
Abstract
Introduction:
The aim of this in vitro study was to evaluate and compare a novel intracorporeal lithotripter, LithAssist (LA; Cook Medical, Bloomington, IN), with the Swiss LithoClast Ultra (SLU; Boston Scientific, Boston, MA) for the fragmentation and removal of artificial stones made of gypsum-based cement.
Materials and Methods:
Ten soft and 20 hard ultracal-30 (U-30) stones were fragmented using two lithotripters. We recorded the stone weight (grams) prior to placing them into a 60-mL syringe for fragmentation. We inserted a 30F percutaneous access sheath into the syringe and positioned the stone within its lumen. Next, we inserted the lithotripter into a right-angled nephroscope. We recorded the times required for first and complete stone disintegration, disintegration to 2 mm, and complete stone removal for each device. In addition, we recorded the stone mass following each minute of stone fragmentation.
Results:
In total, we subjected 5 soft and 10 hard stones to SLU and LA, respectively. All soft stones were completely disintegrated and removed with both the SLU and LA device. For soft stones, disintegration to 2 mm (2.83±0.41 vs. 4.15±0.70 minutes, p=0.049), complete disintegration (3.18±0.20 vs. 6.40±1.95 minutes, p=0.038), and complete removal (3.30±0.22 vs. 8.82±1.05 minutes, p=0.001) were faster for the SLU compared with the LA. For hard stones, fragmentation was not accomplished with the SLU, whereas with the LA, mean time for first disintegration, disintegration to 2 mm, complete disintegration, and complete removal was 3.60±1.36, 7.25±3.33, 7.54±2.94, and 8.64±2.78 minutes, respectively.
Conclusions:
In this in vitro study, the SLU was more efficient for softer artificial stones, and the LA was more efficient for harder artificial stones.
Introduction
S
There have been several studies that compare both ultrasonic and pneumatic lithotripters to the Ho:YAG laser. 3 –6 Studies have demonstrated that stone fragmentation by the Ho:YAG laser is faster than ultrasonic lithotripsy for harder stone compositions. Moreover, the advantage of Ho:YAG laser is that it offers relatively rapid lithotripsy while minimizing tissue trauma. In addition it is effective against all stone compositions, including cysteine and calcium oxalate monohydrate, where ultrasonic lithotripsy may struggle.
The efficiency of existing Ho:YAG lasers, however, is limited by the need for manual extraction of stone fragments and mobilization of small fragments due to the lack of simultaneous suction. Accordingly, this results in longer operative times to achieve stone-free status. As discussed earlier, currently available ultrasonic lithotripters (i.e., Olympus LUS) combine ultrasound energy with suction capability and newer pneumatic lithotripters (i.e., Boston Scientific Lithoclast Ultra) also include suction capability, in addition to ultrasound energy. Recently, a new disposable handheld device (LithAssist [LA]; Cook Medical, Bloomington, IN) was developed that combines the delivery of a laser fiber with suction capabilities for PCNL applications (Fig. 1). This handheld device has a hollow cylindrical probe with two lumens that allows simultaneous fragmentation of the stone with the laser fiber and suction and extraction of small stone fragments, thereby potentially increasing the effectiveness and efficiency of stone fragmentation and removal. Theoretically this device should efficiently minimize the exchange of instruments, as well as keep the area clear from debris and small stones. The LA device is also the first device that has incorporated a mechanism for the surgeon to easily control the degree of suction during the procedure.

LithAssist (LA) device.
Our objective was to perform an in vitro study to establish the effectiveness and efficiency of this novel device at stone fragmentation and removal and compare it to a currently existing lithotripter to assess its relative effectiveness and efficiency.
Materials and Methods
Study design
We used two types of artificial stones (ultracal-30 [U-30]), hard and soft stones, made from gypsum-based cement (United States Gypsum, Chicago, IL) prepared according to McAteer et al. 7 Hard stones consisted of 30 gypsum-cement and soft stones consisted of two parts, 30 gypsum-cement and 35-μm glass, each ∼14.66-mm in diameter and 3.00 g in weight.
