
Abstract
Aim:
To compare the scars and cosmetic results of trocars of 3, 5, and 10 mm in cases by small-incision access retroperitoneoscopic technique pyeloplasty (SMARTp) and standard laparoscopy pyeloplasty (SLp).
Methods:
Between January 2012 and October 2013, 20 pyeloplasties were performed: 12 with SMARTp and 8 with SLp techniques. A 5-mm homemade balloon trocar was used to create the retroperitoneal space. In SMARTp, 3- and 5-mm trocars were used and in SLp, 5- and 10-mm trocars were used. All patients underwent a ureteral (Double-J) stent placement preoperatively. The study included a total of 72 trocar-site scars: 3 mm (24 scars), 5 mm (24 scars), and 10 mm (24 scars). Cosmetic outcome was assessed at the 3rd, 12th, and 24th month of surgeries by the Observer Scar Assessment Scale (OSAS).
Results:
Mean age was 34.7±10.5 (19–52) years, and mean follow up was 18.7±9.2 months. Fifteen patients (75%) underwent Y-V plasty, and 5 (25%) underwent Anderson–Hynes pyeloplasty. Mean operative time was 125.4±28.7 minutes. There was only minimal blood loss, no need for conversion to standard laparoscopic or open pyeloplasty, no intraoperative complications, and only two postoperative complications were recorded: retroperitoneal hemorrhage and wound infection and both were treated conservatively. There were significant differences between objective questions of “vascularization” in a 3-mm trocar and “thickness” in a 10-mm trocar. Twenty-four months after surgery, the cosmetic data assessed by OSAS showed statistically significant differenecs in favor of the 3-mm trocar sites versus the 10-mm trocar sites (OSAS: 13.8±3.9 vs 24.6±1.7; p=0.006) with no statistically significant difference between 3- and 5-mm port sites.
Conclusions:
The SMARTp is proved to be an efficacious and tolerable procedure with better cosmetic results and can be used for the treatment of ureteropelvic junction obstruction (UPJO) in suitable patients. We believe that this technique is likely to become an established procedure.
Introduction
L
Therefore, new techniques such as laparoendoscopic single-site surgery (LESS), natural orifice transluminal endoscopic surgery, and needlescopic surgery have been previously introduced. 2 –6 Besides these, mini-laparoscopy (ML) has been previously described in laparoscopic urology for transperitoneal approaching by using 3-mm instruments. 2 Thus, functional and cosmetic outcomes were promising. Recently, the novel small-access incision retroperitoneoscopy technique (SMART) has been described in an attempt to improve the cosmetic outcomes, and to reduce the invasiveness of standard laparoscopy (SL). 7 SMART combines the cosmetic advantages of ML with the retroperitoneoscopic approach and it provides direct access to the retroperitoneal organs, potential reduction in time, needs less organ retraction, and eliminates the risk of intraperitoneal contamination, infection, and absence of peritoneal irritation by insufflating carbon dioxide.
There is still a lack of data on the linear scar assessment after laparoscopic surgeries focusing on those cosmetic results using validated scar assessment methods with follow-up data. The Patient and Observer Scar Assessment Scale (POSAS) is a standard way for assessing the scars, and it takes the evaluation of the patients and the observers into account. 8,9
The aim of this study is to compare the linear scars and cosmetic results of our SL (5/10 mm trocar incisions) and SMART (3/5 mm trocar incisions) pyeloplasty cases using the Observer Scar Assessment Scale (OSAS), which is a reliable and suitable tool mostly used for burn and linear scar assessment. 9 In addition, we evaluated the changes in quality of the scars, in different time periods of follow up.
Methods
This was a prospective study. Pre- and postoperative data of patients in whom SMART pyeloplasty (SMARTp) and SL pyeloplasty (SLp) were performed by retroperitoneal route were recorded in a Microsoft excel sheet.
Exclusion criteria were irregular follow up, pediatric patients (age <18 years), previous surgery for UPJO, previous history of major abdominal or pelvic surgery, body mass index (BMI)>30 kg/m2, concomitant urolithiasis, skin disease, known allergies to chemical products, and history of scars or keloids. Nine patients were excluded from the study.
Between January 2012 and October 2013, 20 patients underwent LP. Of the 20 patients, n=12 underwent SMARTp and n=8 underwent SLp. All surgical procedures were performed by a single experienced surgeon (J.R.). In SMARTp cases, 3- and 5-mm trocars were used; while in SRTp, 5- and 10-mm trocars were used. The study included a total of 72 trocar-site scars. Out of the 72 scars, we had 24 scars of each size (3, 5, and 10 mm) (Table 1).
