
Abstract
Objective:
To assess urologists' practice patterns and beliefs about dietary therapy for stone prevention. Dietary therapy is offered to stone formers (SFs) by a subset of urologists. While some may involve a registered dietitian (RD) to provide medical nutrition therapy (MNT), most do not as MNT is Medicare-covered only for diabetes and chronic kidney disease.
Materials and Methods:
An investigator-created survey was distributed to assess Endourological Society members' opinions, confidence, and practices regarding nutrition therapy.
Results:
Respondents (n=217) practice largely in academic, hospital/clinic, and private settings. Most (82%) felt dietary therapy should be provided regardless of the number of stone events. Most (90%) said the urologist should provide dietary recommendations and more than half (52%) do so for ≥75% of patients (10% provide it for <25%). Time spent with SFs for nutrition varied from ≤4 to ≥10 minutes (31% and 23%) with 64% feeling this to be insufficient time. Of urologists providing counseling, 58% assess their patients' diets. Self-confidence in determining dietary contributors to risk factors and in quantifying intake of foods/nutrients varied (range 45%–82%). Most (76%) said they would like another provider to give recommendations; 23% partner with an RD to do so.
Conclusions:
Urologists are interested in dietary stone prevention, despite the fact that the majority have inadequate time to provide it. We identified areas of educational need, specifically, quantifying patients' intake of certain foods/nutrients and identifying whether stone risk factors are diet related. Urologists' skill gaps are precisely the strengths of RDs, and thus, a partnership between RDs and urologists could be beneficial.
Introduction
W
Because nutritional strategies are effective for stone prevention, it is important to determine the current practice patterns, confidence, knowledge levels, and knowledge gaps of clinicians who provide nutrition therapy. Currently, registered dietitians (RDs) are not routinely involved in urology clinics where patients with kidney stones are often seen for management and prevention. A recent survey of RDs revealed that only 8% provide medical nutrition therapy (MNT) for stones in the context of a specialty clinic multidisciplinary team. 6 This contrasts with a survey of urologists, in which 83% to 88% reported providing dietary recommendations to their patients with urolithiasis. 7 The purpose of our study was to determine the practice patterns of endourologists of the Endourological Society with regard to providing nutrition recommendations. In addition, we sought to measure their confidence in assessing patients' diets and providing strategies to manage specific nutrition-related stone risk factors.
Materials and Methods
In October 2013, an electronic Qualtrics survey was devised and distributed to the Endourological Society, an international organization of urologists specializing in minimally invasive endourological techniques, many of which are routinely utilized in the surgical management of kidney stones. As such, these urologists should be more prone to be proactive regarding dietary stone therapy than general urologists. The survey consisted of 11 multipart branching questions regarding beliefs about diet and stones, confidence in providing preventive nutrition recommendations, and the manner in which recommendations are provided. Information was also collected on geographical area of practice, professional setting, years in practice, and gender. Responses were collected over a 1-month period. Closed format questions were utilized to minimize the time needed to complete the survey and maximize survey completion rates. Responses to surveys with missing data were included in the results. Results were tabulated electronically and evaluated.
Results
Respondent characteristics
Respondents (n=217) were mostly male (96%). The response rate was 9.3% based on a reported membership of 2,324 (Endourological Society, personal communication, Jan 2014). Table 1 provides practice information for the respondents. Compared to other recent studies for which members of the Endourological Society were surveyed, 8,9 the reported practice characteristics of our respondents were similar.
Interest and role in dietary prevention
The overall interest in nutrition by urologists for the management of kidney stones was 87%, and most (82%) felt dietary recommendations should be provided to all stone formers (SFs), regardless of number of stone events. The vast majority (88%) reported personally providing dietary recommendations to their patients. Of all respondents, including those who reported not personally providing dietary recommendations to patients, 47% have another staff member to do so. Most cited providers were RDs (23%), nephrologists (14%), and nurses (9%). Of urologists without a staff member to provide dietary recommendations, 76% would prefer one.
