
Abstract
Purpose:
To conduct a comparative evaluation of ultrasonic, pneumatic, and dual ultrasonic (DUS) lithotripsy to predict the safety of probes on urinary tract tissue.
Materials and Methods:
The Swiss Lithoclast Ultra (ultrasonic-only [US] and ultrasonic–pneumatic combination [US+P]) and the Gyrus ACMI Cyberwand (DUS) were evaluated. Fresh porcine ureter, bladder, and renal pelvis tissues were used with a hands-free setup to vertically apply 0, 400, or 700 g of force with each probe for a duration of 3 seconds, 5 seconds, or 3 minutes (or until perforation occurred). Data collection included whether perforation occurred and time to perforation. Histological analysis of nonperforated samples was used to compare the anatomical depth to which damage occurred.
Results:
The total percentage of trials resulting in perforation for all tissue types, contact durations, and forces was found to be 8.5% (10/117) for US, 13.7% (16/117) for US+P, and 26.4% (31/117) for DUS. No perforations occurred with light contact (0 g) of probe force, regardless of tissue type, lithotripsy mode, or contact duration. Overall, the renal pelvis was most resistant to perforation (p=0.0004), while no difference was found between the bladder and ureter tissue (p=0.32). Force beyond 400 g and contact greater than 5 seconds increased risk for damage.
Conclusions:
Mode of lithotripsy, tissue type, probe force, and probe-tissue contact duration all significantly impacted the extent of damage and likelihood for perforation to occur. All devices and tissue types provided a reasonable margin of safety for probe-tissue contact times of 3 and 5 seconds with no more than 400 g of force.
Introduction
P
Numerous in-vitro/ex-vivo 1 –7 as well as clinical 5,7 –11 studies have evaluated the fragmentation efficiency of these modalities with varying results; however, a limited number of studies have evaluated the extent to which these devices cause tissue damage. Two studies have previously evaluated damage to ureteral and bladder porcine tissues as a result of electrohydraulic, ultrasonic, and laser lithotripsy; however, the live animal models did not take into account the extent to which varying forces impacted the extent of damage. 12,13 To our knowledge, our study is the first to offer a comparative histological tissue damage assessment of recently developed lithotripsy modalities, using a hands-free testing apparatus under controlled probe force.
Methods
We evaluated the Swiss Lithoclast Master (ultrasonic-only [US] and ultrasonic–pneumatic combination [US+P]) and the Gyrus ACMI CyberWand (dual ultrasonic probe [DUS]). A single hollow probe (FR-106, 3.8×330 mm) was used for the US-only mode, and a pneumatic probe (EL-276, 1.0×497 mm) was inserted through the hollow probe for the pneumatic component of the device, protruding approximately 1 mm beyond the hollow probe, and both were simultaneously activated for the US+P mode. Settings were adjusted to reflect optimal clinical settings, with 100% duty, vacuum pressure of 3.5 bar, and a pneumatic frequency of 6 Hz. Two hollow probes (2.77 mm inner and 3.75 mm outer probe) were utilized for the DUS mode, with the inner probe extending approximately 1 mm beyond the tip of the outer probe.
Each mode of lithotripsy was evaluated with three types of porcine urinary tract tissues (ureter, bladder, and renal pelvis), three forces (0, 400, and 700 g), and three durations of probe-tissue contact (3, 5, and 180 seconds). Treatment durations of 3 and 5 seconds were selected to simulate the contact durations typically used in a clinical setting before the probe is repositioned and reflect the typical time that inadvertent tissue contact may occur. A treatment duration of 180 seconds was selected to determine the time required for perforation to occur while minimizing the impact of probe temperature, as probes tend to heat up with continued use. Forces of 400 and 700 g were based on evaluations conducted with a urology resident, research fellow, and two experienced endourologists at our institution. Each was given a lithotrite probe and asked to conduct 10 repetitions of the typical probe force used to treat soft and hard stones, which ranged from 96.3 g to 418 g for soft stones and from 395 g to 953 g for hard stones. We selected the upper limit for soft stones and the approximate average used for hard stones to allow for a relatively even spread within the range of applied pressures. Zero g of force was used to determine the combined impact of suction and each lithotrite energy. A total of five repetitions were conducted for all ureter and bladder trials, and three repetitions were conducted with renal pelvis tissues, for a total of 351 trials.