All patients were assessed preoperatively with physical examination, abdominal ultrasound, intravenous urography, or computed tomography scan and renal scintigraphy. Demographic, perioperative data and data on complications were recorded and classified according to the Clavien system.
The SMARTp and SLp surgical techniques were previously described in detail. 7 Briefly, after a 5-mm incision, a homemade balloon trocar was used for creating retroperitoneal space. Subsequently, a 5-mm trocar (10.5 mm length) was introduced as an optical port through the same incision. After performing the surgery by using 3- and 5-mm trocars, the 5 mm port site incision was closed by only a single stitch and the 3.5-mm incision was closed by adhesive material (Dermabond®, San Lorenzo, CA).
We objectively evaluated the cosmetic results based on a standardized assessment score system—the OSAS developed by plastic surgeons to evaluate scars. 9 The OSAS consists of numeric scale and contains six items: vascularity, pigmentation, thickness, relief, pliability, and surface area. Each item scored numerically on a ten-point scale. The lowest score for each item in the scale is 1, and it corresponds to the normal skin; the highest score is 10, and it corresponds to the worst scar situation. To objectively assess scars, the OSAS scores of two observers (urologists) not directly involved in surgery were taken into consideration for statistical analysis. The evaluations were made with the observers blinded to each other. The urologists evaluated scars by OSAS scoring at the 3rd, 12th, and 24th month of surgery.
In statistical analysis, descriptive results were reported for all studied parameters. The one-way Anova was used for statistical analysis. Statistical significance was considered at p<0.05. All statistical analyses were performed with the Statistical Package for Social Sciences (SPSS) for windows 16.0 (SPSS, Inc., Chicago, IL).
Results
Out of the 20 patients included in the study, 10 were men and 10 were women with the mean age of 34.7±10.5 (19–52) years. All the patients were Caucasian race with 12 patients included in the SMARTp group and 8 patients included in the SLp group. Fifteen patients (75%) underwent Y-V plasty, and 5 (25%) underwent Anderson–Hynes pyeloplasty. Mean operative time was 125.4±28.7 minutes. There was only minimal blood loss, no need for conversion to standard laparoscopic or open pyeloplasty, no intraoperative complications, and only two postoperative complications were recorded in the SLp: one retroperitoneal hemorrhage and one wound infection, both had a Clavian category 1 or 2 complication and were treated conservatively.
There were no statistically significant differences between the two groups in age and BMI. Mean follow up was 18.7±9.2 months. Demographic, operative, and follow-up data were summarized in Table 2.
ASA=American Society of Anesthesiologists; BMI=body mass index (kg/m2), UTI=urinary tract infection; VAS=visual analogue scale.
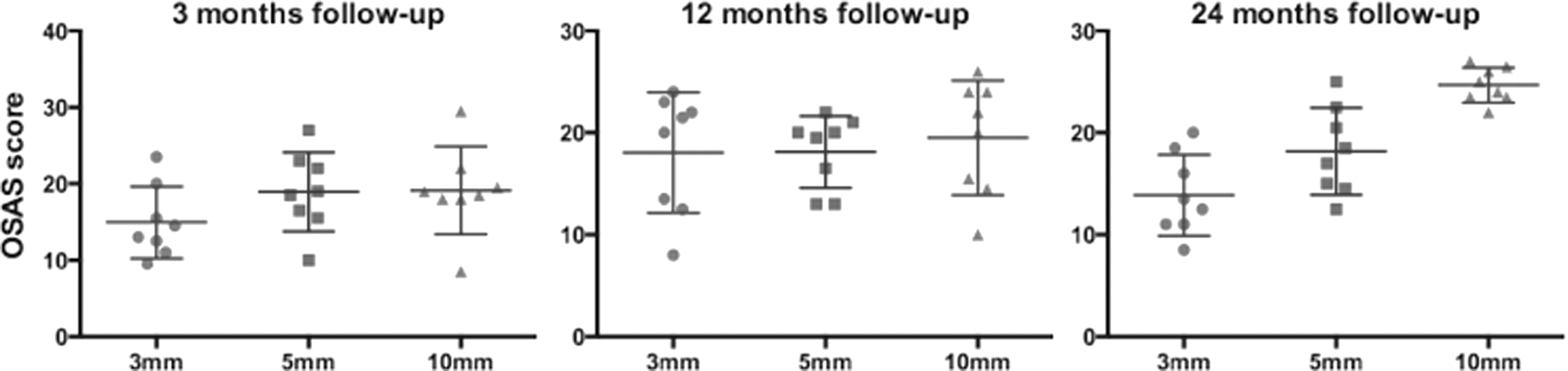
In the scar assessment, the overall mean OSAS evaluating 3-, 5-, and 10-mm trocar sites showed no significant difference among them during the first year of follow up (Figs. 1 and 2).
