
Abstract
Ileal ureter is a suitable treatment option for patients with long ureteral strictures. Minimally invasive techniques have been shown to be as safe as open technique and superior in terms of postoperative recovery. We report the first case of laparoscopic totally intracorporeal replacement of ureter using whole-mount ileum in a patient with right-sided long ureteral stricture. The operative time was 150 minutes, and there were no complications. We have demonstrated the safety and feasibility of laparoscopic intracorporeal ileal ureter with possible advantage of shorter operative time compared with the robotic-assisted technique reported recently.
Introduction
S
The first case of hybrid laparoscopic ileal ureter replacement was reported in 2000, 3 and the same group has also shown clear benefits of laparoscopic assistance over open surgery in terms of postoperative recovery. 4 Since then, there are various reports of ileal ureter using hybrid laparoendoscopic single site as well as robotic approaches. All these groups harvested the bowel openly through a separate incision, however. To date, there has been only one report of totally intracorporeal ureteral replacement using robot assistance. 5 Standard laparoscopy has not been applied yet.
In our study, we report the first case of laparoscopic totally intracorporeal ileal ureter replacement for a patient with a long ureteral stricture. Our patient is a 73-year-old woman with a primary diagnosis of retroperitoneal fibrosis. The patient presented with right-sided ureteral stricture resulting in right hydronephrosis (Fig. 1). In this article and supplementary video, we illustrate detailed surgical steps of laparoscopic intracorporeal ileal ureter (Supplementary video is available online at
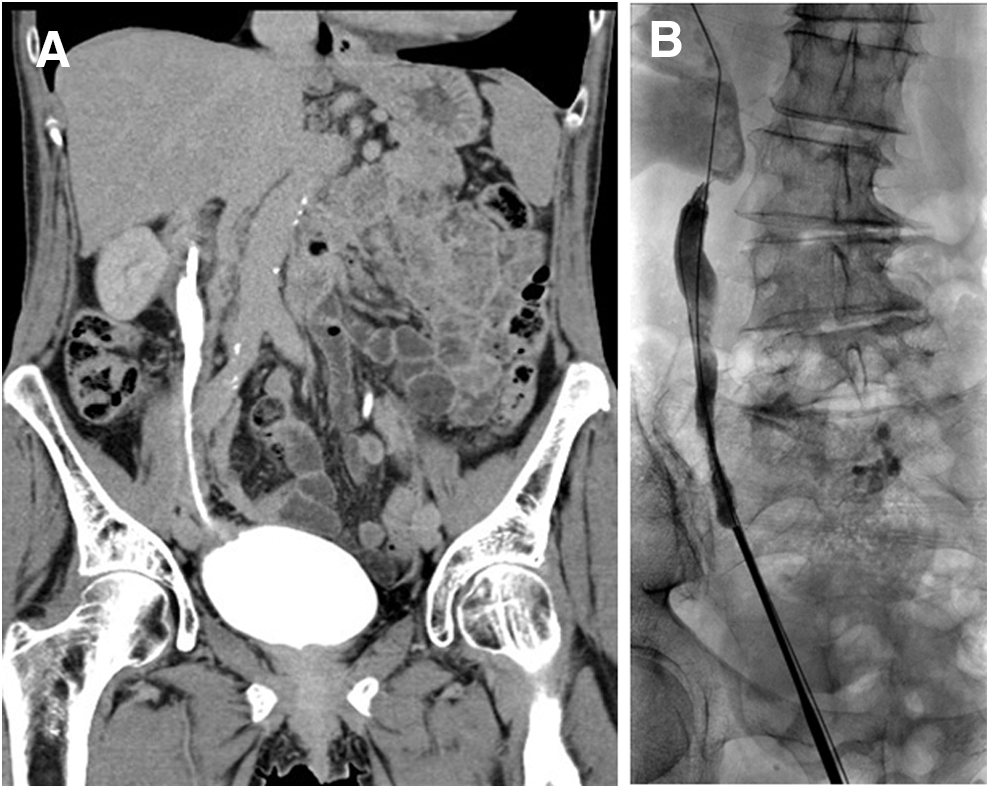
Preoperative CT scan (
Technique
A conventional laparoscopy set and 30-degree telescope are used. The patient is placed in a left lateral position. A transperitoneal approach is used in this case. Ports were positioned as follows: 10-mm port at the level of the umbilicus, two additional 12-mm ports 5 cm above and below the umbilicus, and one 5-mm port 1 cm below the xiphoid for liver retraction. All the ports are placed in the midline. An additional 12-mm port is placed in the right iliac fossa to facilitate the application of an Endo-GIA stapler (Fig. 2).

Port placement: 10-mm port above umbilicus for camera; 12-mm port×2 5-cm above and below the umbilicus; 5-mm port 1 cm below the xiphoid for liver retraction; and additional 12-mm port in right iliac fossa for Endo-GIA stapler.
The ascending colon is medialized to expose the right renal pelvis. A careful dissection of the renal pelvis is performed. In this case, a Double-J stent was inserted preoperatively, and this helps in the identification of the ureter and renal pelvis. After the ureter is identified, the ureter is transected and the Double-J stent is removed. Extensive mobilization of the renal pelvis is then performed, and a stay suture using a straight needle is placed to suspend the renal pelvis.
