
Abstract
Background and Purpose:
Flexible nephroscopy is an important technique in the management of staghorn renal calculi to reach peripheral calices. In this study, we present our experience with flexible nephroscopy and fluoroscopy-guided additional access creation for staghorn renal calculi.
Patients and Methods:
We conducted a retrospective analysis of patients with staghorn renal calculi who were treated with multiple percutaneous renal tracts created with the guidance of flexible nephroscopy and fluoroscopy. Additional tracts were performed with combined flexible nephroscopy and fluoroscopy guidance. Flexible nephroscopy was used to help target the calix and ensure the safety of access.
Results:
Additional percutaneous renal access was achieved using combined flexible nephroscopy and fluoroscopy guidance in 26 patients with complete staghorn (n=21) and partial staghorn (n=5) kidney stones. The cumulative stone size was 59.3 mm. The mean procedure times, fluoroscopy times, and hospitalization times were 91.5 minutes, 3.4 minutes, and 2.7 days, respectively. The postoperative hematocrit drop was 4.96±3.8. Upper and lower calices were the most common primary access tracts in 11 and 15 patients, respectively. Stone-free status was achieved in 22 (84.6%) patients with a mean 2.1±0.3 tract number. Postoperative complications were observed in six (23.1%) patients.
Conclusions:
In the requirement of additional access for staghorn renal calculi, use of flexible nephroscopy with fluoroscopy increases the safety of the procedure by confirmation of precise renal access.
Introduction
A
Although stone removal through a single renal tract with flexible instruments and laser lithotripsy is popular, multiple renal accesses may sometimes be needed for a large caliceal stone burden or an inaccessible renal calix. In these situations, multiple-tract PCNL is an indispensible management option for staghorn calculi. Some authors recommend making punctures to the potential calices at the outset of the procedure and inserting guidewires to stabilize the tract before dilating the main tract. 4 On the other hand, making subsequent punctures if necessary is also reasonable, because laser lithotripsy with flexible nephroscopy may remove some of the satellite stones.
The creation of additional tracts can be more technically challenging; the renal collecting system cannot be distended or opacified through the ureteral catheter because of extravasation from the main tract. Moreover, confirmation of precise renal access may be difficult. Flexible nephroscopy is an additional imaging guidance method for this challenging issue. In this study, we present the safety and efficacy of endoscopy-verified additional renal access for staghorn renal calculi.
Patients and Methods
We conducted a retrospective analysis of patients with staghorn renal calculi treated with multiple percutaneous renal tracts created with guidance of combined flexible nephroscopy and fluoroscopy in two referral centers between 2010 and 2013. The procedures were performed by experienced senior urologists (TZ, AT). The patients' demographics (age, sex, body mass index (BMI), stone size, cumulative stone size) and perioperative and postoperative outcomes (operation, fluoroscopy, hospitalization time, hemoglobin drop, success and complication rates) were also analyzed.
All patients were evaluated with routine laboratory tests and radiologic methods, including CT. Patients with positive urine cultures were treated appropriately during the preoperative period.
Operative technique
After the insertion of a 5F or 6F open-ended ureteral catheter, the patient was placed in the prone position. After opacifiying the collecting system through the ureteral catheter, we selected the main puncture site based on the CT and retrograde urography findings. The access was performed using an 18-gauge access needle under the guidance of fluoroscopy. 5 A guidewire was inserted to the collecting system and directed down to the ureter. The renal tract was dilated over the guidewire using Amplatz dilators up to 30F. The Amplatz sheath was inserted into the collecting system over the dilator. The stone was fragmented and removed using endo-lithotripters (pneumatic or ultrasonic) and a 24F rigid nephroscope. The residual stone fragments in the peripheral calices were evaluated with flexible nephroscopy and fluoroscopic imaging. The small peripheral caliceal stones were fragmented using a holmium:yttrium-aluminum-garnet laser fiber. The decision to create additional access tracts was made in the event of a large stone burden and a calix that was inaccessible with a flexible nephroscope.