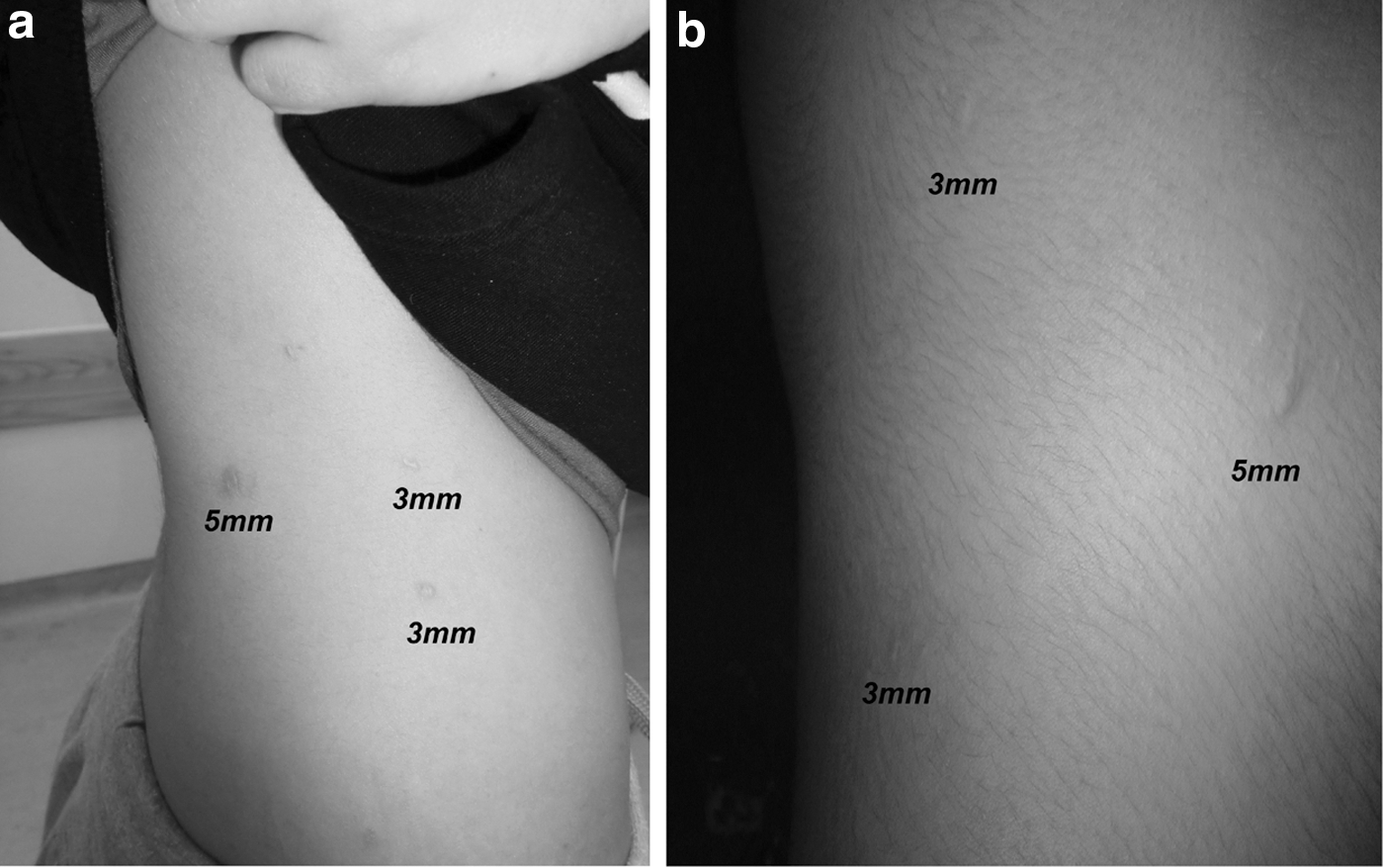
Appearance of 3- and 5-mm scars at 3

Appearance of 5- and 10-mm scars at 3
OSAS Single objective question “pigmentation,” “relief,” and “pliability” showed no statistically significant difference between the three port sites scars during the whole period of follow up. We found significant differences between objective questions of “vascularization” in a 3-mm trocar and “thickness” in a 10-mm trocar (Table 3). Vascularization of the 5-mm port site at a 3 month follow up was statistically significantly higher than that of the 3-mm port site at 3 and 24 months (p<0.05). The OSAS questionnaire of “Surface area” showed statistically significant differences in favor of the 3-mm port site when compared with the 10-mm port site at 3rd, 12th, and 24th month of follow up (p<0.05). Similarly, “thickness” in OSAS scoring showed statistically significant differences in favor of the 3-mm port site scars compared with the 5- and 10-mm sites at 24 months of follow up (p<0.04).
