
Abstract
Purpose:
To evaluate the perception of urologists who have participated in live case demonstrations (LCDs) regarding safety, educational value/benefits, and ethics.
Methods:
A 19-question anonymous survey was sent to urologists who performed and/or moderated LCDs at the World Congress of Endourology meetings from 2008 to 2012. E-survey was distributed via e-mail, and automatic reminders were sent 2 weeks after original distribution if no response was obtained.
Results:
Eighty-one percent (92/113) of the urologists responded to the survey of whom 75% practice full time in an academic setting. Only 48.0% were fellowship trained, however. More than 60% had performed more than five LCDs at their home and/or away institutions. Performing LCD at an away institution was associated with a higher level of anxiety when compared with performing LCDs at a home institution (79.8% vs 34.6%; P<0.01). Respondents considered film equipment and crew; audience and moderator discussions; unfamiliar team, instruments and tools; language barrier; and having to narrate the procedure, as distractors. Seventy-nine percent considered LCD as an ethical practice, and 90.5% regarded LCDs as a “beneficial” and a “great way” to educate. Similarly, considering the various factors and conditions associated with LCDs, 95% would agree to participate in another LCD.
Conclusion:
LCDs are perceived to be an effective mode of education by performers and moderators of LCDs. Standard guidelines and policies are needed, however, for the selection of patient, surgeon and team, equipment, and facility. Studies are needed to evaluate the impact of this education process.
Introduction
D

Massachusetts General Hospital Ether Dome. Dr. John C. Warren performs the first surgery without pain as William Morton administers ether (1846).
While these LCDs offered many in the audience clinical knowledge and skills, they also provided an arena for drama, suspense, and showmanship. Certainly, concerns with this practice existed pertaining to quality of patient care, safety, and ethics. In the modern era, the use of video transmission of surgical techniques had been suggested for education purposes. 1 Benefits of video transmission include the preservation of a “sterile” operative theater with minimal traffic and input from the audience. As the field of endourology developed, however, the interface between surgeon and patient has transitioned from the actual patient body to a monitor. This has lended itself to adaptation of LCDs for facile demonstration of beneficial how-to and mesmerizing display at many national and international meetings. Despite these technologic advancements, concerns regarding this practice still exist. We have previously reported on the perception of genitourinary surgeons performing LCDs 3 and viewers of LCDs 4 with respect to patient care, ethics, and moral principles. Similarly, few have reported on the issues demonstrators face inherent to modern LCDs, safety, and quality of care associated with LCDs, especially within the urologic community. 1,3,5
While several organizations have policies guiding the use of LCDs (Table 1), no such policies or guidelines exist among urologic associations within the United States. Most recently, the European Association of Urology (EAU) presented its guidelines for LCDs, but its publication is still pending. In this study, we evaluated the perception of urologists who have performed LCDs during the World Congress of Endourology (WCE) regarding safety, educational value/benefits, and ethics pertaining to LCDs. Our goal is to lay the groundwork needed to be able to develop and propose a set of guidelines to guide urologists and associations/societies within the urologic community performing or organizing LCDs either at their home or away institutions or at professional meetings.
Adapted from Duty et al. 3
Reprinted from Urology, 79/5, Brian Duty, Zhamshid Okhunov, Justin Friedlander, Zeph Okeke, and Arthur Smith, “Live Surgical Demonstrations: An Old, but Increasingly Controversial Practice,” 1185.e7–1185e11, May 2012, with permission from Elsevier.
Methods
We obtained a list of all urology faculty who performed or moderated a LCD at any WCE from 2008 to 2012. E-mail list was obtained from the Endourological Society, and the list was validated by cross-referencing the addresses with programs from the WCE for the appropriate years. A 19-question anonymous survey was sent to the 113 urologists who met our criteria. The survey was composed of multiple-choice questions with provisions for additional open-ended response where appropriate. The questions focused on demographics (three questions); experience with LCDs (five questions); appropriateness of LCDs (two questions); negative aspects/barriers of LCDs (three questions); ethics (three questions); and general perceptions regarding LCDs (three questions).
Our survey was constructed by several experts in the field with safeguards in place to identify inappropriate or inconsistent response. The survey was posted on the SurveyMonkey® website, and an e-mail containing the link was sent to the study cohort. An automated e-mail reminder was sent to those who did not complete the survey within 2 weeks. Participant responses were downloaded into a spreadsheet once the survey was closed for analysis. Descriptive statistics were used to summarize the results, and the Fisher exact and Mantel-Haenszel chi-square tests were used for comparison of variables at 0.05 level of significance.