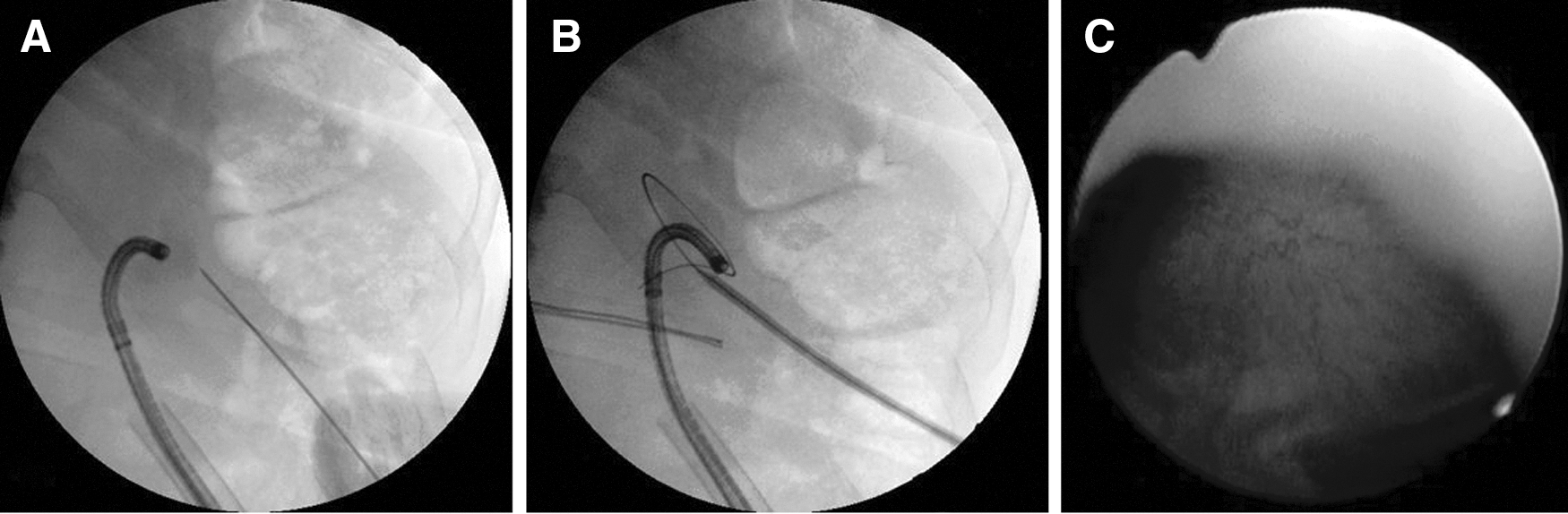
The collecting system could not be opacified or distended because of extravasation through the main renal tract. The flexible nephroscope was inserted into the calix to target the calix and confirm the safety of access. In the case of an infundibulum stone preventing the entrance of the flexible nephroscope into the calix, the stone was fragmented with the holmium laser to allow for the passage of the nephroscope. Then, the flexible nephroscope was inserted into the desired calix. The access needle was targeted to the desired calix with guidance of nephroscopy under fluoroscopy (Figs. 1A, 1B). The entrance of the needle to the collecting system was monitored using the flexible nephroscope (Fig. 1C). A guidewire was inserted to the collecting system. The guidewire could be grasped using a grasper inserted through the flexible nephroscope and withdrawn from the collecting system through the main renal tract (through and through guidewire placement). The tract dilation was primarily performed with endoscopy guidance.
(
All of the phases of tract creation were confirmed by the endoscope. The residual stone burden was fragmented and removed through the additional tract. For the requirement of tertiary access, the tract was created with fluoroscopy or endoscopy guidance. After assessing the stone clearance with fluoroscopy and endoscopy, nephrostomy tubes were put in place over the guidewires.
The patients were evaluated with laboratory tests and plain radiography on the first postoperative day. The ureteral catheter and one of the nephrostomy tubes were removed on day 1. After removing the nephrostomy tubes, the patients were discharged on the second or third postoperative day. Postoperative complications were graded according to the Clavien Classification System. 6 The patients were reevaluated 2 weeks, 1 month, and 3 months after operation. Final stone clearance was based on CT findings.
