
Abstract
Introduction:
Local steroids have been used as an adjuvant therapy to patients undergoing internal urethrotomy (IU) in treating urethral strictures. Whether this technique is effective and safe is still controversial. The aim of this study is to determine the efficacy and safety of local steroids as applied with the IU procedure.
Methods:
A systematic review of the literature was performed by searching Medline, Embase, Cochrane Library Databases, and the Web of Science. We included only prospective randomized, controlled trials that compared the efficacy and safety between IU procedures with applied local steroids and those without.
Results:
Eight studies were found eligible for further analysis. In total, 203 patients undergoing IU were treated with steroid injection or catheter lubrication. Time to recurrence is statistically significant (mean: 10.14 and 5.07 months, P<0.00001).The number of patients with recurrent stricture formation significantly decreased at different follow-up time points (P=0.05).No statistically significant differences were found between the recurrence rates, adverse effects, and success rates of second IUs in patients with applied local steroids and those without.
Conclusion:
The use of local steroids with IU seems to prolong time to stricture recurrence but does not seem to affect the high stricture recurrence rate following IU. When local steroids are applied with complementary intention, the disease control outcomes are encouraging. Further robust comparative effectiveness studies are now required.
Introduction
U
Various techniques have been described for treatment of urethral strictures, depending on the stricture length, location, and depth of the scar. Open urethroplasty of urethral strictures has been dramatically developed worldwide and remains the gold standard for urethral reconstruction. This surgery is often carried out in high-volume, dedicated centers. Internal urethrotomy (IU), however, is still a worthwhile method for treating urethral strictures and is the first choice in many secondary centers. According to the results of a nationwide survey, IU is used for most urethral strictures in the United States. 2 However, high recurrence rates have been reported with this technique and its effectiveness is being questioned by many urologists. 3 These low success rates suggest the need for the development of additional new techniques and complementary strategies to prevent wound contraction and recurrent stricture formation. The purpose of the present meta-analysis is to identify and summarize the evidence of the efficacy and safety of local steroids applied to patients with urethra stricture while undergoing IU.
Materials and Methods
Eligibility criteria
The following eligibility criteria were used to identify relevant studies: (1) The target population was male individuals with urethra strictures undergoing IU with a cold knife or laser. (2) The intervention involved local steroid application, either through injection or lubricated catheter, to the fibrotic tissue of the stricture site (versus no steroid application). (3) The trial was a case-control study.
Information sources and selection of studies
We conducted our search in four databases: Pubmed (1950–February 2014), Embase (1974–February 2014), Web of Science (1985–February 2014), and the Cochrane Library (including the Cochrane Central Register of Controlled Trials, 1800–February 2014). Our searches used the terms “urethrotomy AND steroid,” “urethra AND steroid” and the mesh words “steroids” AND “urethral Stricture/therapy.” No language restrictions were applied in the search strategy.
Two reviewers (K.L. Zhang and E. Qi) independently searched the four databases. The search strategy found titles and abstracts. Irrelevant and repeated titles and abstracts were excluded. A consensus was obtained through discussion to solve disagreements between the two reviewers.
Methodological quality assessment
Methodological quality was assessed by following the guidelines of the Jadad criteria (maximum score 5). 4 The evaluation of the study's quality was done independently by two reviewers (K.L. Zhang and Y.M. Zhang). Randomization, double-blind design, and description of dropouts of each trial were assessed by the criteria. A trial with a score of 3 or more is regarded as high quality. Each trial was given an overall quality score, which was then used to rank the trials.
Data abstraction
All relevant data regarding patients' interventions, characteristics, and outcomes were extracted by using a standardized extraction form previously used by two reviewers (K.L. Zhang and E. Qi). The outcomes of steroid use with IU for urethra stricture contained the recurrence rate, the time to recurrence, the adverse effects, and maximum flow rate (Qmax) at each follow-up. Disagreement between the reviewers was resolved by discussion with senior investigators (Q. Fu, and Y.L. Sa).
Quantitative data synthesis
Meta-analysis was done using Review Manager 5.2 software (The Cochrane Collaboration, Oxford, UK). The weighted mean differences (WMD) and odds ratio (OR) were used for the analysis of continuous and dichotomous variables, respectively. The confidence interval (CI) was established at 95%. P values less than 0.05 were considered an indication of statistical significance. The Cochran Q test was used to assess the statistical heterogeneity among studies. Statistical heterogeneity was assessed using I2 statistics: If the I2 value was less than 50%, the fixed effects of meta-analysis were applied; if the I2 value was 50% or more, the random effects of meta-analysis were used. The overall effects were tested by z test. Sensitivity analysis was used to find out the statistical heterogeneity.