A loop of terminal ileum 20 cm away from the ileocecal valve is identified and suspended to the right abdominal wall using a straight needle. The proximal end of the terminal ileum is transected using an Endo-GIA stapler. Bipolar cautery is used for hemostasis of the cut mesentery if bleeding occurs. The transected end of ileum is brought up to the renal pelvis and temporarily fixed in that position using polyglactin 3/0 sutures. The distal end of ileum is brought down to the pelvis to ensure adequate length for the distal anastomosis, and it is transected at this point using the Endo-GIA. Care is taken to ensure that it is an isoperistaltic segment.
The bowel continuity is reestablished by performing functional end-to-end anastomosis using an Endo-GIA stapler. The pyeloileal anastomosis is performed using a barbed suture (Stratafix suture, Ethicon). A 9F Double-J stent is inserted before completion of the anastomosis. After completion of the pyeloileal anasotomosis, the bladder is mobilized, and a cystostomy is performed at the dome. The ileovesical anastomosis is performed in a similar fashion using the same suture material. A surgical drain is placed.
Equipment
• Standard laparoscopy set
• 30-degree telescope
• 10-mm port×1, 12-mm port×3, 5-mm port×1
• ndo-GIA staplers with reloads
• Stratafix suture×2
• 9F Double-J stent
Role in Urologic Practice
The operative time was 150 minutes, and blood loss was minimal. The patient progressed to a diet on postoperative (POD) 1 with bowel movement on POD 2. There was no significant change in the preoperative and postoperative glomerular filtration rate. The surgical drain was removed on POD 2, and the catheter was removed on POD 5 after a satisfactory cystogram showed no leak. The patient was discharged well on POD 6. There are no perioperative complications. The postoperative intravenous urography showed no contrast extravasation (Fig. 3). The Double-J stent was removed 6 weeks after surgery.
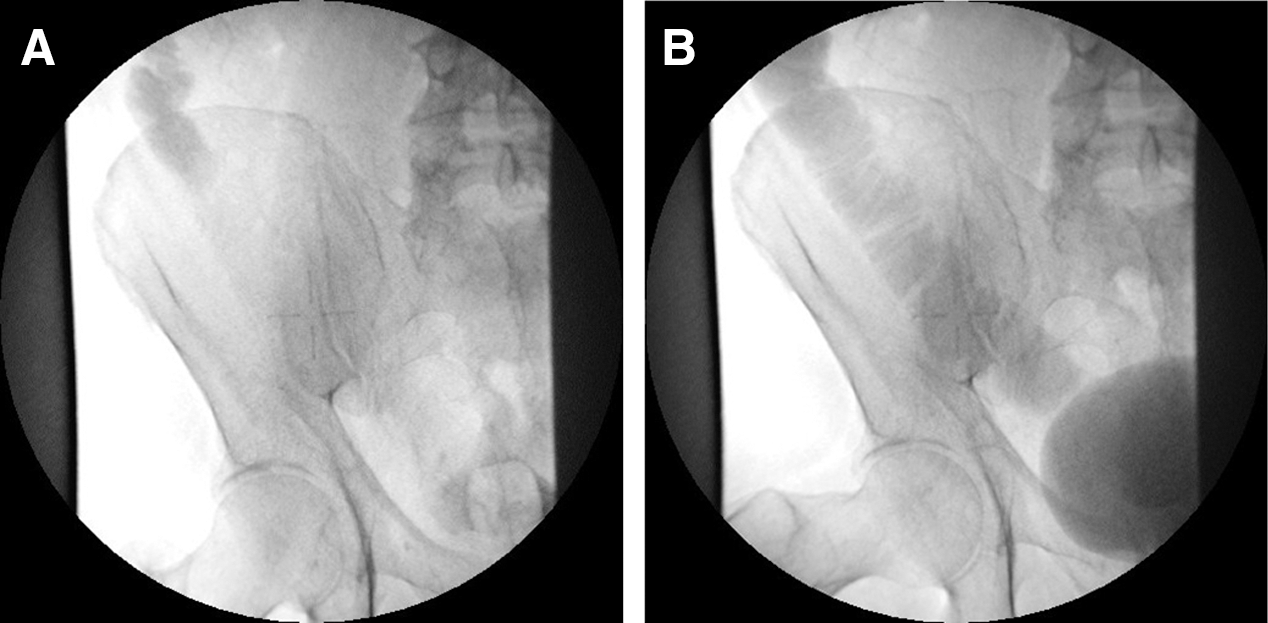
(
A previous study has shown that laparoscopic ileal ureter is superior to open surgery in terms of shorter time to convalescence and shorter hospital stay. 4 A recent study has demonstrated the feasibility of completely intracorporeal ileal ureter using robotic technique. 5 The operative time was 7 hours, however, and this is partly attributed to the docking and undocking of the robot during different parts of surgery, according to the author.
In our study, we think that the laparoscopic approach is clearly advantageous in terms of operative time because the position of the patient can be adjusted whenever necessary without having to undock the robot, thus shortening the operative time. The additional 12-mm port inserted to the right iliac fossa provides a better angle for manipulation of the Endo-GIA to aid in the bowel resection and reconstruction. The pyeloileal and ileovesical anastomosis can be performed efficiently with the aid of barbed suture such as Stratafix or other similar materials. We think all of these factors attributed to the shorter operative time observed in our patient.
Conclusion
Laparoscopic intracorporeal ileal ureter is a safe and feasible procedure and may be a good alternative technique in patients undergoing this surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviation Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.