In total, we subjected 5 soft stones and 10 hard stones to combined ultrasonic and pneumatic lithotripsy with the Swiss LithoClast Ultra (SLU; Boston Scientific, Boston, MA) and similarly 5 soft stones and 10 hard stones to laser lithotripsy with the LA (Cook Medical). In this study, we used 940-μm laser fibers (Cook Medical) and Rhapsody H-30™ Holmium Laser System (Cook Medical).
A single urologist with lithotripter experience performed all procedures. At random, we divided the stones (5 soft and 10 hard) and submerged each group in separate water tanks until removed prior to lithotripter evaluation. An artificial stone and lithotripter for evaluation were selected in a randomized manner. The person who was recording the data was blinded to the type of stone and lithotripter. We recorded the weight (grams) of the stone and placed it into a 60-mL Toomey syringe. Next, we inserted a 30F percutaneous sheath into the syringe and placed the stone within the sheath's lumen. An assistant stabilized the access sheath and stone. 8 We set the laser energy and frequency for the LA to 3 J and 10 Hz, and the energy setting to 100% for the SLU (as recommended by the manufacturer). Next, we inserted the chosen lithotripter into a standard right-angled nephroscope (Karl Storz Endoscopy, Tuttlingen, Germany) and inserted the lithotripter into the percutaneous sheath.
Device description
The LA (Fig. 1) is a disposable handheld device that combines the delivery of a laser fiber with suction capabilities for PCNL applications. The device has a 38-cm dual-lumen stainless steel cannula that is attached to an ergonomic handle for control. Within the rigid 11.6F outer-diameter lumen, there rests a 5F internal lumen designed to house the laser fiber. The remaining interior portion of the cannula facilitates the suction of fluid, soft tissue, and stone fragments. A vacuum source attaches to the universal suction port at the base of the LA handle and, as long as the locking trigger is not depressed, the operator can have continuous suction during lithotripsy. Due to the design of the instrument, the operator can actively and precisely control the degree of suction with a single hand, eliminating the need for an assistant. The laser fiber is inserted through the Tuohy-Borst adapter at the rear of the handle and is extended through the cannula until it extends ∼1–2 cm beyond the tip. If desired, the operator can rotate the Tuohy-Borst adapter counterclockwise to secure the laser fiber at the desired length. In combination, these features allow the surgeon to individually and independently control both the delivery of laser energy and suction during PCNL procedures.
The Lithoclast Ultra has been described and extensively evaluated in previous studies. 9,10 As described previously, the Lithoclast Ultra incorporates ultrasonic and pneumatic lithotripters and consists of an ultrasonic handpiece and 3.3-mm-diameter ultrasonic probe, as well as a pneumatic handpiece with a 1-mm probe. Ultrasonic or pneumatic power settings can be utilized separately or simultaneously during the stone treatment. The pneumatic probe is inserted through the ultrasonic handpiece and rests within the probe lumen. The separate handpieces are interlocked. Suction tubing is attached to the ultrasonic portion of the combined handpiece to allow removal of fragments during treatment.
Outcome measures
Each device was evaluated for the mean time until first disintegration of the stone, disintegration of all stone fragments to 2 mm, complete disintegration of the stone, and complete removal of the stone fragments. In addition, we recorded the stone mass following each minute of stone fragmentation and reported the percent disintegration for each minute over time.
Statistical analysis
The mean time for each of the outcome measures was compared across the SLU and LA groups using the Student's t-test. A p-value of <0.05 was used for statistical significance. All statistical analyses were performed using SPSS version 17.0 (SPSS, Inc., Chicago, IL).