The order in which testing was completed was fully randomized between the combinations of all four independent variables, and a hands-free setup was used to ensure consistency between trials. Figure 1 demonstrates the setup used for testing. A vertical sliding mechanism was used to attach a lithotripter (Fig. 1, part B) to the testing stand with the probe facing downward into the container in which the tissues were held (Fig. 1, Part A). To precisely control the vertical force of the lithotrite, the sliding mechanism was connected to a pulley system that allowed for counterweights (Fig. 1, part D) to be easily attached and removed. Vertical force was confirmed with the use of a digital scale. Constant irrigation was maintained with normal saline during testing, with the use of a closed flow system and an electrical pump (Fig. 1, Part C, Fluid-o-Tech Rotoflow Model 8XAGD) and motor (A.O. Smith Model 316P497).

Hands-free testing setup.
Porcine urinary tract tissues were obtained from 11 hogs (both male and female) ranging from 154±5 lbs to 250±5 lbs. Tissues were obtained at the time of slaughter and testing was conducted within 24 hours of removal. Renal pelvis, ureter, and bladder tissues were sectioned, exposing the urothelium for direct contact with the probes. Figure 2 shows the setup used for securing tissue specimens. Samples were secured between two washers with a 0.5 in diameter hole through the center of the discs, allowing the lithotrite to directly contact the tissue and pass through if perforation occurred. The metal washers had sandpaper glued to the side in contact with the tissue to provide grip. After placing each specimen over the center hole of the bottom washer, the top washer was placed directly over it and secured in place by two hand-tightened C-clamp screws. Tension in the plane of the washers was not applied to any tissue specimens; however, the compressive force provided by the C-clamp screws limited horizontal mobility of the tissue specimen and maintained tension across the 0.5 in holes of the washers as vertical pressure was applied during testing. The entire system was placed on top of a roll of tape to allow additional room for the tissue to stretch and the probe to pass through if perforation occurred. Tissue samples were suspended in normal (0.9% NaCl) saline before testing and fixed in a 10% formalin solution directly after completion of each test for histological evaluation.

Setup used for securing tissue specimens.
Data gathered on each trial included whether or not perforation occurred, and if perforation occurred, the amount of time before perforation. A board certified pathologist, blinded to the test conditions of all samples, conducted a histological examination of nonperforated samples to determine the extent of damage. Each sample was sectioned and a hematoxylin and eosin stain was used to determine the anatomical level and severity of damage.
Statistical analysis on the initial data gathered (whether perforation occurred and time to perforation) involved logistic regression to determine the likelihood of perforation based on modality, tissue type, force, and contact time. Linear regression was conducted to determine differences in gross perforation time based on lithotrite modality, tissue type, and force. Ordered logistic regression was used to compare odds of resulting in deeper anatomical damage between lithotrite modalities, tissue types, forces, and contact time. Damage was ordered into six levels increasing in anatomical depth from the lamina propria (LP) to the superficial muscularis propria (MP), MP, deep MP, and finally rupturing into fat or complete perforation. The severity of damage at the deepest anatomical level, at which damage occurred, was categorized as mild, moderate, or severe, depending on the extent of fragmentation and blistering. Figure 3 provides examples of the qualitative damage scale used for grading samples with damage to the LP and MP levels.