Results
Literature search and trial flow
We identified 1012 potentially relevant studies from the databases and obtained 49 full texts based on the title and abstract reviews (Fig. 1.). During subsequent reviews of the full texts, 10 studies were excluded for “laser versus cold knife,” 8 studies were excluded due to “dilation versus IU,” 9 studies were excluded for contents about “IU and catheter without steroid,” 3 studies were excluded because of supplementation of other medications. Eleven remaining studies were excluded for not being controlled trials. Finally, 8 studies were included for quantitative synthesis and meta-analysis. 5 –9
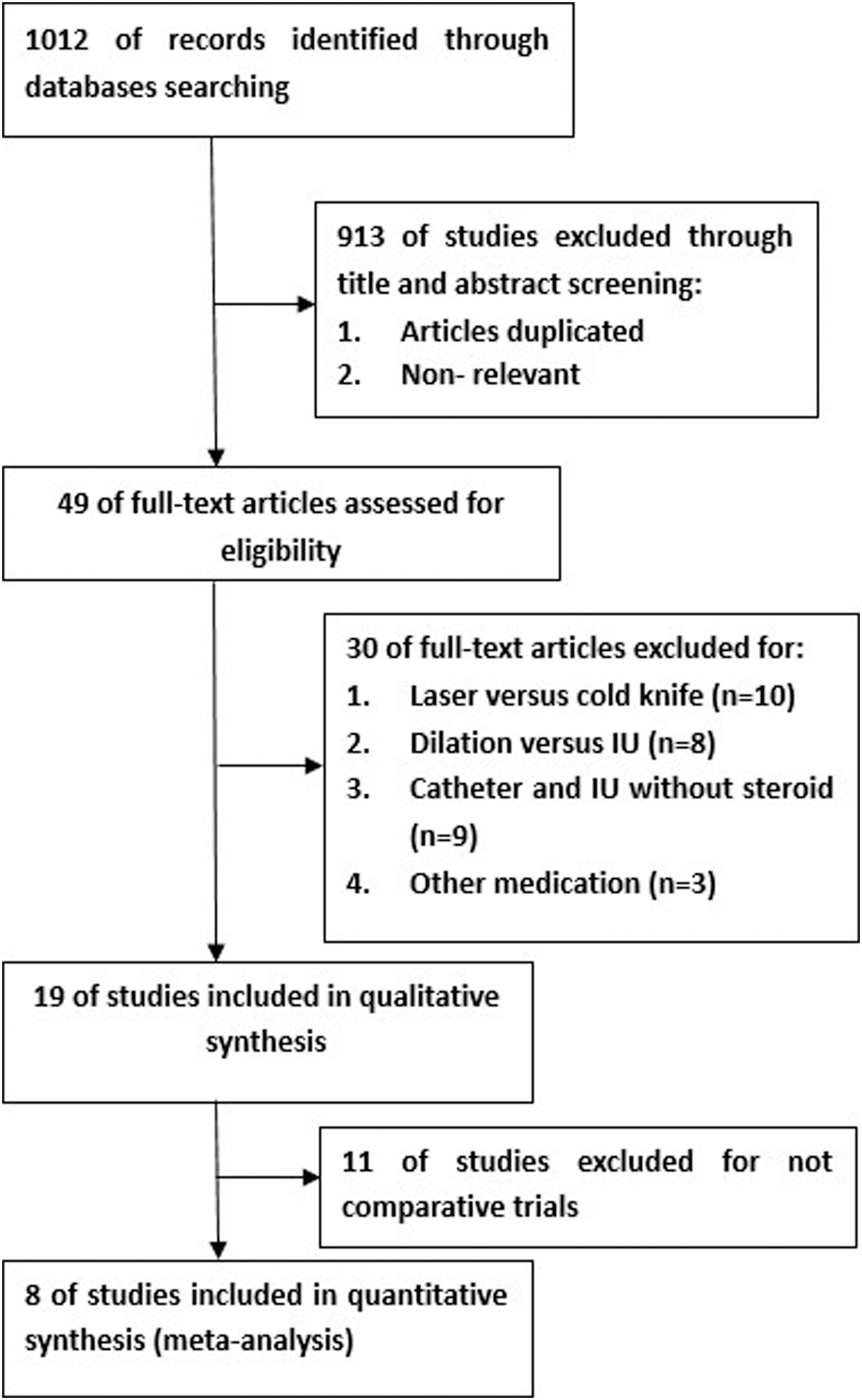
Flow chart depicting systematic incorporation of articles into the review.