Results
All of the secondary percutaneous renal accesses were achieved using combined endoscopy and fluoroscopy guidance in 26 patients with complete staghorn (n=21) and partial staghorn (n=5) kidney stones. The cumulative stone size was 59.3 mm, and the patient demographics are listed in Table 1.
The mean procedure time, fluoroscopy time, and hospitalization time were 91.5 minutes, 3.4 minutes, and 2.7 days, respectively. The postoperative hematocrit level (%) drop was 4.96±3.8. The upper and lower calices were the most common primary access tracts in 11 and 15 patients, respectively. Stone-free status was achieved in 22 (84.6%) patients, with a mean 2.1±0.3 tract number for the PCNL session. Tertiary access was needed in three patients. Endoscopic guidance was used for one of the three cases necessitating tertiary tracts. In two cases, flexible nephroscopy failed to guide the access creation because of the steep infundibulopelvic angle (n=1) and large stone-bearing in the infundibulum and calix, which prevented the passage of the nephroscope (n=1). In these cases, access was obtained by targeting peripherally located opaque stones under fluoroscopy. Additional treatment modalities such as shockwave lithotripsy (n=1), ureteroscopy (URS) (n=2), and PCNL (n=1) were used for four (15.3%) patients with residual stone burdens.
Postoperative complications were observed in six (23.1%) patients. The most common complications were fever (n=2, Clavien grade I complication) and urinary tract infection (n=1, Clavien grade II complication), which were managed with medical treatment. Bleeding necessitating blood transfusion (Clavien grade II complication) was observed in one patient. Prolonged urine leakage from the nephrostomy site because of ureteral calculi (Clavien grade IIIb complication) was managed with URS and Double-J stent insertion. In addition, a chest tube was placed in a patient with a hemothorax (Clavien grade IIIa complication). The perioperative measures and postoperative outcomes are summarized in Table 2.
URS=ureteroscopy; DJ=Double-J; PCNL=percutaneous nephrolithotomy; SWL=shockwave lithotripsy.
Discussion
Staghorn renal calculi represent a challenging issue, even for experienced urologists. Surgical management of staghorn calculi is typically associated with increased complication and additional treatment rates, increased duration of hospitalization and operative times, and lower success rates. 1,3,7 American urology guidelines recommend multiple-access PCNL for the management of staghorn calculi 1 ; however, with refinements in technique and accumulation of experience, efforts have been made to accomplish higher success rates and lower complication and morbidity rates. Because of the limitation of reaching peripheral stones using rigid optics and instruments, flexible devices are regarded as essential tools for the management of complex and branched renal calculi. Flexible URS or nephroscopy is efficient in both guidance for tract formation and stone fragmentation.
Ensuring precise renal access to the collecting system is a critical step of the PCNL procedure. 5 Despite the use of imaging methods such as fluoroscopy and ultrasonography for gaining proper percutaneous renal access, this issue may remain challenging, particularly in patients with anatomic abnormalities or without hydronephrosis. In 1995, Grasso and colleagues 8 reported combined simultaneous flexible URS and fluoroscopy-guided percutaneous renal access as an alternative to the failure or difficulty of fluoroscopy-guided access. 8 Khan and coworkers 9 presented the details and advantages of the technique for patients with a nondilated system, anatomic abnormalities, complex renal stones, and a high BMI. 9 After placement of the ureteral access sheath up to the renal pelvis, percutaneous renal access was performed with the patient in the prone position under the simultaneous combined guidance of fluoroscopy and URS. In addition, flexible URS was used to fragment the peripheral satellite stones that could not be reached with a rigid nephroscope.
Similarly, Marguet and colleagues 10 used flexible URS to reduce the number of tracts in patients with complex renal calculi. All patients were treated via single-access PCNL with a stone-free rate of 71.42%. In that study, URS was only used for stone fragmentation and not for access guidance. Prolonged stone fragmentation time with flexible URS and the necessity for access sheath placement can be regarded as limitations of the technique.