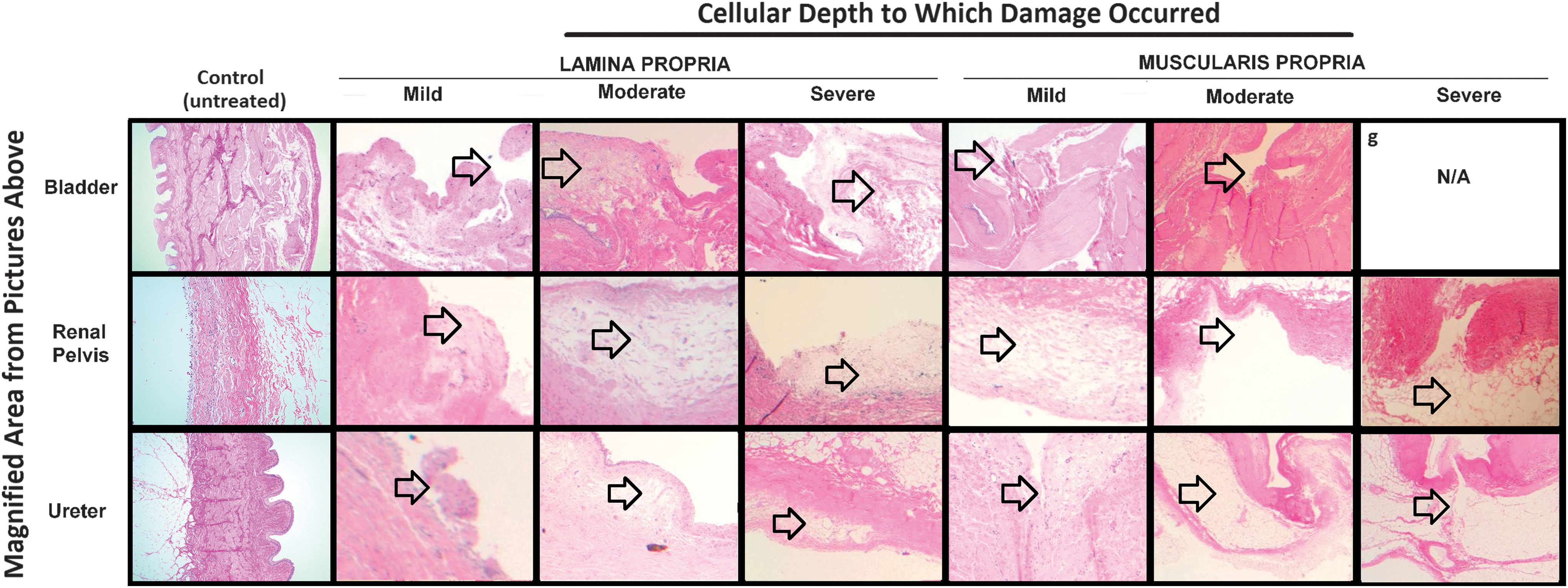
Histological examples of the qualitative damage scale used for grading samples with mild, moderate, and severe damage to the lamina propria (LP) and muscularis propria (MP) levels.
Results
Gross perforation
The total percentage of trials resulting in perforation for all tissue types, contact durations, and forces was found to be 8.5% (10/117) for US, 13.7% (16/117) for US+P, and 26.4% (31/117) for DUS. Logistic regression revealed that the DUS mode had a significantly greater chance of perforation than US+P (p=0.0010) and US (p<0.0001). US had a lesser chance of perforation than US+P, however, the difference did not reach statistical significance (p=0.064).
With regard to tissue type, perforation occurred for approximately 4.94% (4/81) of renal pelvis trials, 20.51% (24/117) of bladder trials, and 24.78% (29/117) of ureter trials. Statistical analysis revealed that the renal pelvis had a significantly lesser chance of perforation when compared with ureter (p<0.0001) and bladder (p=0.0004) tissue. Bladder and ureter tissues were not found to significantly differ with regard to likelihood of perforation (p=0.323). No perforations occurred when 0 g (light contact) of probe force was applied, regardless of tissue type, lithotripsy mode, or contact duration. When force was increased from 400 g to 700 g, the likelihood of perforation significantly increased (p<0.0001). Increasing the contact duration from 3 to 5 seconds was not found to significantly increase the likelihood of perforation (p=0.31), however, a contact duration of 180 seconds was found to dramatically increase the chance of perforation. Results comparing likelihood of perforation are shown in Table 1.