Study characteristics
Table 1 lists characteristics of the included studies. There were 469 participants in the eight studies; all of these patients were scheduled to receive IU and 203 of the patients were in experimental groups with local steroid treatment. The steroid supplementations and procedures are described in Table 1. In five studies, steroids were injected into the fibrotic tissue of the stricture site of patients after IU. In the other three studies, the catheters for dilatation were lubricated with steroid ointment. The methodological quality scores of eight studies are also displayed in Table 1. Scores lower than 3 indicate a poorer quality of methodology. Disagreement between two assessors was resolved by discussion with two senior authors (Q. Fu, and Y.L. Sa).
RCT=randomized, controlled study.
Recurrence rates
Recurrence rates were recorded in the follow-up period. Eight studies with a total of 469 patients were eligible to measure the recurrence rate of IU with local steroid application, as seen in Figure 2. Recurrence of urethra stricture was defined by the need for a new procedure in the follow-up period. We applied the fixed model because the quantity of I2 was less than 50%. The difference between recurrence rates was not statistically significant between IUs with steroids and IUs without steroids in each subgroup. The differences between subgroups of steroid injections with either Jadad scores ≥3 (WMD=0.53; 95% CI, 0.25–1.13, P=0.10) or those with Jadad scores <3 (WMD=0.6; 95% CI, 0.27–1.35, P=0.22) were not significant. Similarly, there was no statistically significant difference in the subgroup with catheters coated with the steroid lubrication (WMD=0.51; 95% CI, 0.24–1.10, P=0.09).
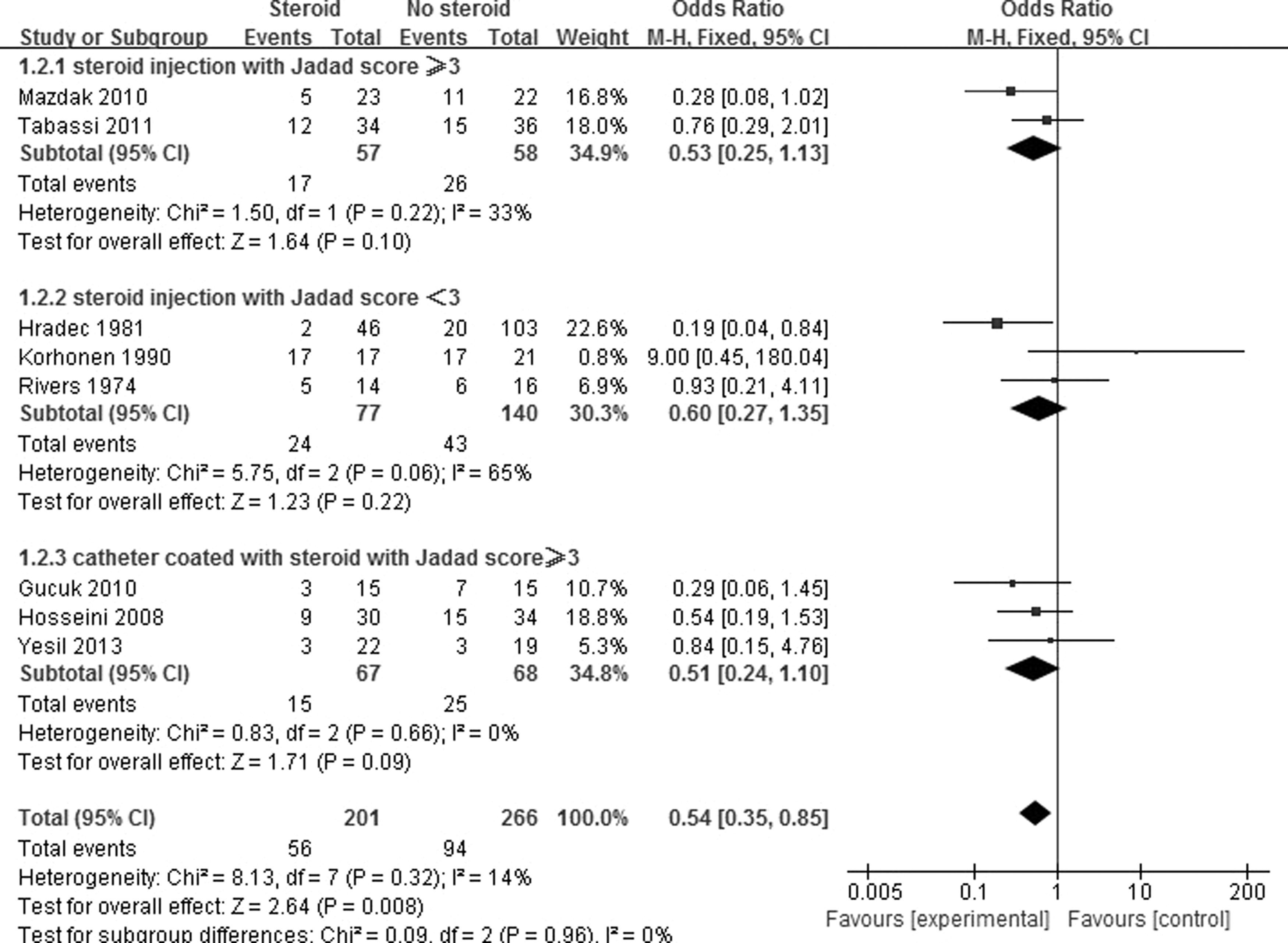
Comparison of recurrence rates between local steroid application and no steroid application. A square indicates dichotomous outcomes, and the size of each square indicates the weight of each study. The diamond signifies that the mean difference is in favor of the local steroid application group.
Time to recurrence