A recently published study found that URS-guided access is a safe technique characterized by a significantly decreased fluoroscopy time, bleeding complications, and need for multiple access tracts compared with fluoroscopy-guided access. 11 This technique, however, may fail in cases in which complete staghorn stones filling the entire renal pelvis and extending down to the ureteropelvic junction prevent advancement of the ureteroscope to the calix. In addition, a flexible URS should be readily available and a ureteral access sheath has to be placed in all cases. In the present study, 21 (80.8%) patients had complete staghorn calculi. Therefore, multiple-access PCNL was considered a first-line therapy.
The use of flexible nephroscopy, laser lithotripsy, and baskets increases the success of PCNL and decreases the complication rate by preventing the necessity of using additional tracts. Moreover, postoperative patients' discomfort, need for analgesia, and hospital stay durations significantly decreased with the decrease in tract and nephrostomy tube number. Upper-pole access and second-look nephroscopy are other methods used to achieve higher stone-free rates. 12,13 Despite the advantages of flexible nephroscopy through a single tract, this procedure may not be anatomically feasible in some cases. In addition, fragmentation of large and high-density stones with a laser and the removal of fragments with a basket may take a long time. The other weak point is that the visibility via flexible optics is easily hampered with small amounts of bleeding. In the present study, despite the use of flexible nephroscopy, additional access tracts were needed in all patients.
It is clear that access to a distended calix is simpler than a nondilated calix. Urine reflux from the needle is an important sign and a confirmation of the entrance of the needle shaft into the collecting system. Achieving additional access in a patient who already has an Amplatz sheath inserted into the collecting system is another challenging situation. 14 The collecting system cannot be distended or opacified because of extravasation through the main tract; however, flexible nephroscopy helps in mapping the caliceal system, selection of the access site, and targeting the calix. This advantage becomes particularly more prominent in patients with radiolucent kidney stones that cannot be visualized under fluoroscopy.
The other advantage of endoscopically monitoring the access creation is that it improves the safety of access. The risk of caliceal infundibulum or wall injury related to excessive insertion of the needle, dilator, or Amplatz sheath and related complications such as bleeding, vascular injury, or urinary leakage from collecting system perforation could be avoided with endoscopic visualization. In the present series, we did not observe any case with intraoperative complications such as collecting system perforation or infundibulum tears.
Contrary to its advantages, endoscopic guidance may fail because of the inability to visualize the calix as a result of bleeding or the inability to reach the calix as a result of a steep infundibulopelvic angle or a large stone filling the calix and infundibulum. In the present series, tertiary percutaneous renal access was needed in three cases. In two of these cases, access was achieved with fluoroscopic guidance because of the limitations of endoscopic guidance. The other disadvantage of this technique is the potential risk of damage to the nephroscope. During the passage of the needle and dilatators, extra care should be taken to avoid optic damage. We did not observe any optic damage in our series.
The success and complication rates of the present study are similar to results presented in the literature. 1,3 The studies exploring factors related to hemorrhagic complications showed that tract number is an important factor. 15 –17 In the literature, the blood transfusion rate is reported to be between 0% and 28.4%. 2,15 –18 Although bleeding may occur during different phases of the PCNL, proper access creation plays a key role in the prevention of this worrisome complication. 5 In the present study, the mean hematocrit drop was 4.96±3.8. Only one (3.86%) patient needed blood transfusion in our series. We believe that this technique decreases complications by enabling precise access creation.
The limitations of the present study are the lack of a comparison group and its retrospective nature. Prospective and randomized studies are needed to evaluate other potential advantages of the technique, such as a decrease in fluoroscopic imaging, access creation time, and blood loss. Despite the limitations, to the best of our knowledge, this study is the first to present the feasibility of flexible nephroscopy-guided renal access for renal staghorn stones. We believe that the technique described in this study will contribute to the literature about the treatment of patients with staghorn calculi.
Conclusions
Multiple renal access tracts may be needed for complete stone removal in staghorn renal calculi. It is clear that using flexible optics and a rigid nephroscope improves the outcomes of the procedure. In the event of additional access, using flexible nephroscopy with fluoroscopy increases the safety of the procedure by achieving precise renal access.
Footnotes
Disclosure Statement
No competing financial interests exist.