Results
We used a total of 10 soft stones and 20 hard stones in the study. All soft stones (n=10) were independently completely disintegrated and removed using both the SLU and LA devices. The mean initial weight of the soft stones treated with each device was equivalent (2.99 g; Table 1). Disintegration and complete removal times are presented in Table 1. The mean time for first disintegration of soft stones was not significantly different for the SLU compared with the LA (1.30 minutes vs. 2.15 minutes, p=0.11). However, the SLU was superior to LA in terms of the mean time for disintegration to 2 mm (2.82 minutes vs. 4.15 minutes, p=0.04) and complete stone disintegration (3.17 minutes vs. 6.39 minutes, p=0.03), respectively. The mean percent disintegration of soft stones over time in minutes for each device is shown in Figure 2. The SLU required a shorter length of time for complete removal of a soft stone compared with the LA (3.30 minutes vs. 8.81 minutes, p=0.001; Table 1 and Fig. 2).

Mean percent disintegration of soft stones over time using LithoClast Ultra and LA (n=5).
LA=LithAssist.
The SLU was not able to fragment hard stones in our study. The mean weight of hard stones in SLU group was 2.59 g. The LA was able to completely disintegrate and remove all hard stones (n=10), which had a mean weight of 2.59 g. The time in minutes for first disintegration of hard stone, disintegration to 2 mm, and complete disintegration was 3.59, 7.24, and 7.54, respectively (Table 2). The mean time for complete removal of the hard stone was 8.64 minutes (Table 2). The mean percent disintegration of hard stones over time in minutes for the LA device is shown in Figure 3.
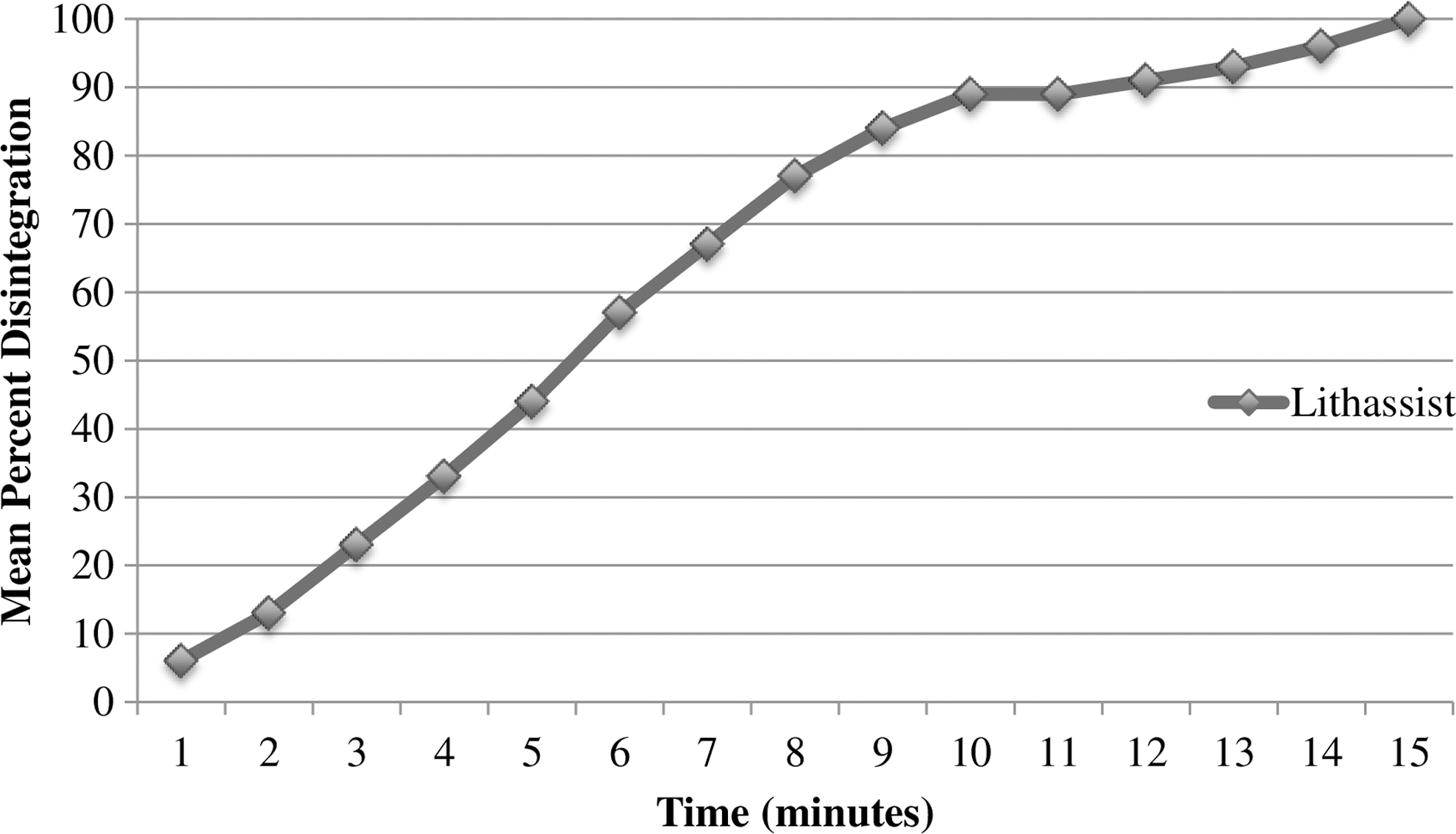
Mean percent disintegration of hard stones over time using LA (n=10).
Discussion
Intracorporeal lithotripters have become an integral component of the surgeon's armamentarium for PCNL procedures. Ultrasonic lithotripters rely on the transmission of high-frequency ultrasonic (piezo-ceramic) waves to fragment large renal calculi. 