Results
Of the 113 urologists to whom the survey link was e-mailed, a total of 92 (81.4% response) completed the 19 multiple-choice question survey. Of those who participated, at least 86% (79/92) responded to each of the 19 questions.
Demographics
The demographic characteristics of the cohort are shown in Table 2. The median age group of respondents was 45 to 54 years. Of the 86 participants who responded to the survey, most were from Europe and North America, and 75% practice full time in an academic setting.
n=90.
n=85.
LCD=live case demonstrations.
Experience with LCDs
Only 48.0% of respondents were fellowship trained, and 7.6% of participants have neither completed fellowship training/formal course nor performed the demonstrated case at a high volume (Fig. 2). Younger LCD performers were more likely be fellowship trained: 75.0%, 39.5%, 31.6%, and 0.0% for 30–44, 45–54, 55–64, and >65 years age groups, respectively (P=0.0007). As presented in Table 2, nearly all respondents had performed at least one LCD, with 61.2% and 64.7% having performed six or more LCDs at their home institutions and at away institutions, respectively. Similarly, 62.4% of respondents had moderated six or more LCDs.

Training attained by performers of live case demonstrations.
Appropriateness of LCDs
Interestingly, among those who had performed LCDs at away institutions, only 30.1% (25/83) reported that the host organization selected an appropriate case for the technique they were assigned to demonstrate (with respect to patient anatomy and pathology vs procedure indications and contraindications). In as often as 1 in 5 and 6 in 10 cases, 65.1% (54/83) and 4.8% (4/83) reported that the case selected by the host organization for LCDs was inappropriate; however, 75.6% (62/82) indicated that the technical complexity of the cases they performed was appropriate for LCDs while 22% (18/82) and 2.4% (2/82) reported that, on average, the cases were slightly too difficult or far too difficult, respectively.
Barriers of LCDs
As shown in Figure 3, performing LCD at an away institution was associated with higher level of anxiety when compared with performing LCD at a home institution. Overall anxiety was “moderate” to “very high” for 79.8% (63/79) of respondents performing LCDs at an away institution compared with 34.6% (28/81) for those performing LCDs at their home institution (P<0.01). The following were considered to be distracting by the respondents: Film equipment and crew (32.1%); audience and moderator discussions (45.7%); unfamiliar instruments and tools (66.2%); unfamiliar team (67.5%); having to narrate to the audience through procedure (43.2%). With respect to operating in a foreign land, 22.6% (19/84) reported that they have experienced language barriers/translation issues that negatively impacted their case. Other less frequent distractors or barriers reported include: Fatigue, jet lag, and accents of observers.