Statistically significant p-value.
However, 24 months after surgery, the cosmetic data assessed by OSAS showed statistically significant differences in favor of the 3-mm trocar sites versus the 10-mm sites (OSAS: 13.8±3.9 vs 24.6±1.7; p=0.006) (Fig. 3) with no statistically significant difference between 3- and 5-mm port sites. In addition, the overall comparison at 24 months showed no statistically significant difference between the three port site scars (p=0.1).
Statistically significant comparison between 3-, 5-, and 10-mm trocar site scars during the follow-up period.
Discussion
Scars that are a part of normal skin healing are one of the undesired manifestations of the surgeries. However, interventions by laparoscopy represent minimal invasive surgery, including minimal scars; cosmesis seems to be an important issue, notably for the young patient population who needs reconstructive surgery for UPJO. 10 Viera et al. reported that scars might have a psychological impact and could affect the patient's quality of life. 11 Therefore, treating and also preventing skin scars has become an important issue. Thus, scar assessments come into question. In this study, we compared skin scars of different-sized trocars in SMARTp and SLp patients. According to the best of our knowledge, this is the first study dealing with this issue in the literature with mid-term follow up.
Up to now, many scales were reported for scar assessments such as Vancouver Scare Scale, matching assessment of scars and photographs, and Manchester scar scale in the literature. 12 The OSAS is the most frequently used scale for scar assessments in published literature. 13 We used OSAS in this series and we evaluated parameters of scars, such as vascularization, pigmentation, thickness, relief, pliability, and surface area. According to our results, at the 24th month of surgery, 3-mm trocar scars were statistically significantly lower OSAS scores. In addition, vascularization sub-variables of OSAS scoring were in favor of 3-mm trocars in SMARTp. Results of our series were parallel to our previous report on SMARTp, which seemed also to have better cosmetic results than MLp. 14 Recently, LESS was introduced and promised better cosmetic results for pyeloplasty, but data are still lacking for cosmetic assessment of LESS, in the literature. 10 We used 3- and 5-mm trocars, in SMARTp, and according to our results, better cosmetic results were obtained in the mid term.
We believe that SMARTp is a plausible surgery for cosmesis. In the light of our study, clinicians should be aware of the scar characteristic that patients value the most. In the race of better cosmesis by minimally invasive surgery, there is a need to perform more studies with large cohorts.
There are some limitations in this series. Numbers of patients were low. On the other hand, we could use the patient “Patient and Observer Scar Assessment Scale (POSAS)” but we did not use the Patient part of POSAS, as it might not be the objective. On the other hand, POSAS was not validated for scars of laparoscopic surgeries.
The SMARTp is a new surgical technique, and patients of this series are from an ongoing SMARTp study of our institute. However, we previously described our technique; there is need to develop new devices for performing optimal cuts for trocars on the skin. The functional outcomes were not the subject of this study.
In summary, scars of trocars heal with time. Statistically significant better scar aesthetics were shown by OSAS scores, in scars of 3- and 5-mm trocars of SMARTp surgeries, in this series. The promising cosmesis can be provided by SMARTp. This is also important for young patients.
Conclusion
The SMARTp is a promising surgical technique in minimally invasive treatment of UPJO. It can provide better cosmesis with 3- and 5-mm trocars in adults.
Footnotes
Disclosure Statement
No competing financial interests exist.