
Abstract
Purpose:
To evaluate intermediate-term oncologic outcomes in a large series of patients who were treated with robot-assisted radical cystectomy (RARC) for urothelial carcinoma of the bladder (UCB).
Patients and Methods:
Between 2004 and 2010, 162 patients underwent RARC at City of Hope Cancer Center for UCB and were analyzed with respect to overall (OS), disease-specific (DSS), and disease-free survival (DFS). Descriptive statistics were used to summarize demographics and perioperative variables. The Kaplan-Meier method was used to estimate survival and recurrence. Univariable and multivariable Cox proportional hazards regression models were used to determine predictors of survival.
Results:
Median follow-up was 52 months. Thirty-eight (23.4%) patients received neoadjuvant chemotherapy before RARC; 28% of patients were pT2 and 33% had final pathology status of pT3 or pT4. Median lymph node count was 28, and positive surgical margin rate was 4.3%. Local recurrence occurred in 11 (6.8%) patients. OS, DFS, and DSS at 3 years were 61%, 76%, and 83%, respectively. OS, DFS, and DSS at 5 years were 54%, 74%, and 80%, respectively. Predictors of OS and DFS on multivariable analysis were lymph node density, pathologic stage, and age-adjusted Charlson Comorbidity Index, while receipt of transfusion was also a negative predictor of OS.
Conclusions:
RARC provides an effective means of treatment of UCB in a minimally invasive fashion with comparable oncologic outcomes to that reported in the literature of open procedures.
Introduction
M
Efforts to reduce convalescence and complications and improve quality of life are continuing goals of minimally invasive RARC. Technical modifications aside, the oncologic efficacy of RARC is of primary importance. ORC remains the surgical standard, and early randomized controlled trials comparing ORC and RARC are ongoing. 5 In a series of 1054 patients with ORC, Stein and associates 6 reported recurrence-free survival of 68% at 5-year follow-up and local recurrence rates of 7%. Early RARC series have used positive margins and lymph node yields as surrogates for oncologic outcomes, 7,8
Recent reports on survival outcomes in laparoscopic radical cystectomy have shown similar results to those of ORC. 9,10 Recent longer-term data on RARC are becoming available in small series. 11 We evaluated the oncologic benefits of RARC in a large consecutive series of patients who were treated for urothelial carcinoma of the bladder (UCB) with respect to pathologic, recurrence, and survival outcomes.
Patients and Methods
Figure 1 demonstrates our patient selection process. Between 2004 and 2012, 254 RARCs were performed at City of Hope Cancer Center. Of these, 204 patients consented to an Institutional Review Board approved protocol for prospective data collection. We limited our intermediate-term survival analysis to 162 consecutive patients with confirmed pathologic evidence of UCB who underwent RARC before 2010.

Flowchart of patient selection.
Our institutional practice is to perform RARC rather than ORC regardless of clinical stage. Thus, no patient is excluded from RARC unless they are undergoing open surgery for another indication. Candidates for RARC had cT2 or greater disease, bacillus Calmette-Guérin–refractory disease, high-risk ≤cT1 disease, or disease that was uncontrollable by endoscopic management. Patients with RARC converted to an open procedure (n=2) were excluded from the analysis. For these two patients, conversions were performed for difficult dissections in pT3/pT4 disease. Furthermore, patients with squamous cell carcinoma, adenocarcinoma, and sarcomatoid histologies were excluded (n=14).
Postoperatively, patients were followed according to National Comprehensive Cancer Network guidelines (urine cytology, creatinine level, liver function tests, and electrolytes values every 3–6 months for 2 years then as clinically indicated; imaging of the chest, abdomen, and pelvis every 3–12 months for 2 years and then as clinically indicated; urethral wash cytology every 6–12 months; and monitoring of the vitamin B12 levels yearly). Local recurrence was defined as clinical or radiographic evidence of disease in the pelvis or lymph node basins after RARC. Recurrence of disease outside these areas (including upper tract) was deemed distant recurrence. Persistent disease was defined as a lack of disease-free status at any point after a surgical procedure and included patients who underwent RARC for palliative intent.