The time to recurrence after initial IU was analyzed in three studies. In two studies of steroid injection (Fig. 3), the time of recurrence was reported with continuous variable. The months of recurrence of the steroid groups in two continuous variable studies were longer than the group without local steroid use. The difference was statistically significant (WMD=4.43; 95% CI, 2.77–6.09, P<0.00001). In the study that used catheters, time was recorded with dichotomous variable (Fig. 4); the number of patients with recurrence was recorded and valued at three follow-up time points. The differences between the patients with recurrence at the follow-up time points were statistically significant (WMD=0.29; 95% CI, 0.08–1.00, P=0.05).

Comparison of time to recurrence between local steroid injection and no steroid use. SD=standard deviation.

Comparison of the number of recurrence at each follow-up time point between catheters coated with steroids and no steroid use.
Adverse effects
Adverse effects of IU with local steroid application were reported in three out of eight studies (Fig. 5) Of the 24 patients with recorded adverse effects, 10 contracted an infection, 6 experienced bleeding, and 8 had extravasation. The adverse effects rate was similar between the patients treated with steroids and those without steroids. There was no statistically significant different between the two groups' total number of adverse effects (WMD=1.59; 95% CI, 0.71–3.58, P=0.26).
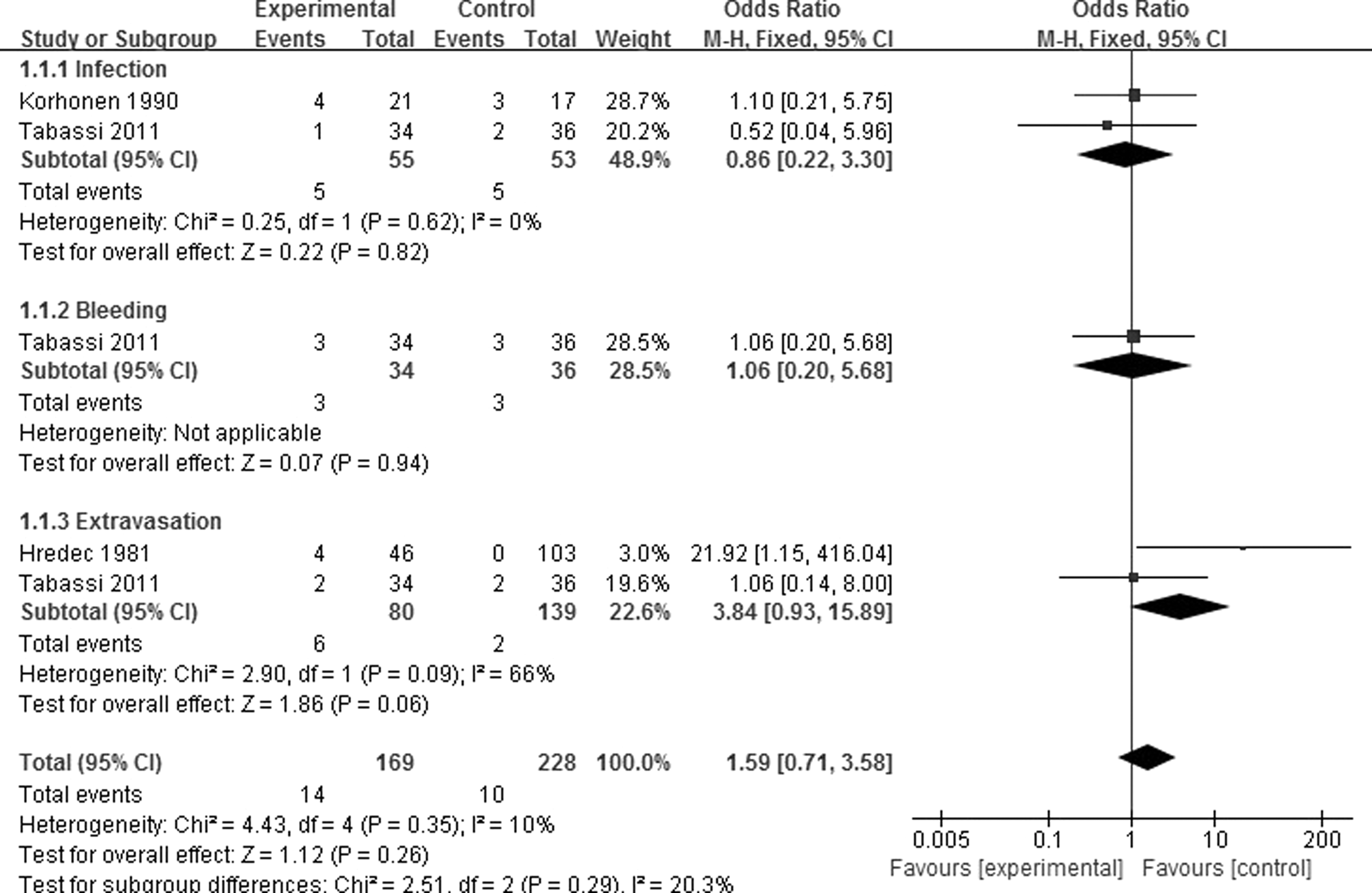
Comparison of adverse effects between steroid injection and no steroid use.
Qmax
In two studies, Qmax was recorded preoperatively and at each follow-up (Fig. 6). The preoperative baseline of Qmax was similar (P=0.53), and all the Qmax time points between the patients treated with steroids and those without steroids was similar without statistically significant difference (WMD=0.11; 95% CI, 0.49–0.72, P=0.71).

Comparison of Qmax between catheters coated with steroids and no steroid use. SD=standard deviation.
Discussion
Our meta-analysis of the currently available literatures indicates that local steroid injection or lubrication could be a safe adjuvant therapy. The outcomes showed that it could not affect the recurrence rate and Qmax significantly; however, it could significantly delay the time to recurrence in patients undergoing IU for urethra stricture.
