
Abstract
Purpose:
To describe our technique for robot-assisted bladder diverticulectomy (RABD).
Patients and Methods:
Ten patients underwent RABD using an extra- or transvesical approach. Three (30%) patients underwent concomitant procedures: Robot-assisted radical prostatectomy, robot-assisted simple prostatectomy, and transurethral resection of the prostate.
Results:
All RABDs were performed successfully. Median estimated blood loss, operative time, and diverticulectomy time were 75 mL, 210 minutes, and 80 minutes, respectively. Median follow-up time was 18 months. Median International Prostate Symptom Score decreased by 57%, P=0.001.
Conclusions:
RABD is feasible and safe. It can be performed via a trans- or extravesical approach, as a stand-alone, or concomitant procedure.
Introduction
T
BD has been performed using several approaches, such as open, laparoscopic, or robotic.
4
–6
Although robotic surgery has recently gained popularity, limited reports exist with regard to robot-assisted bladder diverticulectomy (RABD) within the literature.
7
We report our surgical technique of extra- and transvesical RABD, and perioperative and short-term outcomes of our initial case series, which to our knowledge is one of the largest series of RABD for acquired bladder diverticulae to date. A video demonstrating this technique accompanies this article. A supplementary video demonstrating this technique is available at
Technique
Patient evaluation
We retrospectively reviewed the data of 10 male patients with acquired bladder diverticulae and refractory lower urinary tract symptoms (LUTS) that failed medical intervention and who underwent RABD between August 2011 and May 2013. The main indications for RABD were incomplete emptying, LUTS, and recurrent urinary tract infections. Patients were evaluated using validated questionnaires, urine and blood tests, cystoscopy, imaging studies (ultrasonography, urethrocystography, and/or CT scan), and urodynamics.
Patient preparation
With the patient under general anesthesia and in the lithotomy position, a cystoscopy is performed and a ureteral stent is placed ipsilateral to the diverticulum. A 16F Foley catheter is inserted. Pneumoperitoneum is established, and five ports are placed transperitoneally and positioned similar to the port configuration for robot-assisted radical prostatectomy (RARP) (Fig. 1).

Five ports are placed transperitoneally using the same configuration as for robotic-assisted radical prostatectomy, with the camera port (CM) placed 3 cm above the umbilicus. The da Vinci Si robot is docked between the patient's legs. LA, left arm; RA, right arm; 4th, fourth arm; AS, assistant port.
Extravesical approach
The bladder is filled with saline and, under direct visualization (zero-degree lens), the peritoneum over the diverticulum is incised (Fig. 2). Using blunt and sharp dissection, the diverticulum is circumferentially dissected to its neck. A cystotomy is made at the diverticulum neck, and the diverticulum is excised and placed in an endocatch bag (Endo Catch™, Covidien, Norwalk, CT). The scope is advanced toward the cystotomy, and the bladder is surveyed to ensure no injuries to the ureteral orifices (UOs). The ureteral catheter is removed, and a watertight running closure of the cystotomy is performed in two layers. A Jackson-Pratt drain is placed, the ports are removed, and the specimen is retrieved.