Assessing patients' diets
Urologists' opinions varied as to the relative contribution of dietary factors to patients' specific risk factors. For high urine calcium, the majority (54%) thought that diet contributed “only a little,” while 29% thought it contributed “quite a lot” or “all or nearly all.” Respondents reported that diet contributes “quite a lot” or “all or nearly all” to high urine uric acid (69%), high urine oxalate (57%), and low urine citrate (47%). More than half of the respondents (58%) reported personally assessing their patients' diets for nutritional components related to stone risk. Of these, a majority felt confident in determining whether specific stone risk factors were diet related (67%–82%), but confidence in accurately quantifying patients' daily intake of the most common dietary risk factors—sodium, calcium, and oxalate—fell to about 50% or less (Fig. 1).
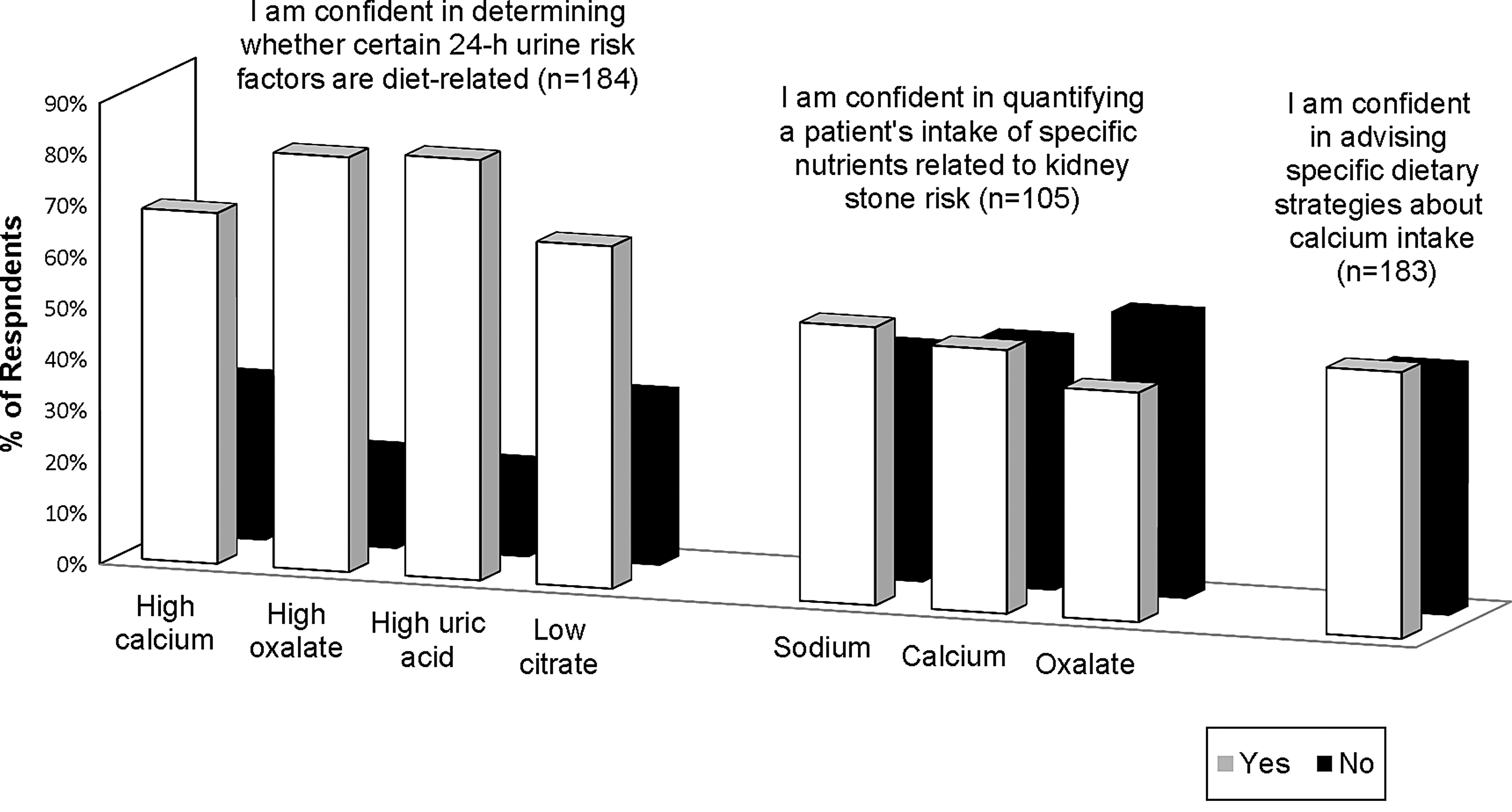
Urologists' confidence in assessing patients' diets for stone risk factors and in providing specific dietary recommendations to prevent recurrence.
