect with the help of an extracorporeal suture segment.
On the first four patients, the sequence of the technique was different in three stages; the trocars were placed in the supine position and the patient was repositioned to the lateral position. First, a transabdominal three port or one multiport approach was used with early ligation of the ureter using a Hem-o-Loc clip. Second, we worked into the bladder, similar to the technique described previously, and then performed the nephrectomy. 9,10 In both cases, the specimen (kidney, ureter, and bladder cuff) was retrieved with an EndoCatch™ bag and removed through a Pfannenstiel incision. We left a suction drain in the perinephric and distal ureteral space, which was removed 2 days later. The port incisions were then closed. Patients were followed up every 3 months the first year and every 6 months thereafter, to check for tumor recurrence.
Results
Of the five patients, the mean age was 70 years (range 58–81 years) and most of them (80%) were male. While all patients had left-sided tumors in the pelvis, 2 (40%) also had a concomitant tumor in the proximal ureter. The mean operative time was 198 minutes (range 115–390 minutes) and the mean time for the management of the distal ureter was 35 minutes (range 27–45 minutes). The mean estimated blood loss was 234 mL (range 60–850 mL) and the mean hospital stay was 3.8 days (range 2–8 days). In all patients, the bladder cuff was free of disease and the final pathology was urothelial carcinoma. Two patients (40%) were grade 3 and one patient had positive lymph nodes at final pathology. Two patients had Clavien grade II complications 11 : one had prolonged ileus that resolved with conservative management and one had significant intraoperative bleeding requiring blood transfusion. With a mean follow-up time of 16.2 months (range 1–38 months), one patient developed spinal cord metastasis.
Discussion
The treatment of UTUC has undergone significant changes over time. Open RNU was the gold standard for UTUC, until the appearance of the LRNU technique in the early 1990s. LRNU has emerged as a feasible minimal invasive approach to the procedure. Compared with the open approach, it has shown similar results along with better recovery, including decreased blood loss, shorter hospitalization, and faster return to normal activity. 1 –4
Despite wide acceptance of LRNU, there is still a controversy regarding the optimal management of the distal ureter and bladder cuff. Several different techniques have been described for its management, and minimally invasive surgeons combine the LNRU with open, endoscopic, extravesical, or transvesical approaches. 10,11 –18 Recently, Xylinas and colleagues 6 reviewed the data from 24 centers, including 2681 patients who underwent RNU with three different approaches for the distal ureter. Overall, they did not find differences in nonbladder recurrence or survival between the transvesical, extravesical, and endoscopic approaches to the bladder cuff; however, the endoscopic approach had a higher rate of intravesical bladder cancer recurrence. For this reason, we adopted the transvesical approach.
Gill and colleagues 19 were the first to report a transvesical approach, which in fact was a combination of transvesical and endoscopic management of the distal ureter. The bladder was filled with saline to create a working space for a resectoscope and needlescopic ports. However, problems with this technique include the difficult learning curve as well as the potential for tumor seeding with fluid extravasation through the bladder defect and transvesical ports.
Zou and colleagues 8 described a technique similar to Gill's technique, except that they used pneumovesicum instead of saline to create a working space, one 10-mm trocar replaced the two needlescopes, a Hem-o-loc clip was used to close the ureteral orifice, and a retroperitoneal nephrectomy was performed. The drawback to this technique was that the bladder defect was left open with the potential risk of tumor seeding and it required that the patient be repositioned. This article was not the first to use pneumovesicum. Cheng and colleagues 7 used three 5-mm PediPorts™ (Tyco) with a transvesical approach. A stitch was placed to close the ureteral orifice and to use as a retractor during mobilization of the intramural portion. Again the defects made by ports were left open.
LRNU has also been described using the Da Vinci System. Recently, Lee and colleagues 20 reported on robotic nephroureterectomy without patient positioning or redocking of robotic arms with excellent results. Nevertheless, in settings where the robot is not available, our technique offers an alternative with adequate management of the distal ureter under direct vision and total sealing of the bladder.
As described previously, we used a laparoendoscopic single-port transvesical approach with pneumovesicum to create a working space to manage the distal ureter. During the initial cases, after placing the trocars, we began with early control of the ureter and caudal dissection, continued with the bladder cuff by T-LESS, and finally performed the nephrectomy in a three-stage manner. Our technique has evolved from a three- to a two-stage surgery, with the management of the distal ureter as a first stage, followed by the nephrectomy and caudal dissection of the ureter as a second stage. In all cases, we placed the Triport in the supine position, after which the patients were repositioned to the lateral position. This is important to keep bleeding, irrigation, and urine at the opposite side of the field, without visual obstruction of the ureter being worked on. In addition, we closed the defect left after mobilization of the ureter; the operative time of the distal ureter in the last patient was faster using the V-loc suture, which facilitated closure of the bladder defect. This technique provides good control of the distal ureter, minimizes the potential for tumor seeding, and provides a minimally invasive alternative that resembles the traditional open approach.
The present study has some limitations, including the small number of patients and the short duration of the follow-up. In addition, this technique requires an experienced surgeon in LESS.
Conclusion
The transvesical laparoendoscopic single-site approach of the distal ureter and bladder cuff for UTUC seems to be safe and reproducible. It provides a minimally invasive technique with early control of the distal ureter under direct vision, faster closure of the bladder defect, and improved cosmesis. Further study is needed with more patients and a longer follow-up to confirm the advantages of this method.
Footnotes
Disclosure Statement
No competing financial interests exist.