Patient demographic, clinical, surgical, and pathologic data were retrospectively reviewed and summarized using descriptive statistics. The Kaplan-Meier method was used to compute estimates for overall (OS), disease-free (DFS), and disease-specific survival (DSS). Univariable and multivariable Cox proportional hazards regression models were used to identify predictors for OS and DFS. Clinical variables such as age, sex, body mass index, American Society of Anesthesiologists (ASA) score, age-adjusted Charlson Comorbidity Index (CCI) score, receipt of neoadjuvant chemotherapy, smoking status, and previous abdominal surgery were examined alongside pathologic indicators such as number of nodes sampled (>15 vs ≤14), positive surgical margins, pathologic stage (pT3/T4 vs<pT3), and lymph node density (number of positive nodes/total nodes sampled, 1–10%, >10% vs node-negative). We also considered as predictors whether patients needed a blood transfusion or experienced Clavien grade III and above complications within 90 days after the surgical procedure. SAS® v9.3 software was used for all statistical analyses and computations.
Operative technique
RARC was performed with the daVinci® Surgical System (Intuitive Surgical, Sunnyvale, CA) using a six-port transperitoneal approach described previously. 11 Bilateral ureters were freed down to the base of the bladder and then clipped to prevent urine contamination before division. A frozen section from the distal end of each ureter was sent for examination. An extended pelvic lymphadenectomy was performed typically with the limits of dissection as the crossing of the circumflex iliac vein over the external iliac artery (distal), the genitofemoral nerve (lateral), the bladder (medial), the obturator fossa (posterior), and up to the level of the inferior mesenteric artery (superior). Lymph node packets were sent for pathologic evaluation as regional, separate specimens.
Posterior and lateral pedicles were divided using a laparoscopic articulating stapler. The dorsal venous complex was controlled using a laparoscopic stapling device or suture ligation. In men, after prostatic apical dissection, the urethra was divided and a frozen section from the urethra was sent for examination. In men, if an orthotopic urinary diversion was not planned, the urethra was clipped distally before transection and the specimen side oversewn to prevent urine spillage during division. In women, the posterior vaginal vault was opened and the lateral vaginal wall was divided using thermal energy, thus leaving a portion of the anterior vaginal wall associated with the surgical specimen. The remaining vaginal tissue was reapproximated in a clamshell fashion. Furthermore, if a woman had not had a hysterectomy, anterior exenteration was performed.
All specimens were placed in impermeable bags once free and before removal from the body. Urinary reconstructions were performed in an open, extracorporeal fashion using a Studer pouch, Indiana pouch, or ileal conduit, depending on patient characteristics and preference after thorough discussion between the physician and patient.
Results
Demographics for the 162 patients with UCB are shown in Table 1; 136 (84%) patients were men and the median age at surgery was 70 years. Median age-adjusted CCI score was 8 (interquartile range [IQR]: 5–11) and 126 (77.8%) patients had an ASA score ≥3. Clinical stage was T2 or higher in 105 (65%) patients, and median follow-up was 52 months. Neoadjuvant chemotherapy was administered to 38 (23.4%) patients, with 84% completing at least three cycles. Twenty-eight (74%) of these patients received combination gemcitabine and cisplatin (n=13) or methotrexate, vinblastine, doxorubicin, and cisplatin (n=15) with the others receiving alternative regimens (ie., carboplatin and gemcitabine). Continent diversions were performed in 70.4% of cases. A complication of any Clavien grade (i.e., grade I–V) occurred in 133 (82.1%) patients with a major complication rate (i.e., grade III–V) of 37% (n=60).
IQR=interquartile range; BMI=body mass index; ASA=American Society of Anesthesiologists; EBL=estimated blood loss.
Pathologic examination after RARC showed 108 (66.7%) patients to have organ-confined disease (or pT0) while 54 (33.3%) had ≥pT3 disease (Table 2). The median lymph node yield was 28 (IQR: 19–38) with positive nodes in 21.6% (n=35). Of those with positive lymph nodes, 15 (42.9%) patients received adjuvant chemotherapy. The rate of positive margins was 4.3%. Chronologic breakdown of the study population into two 81 patient groupings showed no difference in positive margin rates; however, lymph node yield did increase successively.
IQR=interquartile range.