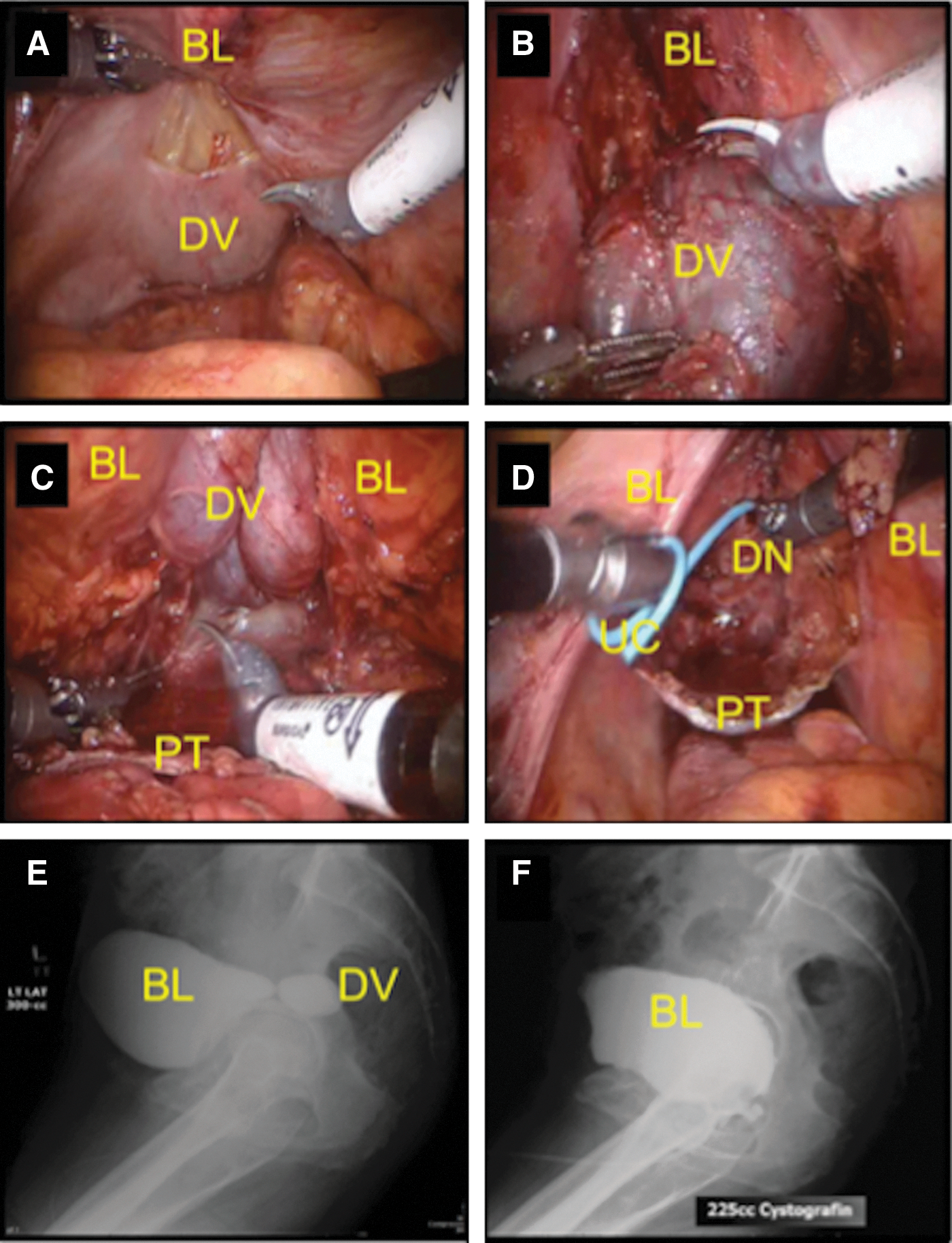
Extravesical robot-assisted bladder diverticulectomy. (
Transvesical approach
This is our preferred approach for diverticulae that are large or close to the UOs. With the bladder filled with saline, a midline cystotomy is performed. The edges of the cystotomy are retracted laterally using stay sutures (Fig. 3). The UOs are identified and the neck of the diverticulum is scored. The tip of the Foley catheter is advanced into the diverticulum, the balloon is inflated, and the diverticulum is filled with saline. From outside the bladder, the diverticulum is dissected to its neck. The bladder mucosa at the diverticulum neck is incised, and the diverticulectomy and bladder closure are performed as described previously.