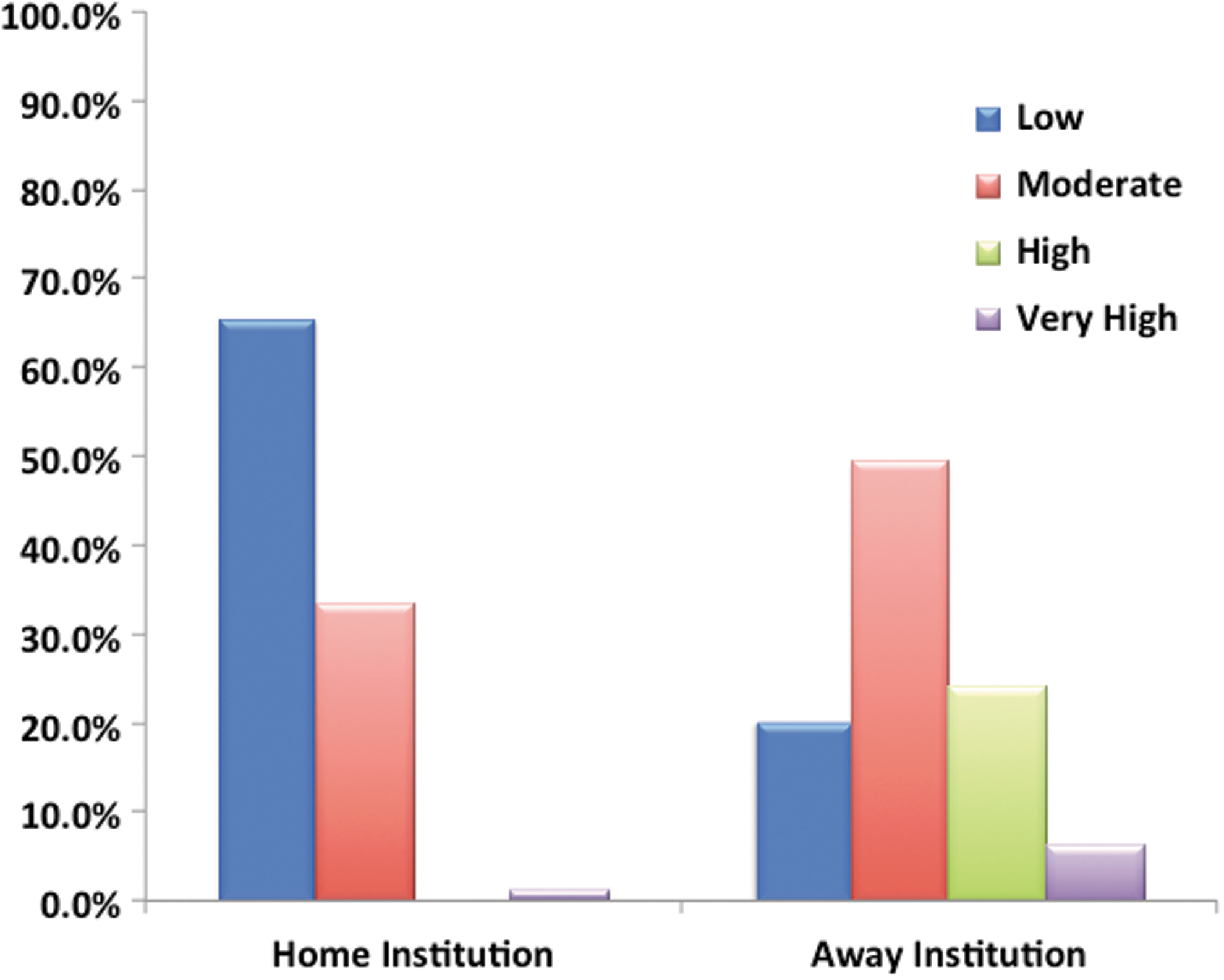
Anxiety levels of performers of live case demonstrations at home and away institutions.
Ethical considerations
Fifty-nine percent (48/82) of respondents reported patient operative care was not delayed as a result of the LCD. Although 41.4 % (34/82) reported that patient operative care was delayed, only in 2.4% of cases overall did the delay negatively impacted patient's clinical care. Furthermore, of performers/moderators of LCD who regarded LCDs as an ethical practice, 79.2% (57/72) were more likely to allow themselves or a family member to be a patient in a LCD compared with 25% (3/12) who did not regard LCDs as ethical (P<0.001).
General perceptions regarding LCDs
Considering the various factors and conditions associated with LCDs, 95.2% (80/84) would agree to participate in another LCD. Respondents' ethical view of LCDs, however, did not appear to affect their decision to or not to participate in another LCD (P=0.096). Although 35.7% (30/84) reported that the benefits of LCDs are limited to increasing attendance at meetings, 90.5% (76/84) overall considered LCDs as beneficial and a great way to educate. On the contrary, 35.7% (30/84) would prefer LCDs to be replaced by edited or unedited surgical videos. All 54 respondents who would not want LCDs to be replaced by surgical videos because of interactions afforded by LCDs would agree to participate in another LCD (P=0.001), however.
Discussion
The field of urologic surgery has witnessed significant changes over the past few decades. Surgical technology and innovation have been widely applied to most urologic procedures and, in fact, have led to the development of an entire subspecialty—endourology. The rapid pace of development has necessitated the facile, concise, and clear method of propagating such operative knowledge to those in training and in practice alike. Thus, LCDs have recently become a routine part of regional, national, and international urologic meetings, often featured as an effective way of educating and promoting novel surgical technology and techniques. 6
Such demonstrations are not without controversy, however. Many have feared that LCDs are fraught with conflicts of interest and may ultimately be detrimental to patient safety and privacy. In fact, Duty and associates 3 noted in a survey of 90 members (50% response) of the American Association of Genitourinary Surgeons that 43.9% were concerned over the appropriateness of LCDs. Although 70.9% of the respondents regarded LCDs as being morally ethical, only 30.1% stated that LCDs should continue in their present form, suggesting that guidelines are needed.