A recurrence developed in 39 (24.1%) patients over the follow-up period. Eleven (6.8%) patients experienced local recurrence at a median 8 months after RARC. Metastatic disease developed in an additional 28 (17%) patients during the follow-up period. Nine (5.6%) patients had persistent disease. With regard to mortality, 58 (35.8%) patients died during follow-up. Twenty-six (44.8%) patients died of other causes with no evidence of disease at time of death, 7 patients (12.1%) had recurrence of bladder cancer but died of other causes, and, lastly, 25 (43.1%) patients died from bladder cancer.
Three-year OS estimate after RARC was 61%, DFS was 76%, and DSS was 83%. Five-year OS estimate was 54%, DFS was 74%, and DSS was 80% (Fig. 2). Patients with organ-confined disease (≤pT2) had improved survival compared with those with nonorgan-confined disease (pT3–4) with respect to OS, DFS, and DSS (Fig. 3).

Overall (OS), disease-free (DFS), and disease-specific (DSS) survival for patients undergoing robot-assisted radical cystectomy for urothelial carcinoma of the bladder.
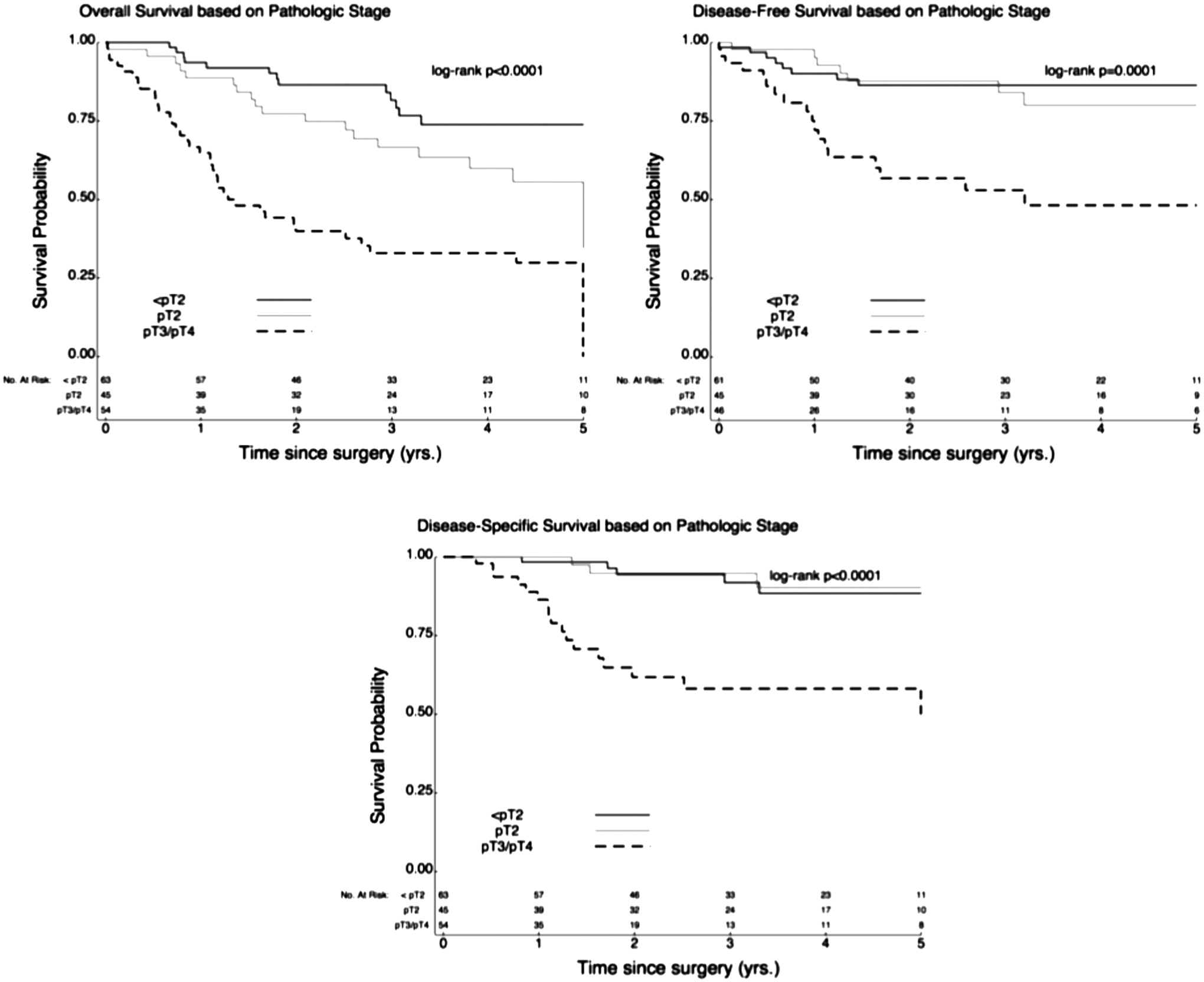
Overall, disease-free, and disease-specific survival for patients undergoing robot-assisted radical cystectomy stratified by pathologic stage.