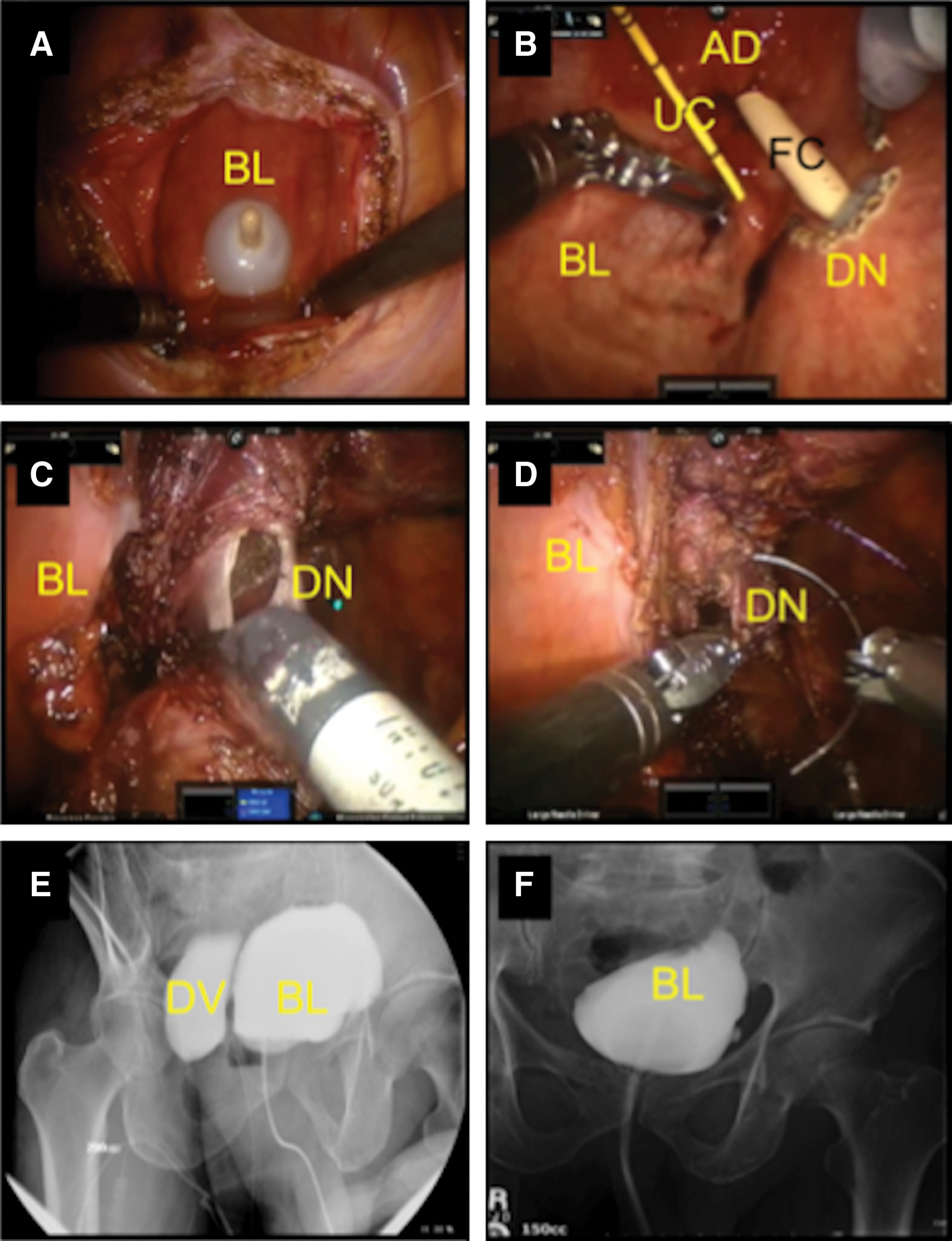
Transvesical robot-assisted bladder (BL) diverticulectomy and concomitant robotic simple prostatectomy. (
Concomitant procedure technique
If a concomitant procedure is planned, a sequential approach is used. For simultaneous RARP, the extravesical RABD is performed first, followed by RARP. For simultaneous robot-assisted simple prostatectomy (RASP), a transvesical approach is used to perform RABD followed by transvesical adenomectomy. As such, the bladder is sutured at the end of the RASP. For a concomitant transurethral resection of the prostate (TURP), the TURP is performed first, followed by RABD.
Postoperative and follow-up
The patient is discharged to home with an indwelling 18F Foley catheter that is removed after cystography on postoperative day (POD) 7 to 8 (Fig. 4).