IU has gained an important place in the management of urethral stricture since the 1980s. 10 Although it has been suggested as the procedure of choice for correction of urethral strictures shorter than 1.5 cm, recurrence of strictures has remained a major drawback. 11 Pansadoro et al. 12 reported a curative success rate of 30% to 35%, and in 2010 Santucci et al. 13 published even worse success rates of less than 10%. These low success rates suggest the need for the development of adjuvant techniques to prevent wound contraction and thus recurrent stricture formation. Even the use of techniques such as Foley catheter placement, self-catheterization, and the use of urethral stents has unfortunately proven to be insufficient in the long-term. 5
Local steroid therapy for urethral strictures without IU originated in 1965. 14,15 In their 1976 retrospective study of steroid management of urethral strictures, Sharp and Finney 16 observed 96 patients for 1 year after urethral injection with triamcinolone. The authors suggested that this treatment was especially helpful in cases with strictures in the distal urethra or the meatus. Uemura and colleagues 17 reported three cases of urethral stricture due to balanitis xerotica obliterans after hypospadias repair. They employed topical steroid ointment or sublesional triamcinolone injection after complete excision of the affected urethra and achieved satisfactory outcomes. Garcia-Alix et al. 18 reported three patients with severe hypospadias (scrotal and perineal) with histories of multiple operations for that condition and postoperative urethral stenosis at different sites. Enlargement was performed using oral mucosa graft in two cases and a local flap in the third. Urethral stricture recurred in all cases very soon after surgery, and repeated dilations did not improve the symptoms. Subsequently, the patients had repeated triamcinolone injections at hypertrophic scar and keloid sites in the urethral lumen every 2 to 3 months. Follow-up ranged between 5 and 20 months, by the end of which all patients were symptom free.