While the urologic community has often been at the forefront of technologic development and the use of LCDs for its promotion and distribution, they are behind the curve with respect to the regulation of such practices. In fact, many societies within medicine/surgery (other than urology) have adapted policy statements or guidelines intended to limit conflicts of interest and patient harm associated with LCDs, even before the urologic literature has evaluated this practice (Table 1). 7 –9 Only recently has the first urologic society to develop rules governing the use of LCDs announced its policy. Their practice uses a central registration process, common consent, and the assigning of a patient advocate. They also require that the audience not be able to ask questions from the surgeon directly, but rather a discussion be held through moderators located both within the audience and with the surgeon. Furthermore, data on all LCDs should be kept in a central location within the EAU for ongoing evaluation. Meetings/events showcasing such sanctioned LCDs need to obtain a certificate from the EAU. 10
The Endourological Society (ES) currently lacks similar guidelines, despite sanctioning many LCDs. Recently, the literature has witnessed a robust discussion regarding the risks and benefits of LCDs. This is of particular relevance to the ES because endourologic cases are, arguably, the most amenable to video transmission to a large audience. Our survey targets members of the ES who had performed and/or moderated laparoscopic, robotic, or endoscopic LCDs during any of the WCE meetings from 2008 to 2012. In our current study, 79.2% considered LCDs as an ethical practice with 95.2% agreeing to participate in another LCD, suggesting that most urologists who had participated in a LCD see a need for its continued use. Furthermore, most respondents regarded LCDs as a great way to educate, and 79.2% will allow themselves or a family member to be a patient in a LCD. These findings are similar to those of Sugarman and colleagues, 11 who surveyed faculty and attendees of LCDs sponsored by Vascular Interventional Advances in 2009 and 2010. They reported that 71% to 76% would allow a family member or a friend to be a patient in a LCD, although only 44% to 58% would agree to be a patient in a LCD.
One of the concerns of LCDs, however, is the safety and quality of care offered to the patients used. Live robotic surgery has been shown to result in equivalent outcomes when compared with similar surgeries performed under standard operating procedures without live broadcast. In a retrospective analysis comparing robotic-assisted laparoscopic partial nephrectomy (RAPN; n=39) performed in LCDs with those performed without live broadcast (n=847), Mullins and coworkers 5 reported no difference between operative times (196.3 vs 183.8 min; P=0.22), estimated blood loss (187.8 vs 190.7; P=0.93), warm ischemia time (20.8 vs 18.8; P=0.17), length of stay (2.8 vs 2.8 days; P=0.99), positive surgical margin rate (2.6% vs 2.3%; P=0.83), and complication rates (5.1% vs 12.8%; P=0.16). 5 This was a retrospective study with the potential for selection bias, however, and it may be difficult to quantify how many cases are needed to be able to safely and effectively perform a LCD. Mullins and colleagues 5 reported, though, that each surgeon before performing a LCD had performed an average of 51.3 cases of RAPNs. This suggests that experience is certainly needed to be able to perform a LCD.
Our survey reveals that most performers of LCDs are recognized experts in their fields, and most of them had performed at least 1 LCD, with the majority having performed more than 10 LCDs. A concerning finding from our survey, however, was that almost 10% had no previous formal training in the particular procedure they demonstrated. This again highlights the need for the formulation of guidelines regarding LCDs that will guide surgeon selection for LCDs at professional meetings. It is noteworthy that the anxiety of the surgeon may impact the quality of care and safety of patients used in LCDs. 12 We found that anxiety was significantly higher among those performing LCDs at away institutions compared with performing LCDs at home institutions, consistent with the findings of Khan and associates 12 in a survey of European urologists who performed live surgical broadcasts.
Given the issues associated with LCDs, possible alternatives, including surgical videos (edited or unedited), LCDs at the home institution with videoconferencing, and minifellowships, have been proposed. These are expected to eliminate some of the associated anxiety, cost, and fatigue from travel. Some of the concerns with this mode of education, however, are the picture and sound quality of the media transmitted over the Internet. The application of international videoconferencing for laparoscopic surgery has been evaluated in the general surgery literature. In an evaluation of 129 respondents who attended a laparoscopic surgery (gastrectomy, pancreatectomy, and colectomy) demonstration via the Internet, Huang and coworkers 13 reported only a 0.3 second delay in transmission and a 0% packet loss in video data. In the cases demonstrated, the quality of the image and sound were reported to be good to excellent in 97.7% and 87.6% of cases, respectively. The possibility of interaction between surgeons and attendees was not reported, however.