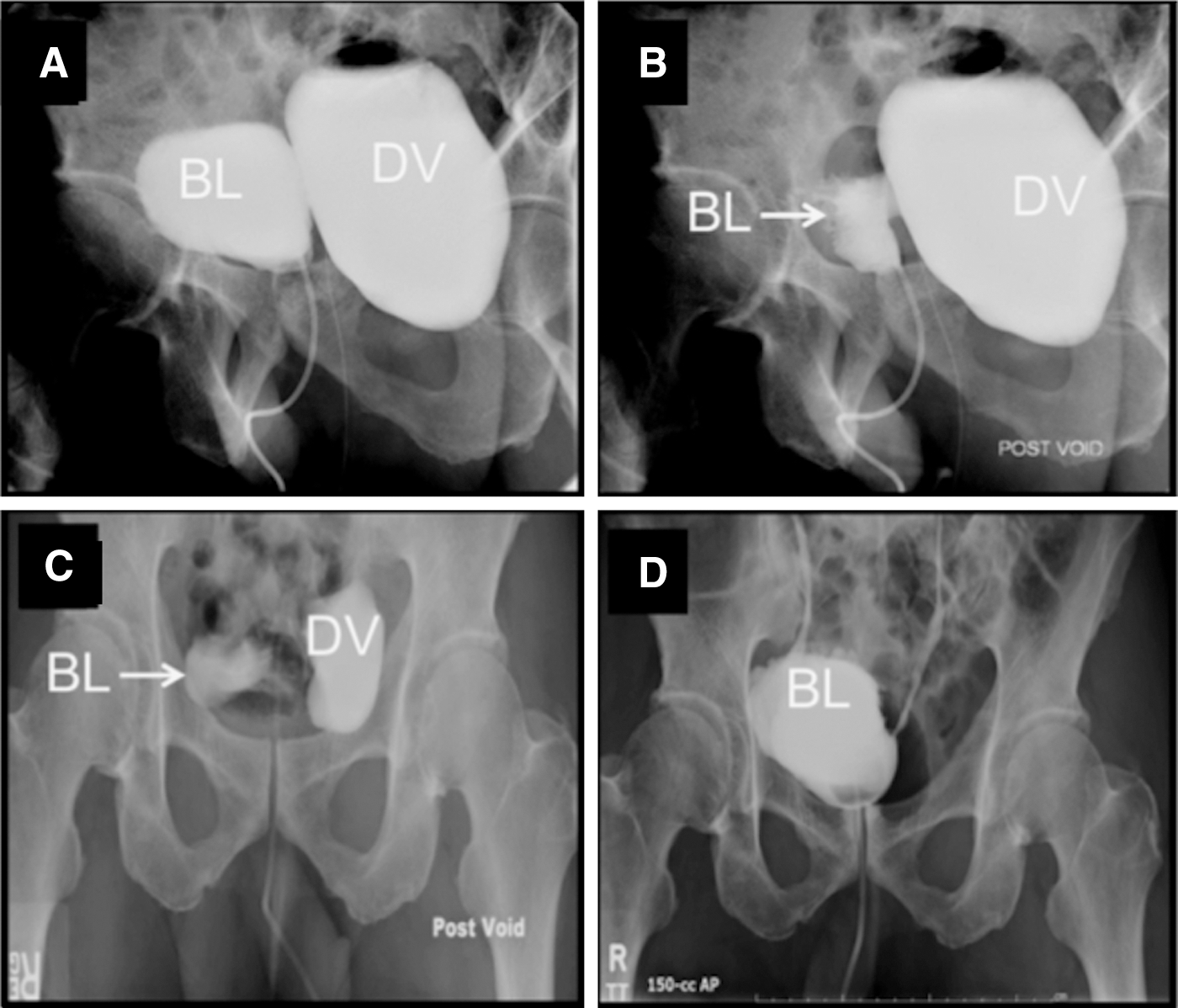
(
Complications were analyzed up to 30 days postoperatively and were graded according to the Clavien-Dindo classification. Follow-up included administering validated questionnaires to assess symptomatic improvement. The two-tailed Student t test was performed to assess statistical significance (P<0.05).
Equipment
• da Vinci Si Robot (Intuitive, Sunnyvale, CA)
• 2-0 Vicryl® (Ethicon, Cincinnati, OH) sutures on a CT-1 needle
• 2-0 V-Loc
• Prograsp™ Forceps (Intuitive, Sunnyvale, CA)
• Hot Shears™ (Monopolar Curved Scissors) (Intuitive, Sunnyvale, CA)
Role in Urologic Practice
Results
All procedures were successfully performed robotically. Three (30%) patients underwent a concomitant procedure: RARP, RASP, and TURP. The patient who underwent RABD and concomitant RARP had, on postoperative cystography, a small leak from the vesicourethral anastomosis but not from the cystotomy. In this case, the Foley catheter was left in place for 16 days with resolution of the leak. Postoperative complications occurred in three (30%) patients, two (20%) of which were low-grade. The patient with a high-grade complication underwent RABD and concomitant RASP and presented with small bowel obstruction from intra-abdominal adhesions on POD 30 that necessitated reoperation. On histologic evaluation, all diverticulae were found to be benign (Fig. 5). Median (range) follow-up was 18 months (7–27); all patients were doing well and the median International Prostate Symptom Score (IPSS) improved 57%, P=0.001 (Table 1).