Patients with no evidence of lymph node invasion had improved survival compared with patients with lymph node positive disease (P<0.0001, Fig. 4). Patients with node negative disease had 3-year OS, DFS, and DSS of 70.9%, 83.1%, and 92.1%, respectively. In contrast, patients with node density of 1% to 10% had 3-year OS, DFS, and DSS of 30.7%, 34.3%, and 49%, respectively. Finally, patients with node density of >10% had even worse outcome with 3-year OS, DFS, and DSS of 20.0%, 29.6%, and 37.9%, respectively.

Overall survival for patients undergoing robot-assisted radical cystectomy stratified by lymph node involvement and density.
Univariable analysis of OS showed that age, CCI, positive surgical margins, higher pathologic stage, receipt of blood transfusion, and lymph node positivity negatively predicted survival. With multivariable analysis, CCI (P<0.01), pathologic stage (P=0.01), receipt of blood transfusion (P=0.05), lymph node density 1% to 10% (P=0.05), and lymph node density >10% (P=0.03) were the only independent predictors of overall survival (Table 3).
Body mass index, sex, smoking status, neoadjuvant chemotherapy and radiation, number of nodes sampled, and 90–day incidence of major adverse events were assessed in the model and found not to be significant predictors of overall survival.
CI=confidence interval; CCI=Charlson Comorbidity Index.
Analysis of DFS yielded similar but slightly different results. Under univariable analysis CCI, pathologic stage, and lymph node positivity were predictive of DFS. Multivariable analysis confirmed these variables as being independent predictors (Table 4).
Body mass index, sex, smoking status, neoadjuvant chemotherapy and radiation, positive bladder margin(s), number of nodes sampled, and 90–day incidence of major adverse events were assessed in the model and found not to be significant predictors of disease-free survival.
CI=confidence interval; CCI=Charlson Comorbidity Index.
Discussion
With emerging surgical techniques, continued assessment and reevaluation are necessary to ensure optimization of outcomes. Maturing data from robotic cystectomy series are presently addressing the cancer control characteristics of this procedure. Our experience at a high-volume RARC center demonstrates low positive margins (4%), adequate lymph node yields (28), and a low rate of local recurrence (7%). The 3- and 5-year survival outcomes are similar to those of contemporary ORC series. Lymph node positivity, higher pathologic stage, and baseline comorbidity are important prognostic factors with regard to survival. Receipt of perioperative blood transfusion was also negatively associated with overall survival. In a similar manner, Linder and coworkers 12 also found perioperative blood transfusion to be associated with cancer recurrence and mortality.
ORC represents the gold standard surgical approach to locally advanced bladder cancer, with large series reporting long-term survival benefits. Stein and associates 6 previously reviewed 1054 patients who had undergone ORC with OS of 60% at 5 years and 43% at 10 years. The DFS was 68% and 66% at 5 and 10 years, respectively. In another analysis, Hautmann and colleagues 13 reviewed 1100 chemotherapy naïve patients and showed similar results at 10 years with OS of 44%, DSS of 67%, and DFS of 66%.