More researchers would like to combine injection of triamcinolone or other steroids with IU. In their retrospective study of patients from 1976 to 1978, Hradec and colleagues 19 observed 149 patients with IU and followed up 1 to 3 years postoperatively. In the series of patients treated by urethrotomy without corticoid injection, the rate of recurrent stricture was 19.4%. Using a specially constructed needle for injection of triamcinolone acetonide, the recurrence rate was reduced to 4.3%. Gaches et al. 20 reported a multicenter survey of 197 cases involving 322 urethrotomy procedures from 5 urological departments in England. The authors recommended the additional injection of triamcinalone acetate into the strictured area before urethrotomy in resistant cases. Rivers and colleagues 21 achieved less encouraging results, however. In their study, the combination of IU with intralesional corticosteroid injections resulted in a failure rate of 44%. Tavakkoli Tabassi et al. 6 performed a double-blind, randomized, placebo-controlled study on 70 patients with urethral stricture. Complication and recurrence rates in the experimental group were lower than the control group, but the difference was not statistically significant. Whereas, time to recurrence decreased significantly in the experimental group. No complications could be attributed to the steroid injections, so it seems that steroid injection is a safe method and may delay the recurrence of urethral stricture. Korhonen and associates 7 treated one group in their study with IU and intralesional methylprednisolone injections with a flexible needle through the cystoscope. The total success rate was only 11%, and 71% of patients in this group had to be treated operatively for a recurrent stricture.
Gucuk and colleagues 5 suggested using a catheter coated with steroid to dilate the urethra instead of injection because the effect of steroid injections is short and difficult to repeat. Furthermore, injections themselves might contribute to scar formation via the traumatic effect of the needle. Mazdak et al. 8 randomized 50 male patients with anterior urethral stricture into 2 groups. The authors demonstrated that the injection of triamcinolone significantly reduced stricture recurrence after IU, with a mean follow-up of 13.5 (±5.5) months postoperatively. In 2012, Kumar et al. 22 evaluated the outcome of IU with the holmium laser along with intralesional triamcinolone injection in 50 patients. All patients were followed up for 12 months postoperatively by history and uroflowmetry. Twelve patients (24%) developed recurrent urethral strictures. The authors discovered that the success rate in patients with strictures <1 cm in length was 95.8%. Kamp and colleagues 23 used IU with a holmium:YAG laser as a minimally invasive treatment for urethral stricture in 32 male patients. Triamcinolone was instilled intraurethrally after removal of the catheter. After a mean follow-up of 27 months (range 13–38 months) 24 of the 32 patients were considered successful, although a urinary tract infection was diagnosed in 5% of patients postoperatively. Overall, the efficacy and safety of local steroid injection after IU is still a controversial issue.
The present study demonstrated that no life-threatening adverse effects occurred in patients undergoing IU with the lubrication of steroid. The reported adverse effects in local steroid injection included local infection, bleeding, and extravasation. These were similar to the data of the placebo or control group. This result suggested that these adverse effects could be the result of the IU procedure instead of the steroid supplementation. Augspurger et al., 24 however, reported two cases of Cushing syndrome following intralesional triamcinolone acetonide injections of urethral strictures in children. Graversen et al. 25 reported that 11 out of 104 patients (10.6%) experienced partial or total erectile dysfunction following IU; most of these patients had distal and long strictures. There was no report of sexual potency in the eight studies included within our study.
The limitations of this meta-analysis include the small number of participants in each study, which could be insufficient to achieve a conclusive result. There are also relevant differences in the reviewed literature. For example, Gucuk 5 discharged patients with the indwelling catheter within 2 weeks. Considering Albers' paper, 26 catheters should not be left more than 3 days. Hosseini and colleagues 9 included 35 patients after urethroplasty, but this is a completely different situation than a primary urethral stricture that could influence the outcome of IU. Tabassi 6 had only a mean follow-up of 8.68 months, which seems to be not long enough given that recurrence occurs within the first 12 months.
Conclusion
Altogether, IU does not appear to be an ideal treatment option and should only be applied in selected cases with very short strictures, no stricture recurrence, or older and unfit patients. Steroid application might be considered in conjunction with IU in order to prolong stricture recurrence. Robust and well-designed randomized, controlled trials are still warranted.
Footnotes
Disclosure Statement
No competing financial interests exist.