Our survey showed that 64.3% would not want LCDs to be replaced by surgical videos because the interactions afforded by LCDs cannot be mimicked by videos. Furthermore, 91.5% overall considered LCDs to be a beneficial and great way to educate. These findings from our study are comparable to those of Sugarman and colleagues, 11 who reported that 70% to 82% of respondents of their survey were of the opinion that LCDs are more valuable than watching a prerecorded video.
Some other ethical issues surrounding LCDs are factors influencing patient selection, delay in treatment or deviation from what is considered routine medical care, and appropriateness of indications for treatment. 14 In a review of 168 live endoscopic retrograde cholangiopancreaticography cases demonstrated over a 12-year period, Schmit and associates 15 reported that procedures were delayed (by an average of 9 days) in 10.7% of cases, and these patients were more likely to undergo general anesthesia (87.5% for LCDs vs 44% for controls; P<0.001). The success and complication rates were reported to be comparable, however. Similarly Eliyahu and coworkers, 16 in a review of 101 patients who underwent interventional cardiovascular procedures performed in the setting of LCDs, reported similar immediate and 30-day clinical outcomes compared with those of routine clinical practice and those published in the literature. Although 41.4% of respondents in our study reported that the patient's operative care was delayed, only in 2.4% of cases did the delay negatively impacted the patient's clinical care.
A limitation of our study is its retrospective nature, which may be associated with recall bias. For example, a surgeon who had an overall good experience with LCDs may not recollect the level of anxiety associated with the case. Also, we were unable to evaluate the specific procedures performed during LCDs, which may be associated with varying levels of anxiety or stressors. Furthermore, the results of our study are based on a survey completed by the performers of LCDs themselves and may be limited by reporter bias, given that physicians may be poor at judging themselves.
The results from our study indicate, however, that the ES must mitigate potential concerns with a uniform regulated standard for LCD. In exchange, such LCDs would not only be safer for both patient and surgeon, but possibly more educational for the viewer. Such LCDs would merit the endorsement of the ES and set them apart from unsanctioned events. We propose the following points for possible consideration: 1. If possible, LCDs be performed at the surgeon's home institution and be telecast using high quality transmission means. For LCDs to be performed at an outside institution, however, an indication conference should be held to assess the suitability of the case and all concerns addressed before approving the case. The ES should avoid endorsing LCDs performed by a visiting surgeon that may be susceptible to challenges of unfamiliar operating room setting/team or less ideal patient factors outside of the surgeon's control. 2. LCDs be performed by surgeons deemed to be experts within the field. The definition of expert may be based on previous surgical volume, previous LCD experience, or other predefined metric. 3. LCDs be moderated with an ES representative within the operating room who will serve as a filter between the moderators in the audience and the surgeon, allowing for direct discussion with the surgeon only during appropriate times (minimizing distraction). 4. The assignment of a patient advocate or patient advocate team within the ES, which will review the credentials of the surgeon and the details of the case to prevent delays in care or deviations from standard of care. Such a council would select a representative that may cease the transmission of the case if standards are not met or in the case of a dangerous situation. 5. All cases entering LCD have a specific patient consent form highlighting possible specific concerns associated with LCD. 6. Prospective data collection of all cases performed in the LCD setting to monitor ongoing safety of such cases compared with a reference standard. 7. The ES provide a disclaimer such that viewers have an idea of what is safely transferrable to practice without further training.
Conclusion
LCDs may be a valuable way to educate surgeons, but there are issues with which performers must be prepared to deal. Well-trained and experienced performers of LCDs may be adversely affected by inappropriate case selection, technical difficulty of cases, anxiety associated with operating at an away institution, and unfamiliar instruments/surgical team. Results from the present study support concerns within the cardiothoracic and endoscopy literature about the continued use of LCDs. Standard guidelines and policies need to be formulated for the selection of patients, the surgeon and team, equipment, and facility.
Footnotes
Disclosure Statement
No competing financial interests exist.