8 Although the ultrasonic lithotripter is considered the gold standard due to its ability to simultaneously fragment and aspirate the resulting small stone fragments, 11,12 it has been shown to be less effective in fragmenting stones of high dense composition, specifically cystine or calcium oxalate monohydrate. 13 –15 Conversely, the high-powered ballistic energy employed in the pneumatic lithotripter has proven to effectively fragment stones of dense composition. Pneumatic lithotripters, however, lack the ability to aspirate stones. The subsequent extraction of the resulting stone fragments is required and potential stone migration and retropulsion are problematic. 6,16,17
The SLU, introduced in 2002, combined ultrasonic and pneumatic-ballistic energy modalities within a single lithotripter device. The pneumatic probe allows for the fragmentation of dense stones while the ultrasonic probe allows for the fragmentation and removal of softer stones through its hollow probe. When compared with stand-alone ultrasonic and pneumatic lithotripters, the combined SLU demonstrated increased fragmentation and clearance efficiency. 8 –10
Rather than utilize ultrasonic or pneumatic energy, the recently introduced LA device utilizes holmium laser energy to fragment renal calculi. The Ho:YAG laser uses photothermal energy to ablate each calculi, effectively yielding smaller fragments than pulsed dye lasers, mechanical lithotripsy, or electrohydraulic lithotripsy. 18 Additionally, the risk of retropulsion is minimal as compared to alternative modalities. 19
Comparing pneumatic lithotripters to the Ho:YAG laser, Malik and colleagues performed a randomized study that included 60 patients who underwent PCNL. 4 They compared the Ho:YAG laser to a pneumatic lithotripter, for stones ≥2.5 cm, and showed that both lithotrites are effective options for the treatment of large renal calculi. Although the use of the Ho:YAG laser was associated with longer operating times, the pneumatic lithotripter was associated with increased complications. 4 Because the efficiency of the Ho:YAG laser is limited by the need for endoscopic entrapment and extraction of stone fragments due to the lack of simultaneous suction, operative times to achieve stone-free status were longer.