The role of minimally invasive radical cystectomy is still evolving. Some studies have shown RARC to compare favorably with the open technique with respect to reduced blood loss, pain, time to bowel recovery, and complications. 1 –3 Because of the limited time in which robotic cystectomies have occurred, most studies have been restricted to 1-, 2-, or 3-year oncologic outcome data. 7,8,14 –16 In a study by Nepple and coworkers, 14 36 patients who had undergone RARC were directly compared to 29 patients who had undergone ORC. Estimated 2-year DFS (67% vs 58%), DSS (75% vs 63%), and OS (68% vs 63%) after RARC and ORC were similar between the two techniques, respectively. In addition, Martin and colleagues 8 reported on 59 RARC patients with a median follow-up of 25 months and found 3-year OS and DSS of 69% and 72%, respectively. Khan and associates 10 described the longest follow-up after RARC in a small series (n=14) of patients with follow-up of 5 years or mortality from bladder cancer. OS, DSS, and DFS were 64%, 75%, and 50%, respectively. The findings of the present study with five-year OS (54%), DFS (74%), and DSS (80%) compare well with reports in the literature on open procedures.
Selection bias is a potential confounding factor in comparing RARC and ORC because there has been a general tendency in the literature to select healthier patients with less comorbidity and lower volume disease for the newer technology of RARC and use ORC for sicker patients with more advanced disease. 17 At our institution, nearly all patients are treated with RARC unless a minimally invasive approach is contraindicated. For our analysis, no selection of patients occurred as evidenced by the median age of 70 years, nearly 80% with ASA score ≥3, and one-third with extravesical disease at final pathologic evaluation.
Earlier RARC series adopted lymph node yield as a surrogate for oncologic efficacy. May and coworkers 18 recently indicated that patients who had removal of ≥16 lymph nodes fared better than those with <16 lymph nodes removed with a DSS of 83% vs 72% (P=0.01). Likewise, Abol-Enein and associates 19 preferentially recommended an extended lymph node dissection as a result of 5-year DFS of 66.6% for an extended dissection compared with 54.7% for a standard dissection. The robotic technique for lymphadenectomy has been shown to generate a similar lymph node yield compared with open technique. 20 In the present study, 21.6% of patients had at least one positive lymph node, similar to what is seen in the literature on the open technique and other RARC series. To elaborate on the previously described theory of lymph node density as a measure of nodal metastasis volume, we also found higher density to be associated with decreased survival. 21
Neoadjuvant chemotherapy before cystectomy compared with cystectomy alone has been shown to confer a survival advantage. Grossman and coworkers 22 showed that the median survival for patients with neoadjuvant chemotherapy before cystectomy was 77 months compared with 46 months in those who just underwent cystectomy (P=0.06). Neoadjuvant chemotherapy is still underutilized in clinical practice, although the incidence is increasing. In the same ORC series from the University of Southern California above, neoadjuvant chemotherapy was used in 5% of 1054 patients from 1971 to 1997. 6 In a more recent ORC series looking at 432 patients from 1992 to 2007, neoadjuvant chemotherapy was delivered in 13% of patients. 23 In the robotic literature, neoadjuvant chemotherapy is increasingly being used with studies showing usage rates of 5% to 20%. 8,15,16
In the current study, 23.4% of patients received neoadjuvant chemotherapy, consistent with the increasing trend to use systemic therapy along with surgery in the management of UCB. Although the majority of these patients received “standard” neoadjuvant regimens and completed at least three cycles before RARC, the lack of improvement with respect to OS or DFS suggests that the analysis was underpowered to detect a difference.
Limitations of this study include its retrospective design as well as the relatively lower number of patients reviewed. Moreover, this study was performed at a high volume RARC center, and the outcomes of this study may have limited applicability to surgeons performing a lower volume or in hospitals with a lower volume. Further study is needed to determine the oncologic effectiveness of RARC up to and beyond 10 years after treatment. Meanwhile, prospective, randomized, controlled trials comparing RARC with ORC are needed.
Conclusions
RARC is an effective method of locally controlling bladder cancer in a minimally invasive fashion with durable long-term survival and comparable outcomes to what is seen in the literature on open procedures. Continued long-term follow-up and randomized, controlled, prospective trials are necessary to fully compare RARC with open surgical techniques.
Footnotes
Disclosure Statement
No competing financial interests exist.