Providing specific strategies
When asked about confidence in providing specific strategies to achieve optimal calcium intake, confidence was lower at 52% (Fig. 1). In the scenario of a patient with high urine calcium whose diet was determined to play a role, most respondents reported confidence in providing dietary recommendations to address it (73%). Even more, felt confident to address dietary contributors to high urine oxalate (86%), high urine uric acid (88%), and low urine volume (94%). In patients with a suspected dietary contributor to low urine citrate, 80% of urologists felt confident in advising dietary strategies to raise it. Urologists' practices regarding calcium supplementation for patients with a history of and/or risk factors for calcium oxalate stones varied (Fig. 2).

Urologists' practices regarding recommending calcium supplements to patients with a history of calcium oxalate kidney stones (n=169 responses).
Frequency and time spent on diet recommendations
Of urologists who reported personally providing nutrition recommendations to patients, more than half (52%) said they offer it to ≥75% of their patients; 10% provide it to <25%. Seventy percent were confident that their recommendations were effective in preventing recurrence. Time spent per patient for dietary recommendations varied as follows: ≤4 minutes (31%), 5 to 9 minutes (46%), 10 to 14 minutes (17%), and ≥15 minutes (6%). Only 36% of urologists reported feeling that they have sufficient time to provide nutrition recommendations and 62% would like more time.
Discussion
According to our results, the majority (90%) of the endourologists in the Endourological Society who responded to our survey believe they should provide nutrition recommendations, and the majority does so. Moreover, most believe these recommendations are effective. This is in agreement with a previous study, in which 72% of general urologists and 73% of endourologists thought themselves able to effectively provide dietary recommendations to SFs. 7
While we found that urologists believe that high urine oxalate and uric acid are highly attributable to dietary factors, fewer reported believing that diet is a major contributor to high urine calcium. This likely reflects the well-known prevalence of genetic and nondietary influences on this parameter such as hyperparathyroid activity, excessive calcium resorption from bone, intestinal hyperabsorption of calcium, and impairment in renal tubular reabsorption of calcium. 4 Hypercalciuria does, however, have several nutritional influences, including high sodium intake, 10,11 high dietary acid load, 12,13 suboptimal fiber intake, 14 and/or excessive carbohydrate intake. 15,16
Responses varied widely on the use of calcium supplements (Fig. 2). Increasing the dietary intake of calcium was previously suspected to increase the risk of calcium stones, but research has shown dietary calcium to potentially reduce the risk of stone formation. 17 Furthermore, calcium intake concurrent with oxalate is associated with reduced urinary oxalate excretion secondary to reduced gastrointestinal absorption. 18 Calcium supplementation with meals would be appropriate in patients with calcium malabsorption or in those whose dietary calcium intake was suboptimal. Yet, 27% of urologists reported never recommending calcium supplements to patients with a history of calcium oxalate stones (Fig. 2). On the other hand, 17% would recommend calcium supplements to any patient with high urinary oxalate excretion, without consideration of calcium intake. In some patients with high urine oxalate, calcium intake is already meeting the goal, and thus, other contributing factors should be addressed.