To address this limitation, the LA combines the delivery of holmium laser energy with suction capability. As such, its suction mechanism allows the surgeon to control the degree of suction during PCNL. Theoretically, this device should efficiently minimize the exchange of instruments, as well as keep the area clear from debris and small stones.
As per the literature, stone composition heavily influences the efficacy of each intracorporeal lithotripter. As a result, we selected the U-30 stones, as they have been proven to be an accurate stone model to use in the evaluation of effectiveness of intracorporeal lithotripters. 7,20 Moreover, it has been shown that these artificial stones disintegrate in a similar fashion to traditional stones. 21,22 Thus, the U-30 stones allowed for the controlled and reproducible conditions needed to conduct lithotripter performance testing with minimal variability in stone composition, size, and structure. Additionally, the increased variability in stone composition did permit analysis of the lithotripter performance on stones of varied composition.
In this in vitro study, our data demonstrated that the SLU was superior for fragmentation and removal of stones of softer composition resulting in faster mean times for disintegration to 2 mm, complete disintegration, and complete stone removal when compared with the LA. Prior studies have similarly demonstrated improved fragmentation time with combined pneumatic and ultrasonic lithotripters compared with laser lithotripters. 4,19 It should be noted that we performed this experiment with a 940-μm end-firing fiber using power settings of 3 J and 10 Hz. A previous study performed by Teichman and associates revealed that side-firing fibers were in fact faster and more efficient compared with end-firing fibers. 23 Accordingly, we believe that with a side-firing fiber the performance of LA would likely be improved, with better fragmentation times potentially equivalent to that of the SLU.
Conversely, for stone models of harder composition the LA was superior to the SLU. The LA was able to completely fragment, disintegrate, and remove all stone models of harder composition using the 940-μm laser fiber, whereas the SLU was completely ineffective and unable to fragment the harder stones in our model. The SLU was applied continuously for several minutes with each of the hard stones with no fragmentation observed. This was certainly surprising considering the proven efficacy of the pneumatic component of the SLU at fragmenting stones of harder consistency. However, as would be expected, the Ho:YAG laser demonstrated consistent efficacy at treating stones of varying consistency, especially those of greater density. This certainly underscores the value of the Ho:YAG laser, in particular, when it can now be coupled with advantages of simultaneous suction capability.
No issues with use of the 940-μm laser fiber within the LA device were encountered during the study. However, we did observe some lumen clogging of the LA device cannula by stone fragments. This was easily resolved with slight back and forth movements of the laser fiber, which helps to clean the lumen of the LA cannula and restore suctioning. Overall, suction capability of the novel LA device was efficient in removing all of the small fragments and dust created by the laser fiber.
The principal limitation of this study is the generalizability of the results to the clinical setting and in vivo lithotripsy. The in vitro model utilized in this study, although effective for assessing fragmentation and clearance in a standardized and controlled fashion across the two lithotripter groups, did not completely replicate the in vivo environment. Specifically limited lithotripter manipulation by the operator was possible, and there was relatively no risk of stone migration and subsequent need for endoscopic entrapment and removal. Each stone remained positioned within a 30F percutaneous sheath during evaluation; however, in vivo stone migration is not limited in this fashion. Further evaluation and comparison of the LA with the SLU in a clinical setting will help to address this limitation and determine whether the benefits in stone disintegration and removal seen in the present study translate to improved operative times in the in vivo setting. Notwithstanding this, the goal of this study was to evaluate the in vitro performance of the LA to establish the effectiveness and efficiency of this novel device at stone fragmentation, which was successfully accomplished.
Conclusions
The present study demonstrated that both the SLU and the LA can fragment and remove softer artificial stones. In this regard, the SLU demonstrated faster times for disintegration to 2 mm, complete disintegration, and complete stone removal when compared with the LA. However, for the harder artificial stones, the LA was superior at fragmenting and completely removing harder artificial stones, in the model tested. The next step, which is currently underway, is to conduct a prospective randomized clinical trial to confirm these findings in a clinical setting and assess the impact on operative time and outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.