(
Data pertaining to the largest diverticulum.
One patient with previous radical prostatectomy.
Difference between preoperative and postoperative IPSS was significant, P=0.001.
Difference between preoperative and postoperative quality of life was significant, P=0.002.
Concomitant RARP, the urine leaked from the bladder-urethral anastomosis.
Concomitant RASP. This patient presented with small bowel obstruction from adhesions 30 days after the operation.
BMI=body mass index; ASA=American Society of Anesthesiologists; UTI=urinary tract infection; TURP=transurethral resection of the prostate; RP=radical prostatectomy; IPSS=International Prostate Symptom Score; RARP - robot-assisted radical prostatectomy; RASP=robot-assisted simple prostatectomy.
Discussion
The literature is scarce regarding acquired BD. Approximately 45 cases have been reported to date, of which 30 are for acquired diverticulae and 15 for congenital diverticulae. 2 Open BD has been performed with satisfactory long-term outcomes. 3 More recently, laparoscopic BD has been proposed as an alternative, because of the benefits of minimally invasive surgery (MIS). 4,5 Porpiglia and associates 4,5 reported that laparoscopic BD provided decreased blood loss and postoperative analgesic requirement, and shorter hospitalization compared with open surgery. We report perioperative outcomes similar to other MIS-BDs reported. 2,7 Median estimated blood loss was minimal, median total operative time was 210 minutes, and median diverticulectomy time was 80 minutes. Hospital stay and Foley catheter duration were as expected, and a high-grade complication occurred in one patient with concomitant RASP. On follow-up, median IPSS decreased by 57%.
Altunrende and colleagues 8 report a case series of six adult patients who underwent RABD. We report similar patient indications, perioperative, and postoperative outcomes for RABD. In the present study, we used pre- and postoperative validated questionnaires that demonstrated the efficacy of our surgical treatment.
There are several approaches to perform BD: Extravesical, transvesical, extraperioneal or transperitoneal. While the majority of reported cases use an extravesical approach, we performed the transvesical approach in 60% of our patients. 7 While this choice was based on the surgeon's discretion, some factors favored the transvesical approach: Multiple diverticulae, large diverticulum close to the UOs, and certain concomitant procedures (RASP). We performed RABD extravesically if the diverticulum was small and in a favorable location. From our experience, either approach is feasible, safe, and may provide similar outcomes. We performed RABD transperitoneally because we are familiar with this approach (similar to RARP), and it provides a larger intra-abdominal workspace, allowing better visualization of the anatomy.
Several maneuvers to identify the UOs and the diverticulum are reported. 5,8,9 We were able to identify the diverticulum protruding from the bladder and directly approached it either trans- or extravesically. In cases performed transvesically, the diverticulum was usually large and close to the UO. We advanced the Foley catheter under direct visualization into the diverticulum and filled it to facilitate dissection. We routinely placed a ureteral catheter before RABD if the BD was close to the ureter. The distal part of the ipsilateral ureter was first dissected down to the bladder and looped up. These preventive maneuvers do not add significant time to the procedure but can decrease chances of ureteral injury. In our series, we did not experience injury to the ureter or UOs.
It is important to manage the underlying disease that causes the diverticulum. 1,3 RABD can be performed as a single-stage or stepwise procedure (two separate operations). 4,5,10 We report a total MIS single-stage approach in three patients. One patient underwent RABD with concomitant RARP. Because the diverticulum was located in the posterior midline and close to the dome, we performed RABD before dropping the bladder from the anterior abdominal wall for RARP. One patient had a large prostate (80 g) and a large diverticulum (8.3 cm). We performed RABD tranvesically with subsequent transvesical RASP. This patient was reoperated on POD 30 for adhesive small bowel obstruction. The final patient who underwent a concomitant procedure had a 69 g prostate gland with four diverticulae. To avoid tension on the suture line of the bladder, we performed TURP before the RABD. 4,5 This patient had no perioperative complications, and no leak was noted on postoperative cystography.
Conclusion
RABD is feasible and safe. It can be performed trans- or extravesically and as a stand-alone or concomitant procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.