While it may be tempting to restrict dietary oxalate in patients with hyperoxaluria, high oxalate foods like spinach, nuts and seeds, and beets are healthy foods. Dietary oxalate restriction should be reserved for patients whose hyperoxaluria has not responded to other management methods and after genetic and metabolic disorders have been ruled out. These methods include the provision of oxalate binders such as calcium and magnesium with meals, provision of probiotic supplements 19 to replenish oxalate-degrading bacteria in those with a history of frequent antibiotic use, 20 and the discontinuation of supplements such as turmeric 21 and cranberry 22 that have been shown to increase urinary oxalate excretion.
Detailed knowledge by urologists of corrective nutrition strategies for stone risk factors may be insufficient, and this is not an uncommon scenario among healthcare providers. In our survey, about 50% of urologists reported low confidence in quantifying patients' intake of certain stone-related nutritional components (Fig. 1). This is similar to other studies that found perceived knowledge of health-related recommendations outweighed actual knowledge. For example, physicians had inadequate knowledge of therapeutic dietary recommendations to optimize blood lipid profiles. 23 Another study evaluated healthcare professionals' knowledge of lifestyle factors for chronic disease management and found that many overestimated their knowledge as compared to a test of their actual knowledge. 24 Finally, in a study of Canadian gastroenterologists, 89% thought a gastroenterologist should be involved in providing clinical nutrition care, but 20% chose an incorrect indicator for the assessment of general nutritional status. 25 Not surprisingly, all three studies cited the paucity of nutrition training as an obstacle to providing quality nutrition recommendations. 23 –25
An additional finding of our study is that 58% of urologists reported actually assessing their patients' diets. Diet assessment involves asking open-ended questions of a person's typical daily food and beverage intake to quantify food and nutrient intake. The lack of a good diet assessment may mean that improper or irrelevant nutrition recommendations are emphasized, causing the patient to overlook more relevant nutrition information or leave the appointment with misplaced prioritization of recommendations.
While we did not query urologists about the number of patients they see, assuming 30 patients in 7 contact hours, this would leave ∼14 minutes/patient. This is arguably insufficient time to provide the necessary urologic care, assess the diet, and provide nutrition care. In comparison, RDs focus exclusively on providing nutrition therapy—which includes a thorough assessment of diet and supplements and the development of an intervention—in 30- to 60-minute appointments. Among the 53% of urologists who do not have a staff member to provide nutrition information, 76% would like one. As RDs are highly trained in nutrition assessment and in the development and application of individualized MNT, they are ideal partners for urologists wishing to include nutrition in their stone practices. A recent survey of RDs suggested that RDs are underutilized for stone prevention. Only 48% of RD respondents reported being involved in providing MNT to stone patients. Of those, 80% see only one to two stone patients per month. 6 This study strongly suggests that barriers exist to the inclusion of RDs in the care of patients with stones. Barriers may include lack of reimbursement and the allocation of RDs in hospitals and clinics to other services. Despite these barriers, a clinician with specialized training in nutrition recommendations for stone disease, such as an RD, is often the best option for providing stone patients with the appropriate information to decrease the risk of stone recurrence.
Our study has limitations. The low response rate weakens our findings as does the fact that some urologists did not complete the entire survey. There is population bias due to limiting the survey invitation to urologists with valid email addresses and to those belonging to a single urology organization. Given the limited number of specific nutritional questions in our survey, it is difficult to draw strong conclusions as to the breadth of nutrition knowledge among urologists. Further research could delineate this, identify more specific educational needs, and identify specific attributes that trigger urologists to provide or refer a patient for nutrition intervention.
Conclusions
The results of our study suggest that many urologists support and provide dietary recommendations to prevent stones. However, self-reported confidence in providing the most appropriate corrective nutrition strategies is variable, and the practice is confounded by a lack of specific nutrition training and knowledge as well as limited time. One specific way that urologists could improve the nutrition therapy provided to patients is through ensuring that a thorough diet assessment is performed by obtaining a 24-hour diet recall or using a food frequency questionnaire to determine habitual intake. Due to their rigorous and specialized training in nutrition assessment and therapy, RDs could be beneficial partners for urologists in providing nutrition care to SFs.
Footnotes
Disclosure Statement
No competing financial interests exist for any of the authors.