Odds ratios, 95% confidence limits, and p value results from logistic regression comparing chance of perforation between lithotripsy mode, tissue type, force, and contact duration. Statistically significant values are highlighted in bold.
Although no significant difference in the likelihood of perforation was found between US and US+P, our analysis revealed that if perforation does occur, it is more likely to occur in less time when using US+P compared with US (p<0.001). For samples where perforation occurred, the average time it took for perforation to occur for US, US+P, and DUS modes was found to be 117.5±43.9, 34.3±56.0, and 25.8±33.7 seconds, respectively. DUS and US+P did not differ in perforation time (p=0.24), however, DUS was found to perforate in significantly lesser time than US (p<0.0001). Perforation time was not found to differ between ureter and bladder (p=0.33), ureter and renal pelvis (p=0.50), or bladder and renal pelvis (p=0.86). Similarly, increasing force from 400 g to 700 g did not significantly decrease time until perforation (p=0.078). Results comparing perforation times are displayed in Table 2.
Linear regression results on time until perforation between all modes and tissue types and between 400 g and 700 g of probe force (no perforations for 0 g of force). Negative values suggest the first mode/tissue/pressure is likely to perforate quicker than the second. Our model suggests that when perforation occurred, DUS mode perforated samples approximately 97 seconds sooner than US mode, which is considered statistically significant. While our model also predicts 400 g of force resulted in perforation 24.5 seconds after samples on which 700 g of force are applied, the variability in perforation time between samples is too large to conclude whether this difference is significant. Statistically significant values are highlighted in bold.
Histological comparisons
Statistical analysis of histological examinations revealed significant differences in the extent of damage that occurred under the various conditions. No significant difference was found between DUS and US+P modes (p=0.99), however, both were found on average to have significantly greater odds of resulting in deeper anatomical damage than US (p<0.0001). On average, the US mode had the highest probability (44%) of resulting in damage to the LP level (vs. 25% and 16% for DUS and US+P, respectively), while the US+P had the highest probability of resulting in damage to the MP level (48% vs. 28% and 20% for DUS and US, respectively), and the DUS mode had the highest probability of the deepest level of damage, rupturing into fat layers or resulting in complete perforation (23% vs. 4.0% and 1.0% for US+P and US, respectively). Figure 4 demonstrates the complete distribution of damage levels and severity of damage for all devices, tissues, forces, and contact times.

The distribution of damage levels and severity of damage for all modes of lithotripsy, tissues, forces, and contact times. Results are pooled, resulting in a total of 135 ureter and 135 bladder trials (5 trials of all combinations of 3 modes, 3 forces, and 3 durations) and 81 trials on renal pelvis (3 trials of all combinations of 3 modes, 3 forces, and 3 durations). Cellular depth of damage increases from left to right, and severity of fragmentation increases from light to dark. US mode most commonly resulted in damage to only the LP (43% of all trials, approximately half of which was only mild fragmentation or urothelial disruption) and had the highest incidence of resulting in no damage at all (13% of all trials). US+P mode most commonly resulted in damage beyond the LP and through to the MP (46% of all trials, approximately half of which involved moderate fragmentation). DUS mode had similar incidence of damage to LP (26%), beyond the LP and down to the MP (28%), and through both the LP and MP and perforation into fat tissues (23%).
When using histological analyses to compare average damage levels between tissue types, renal pelvis had significantly lower odds of deeper anatomical damage than the bladder (p=0.0035) and ureter (p=0.0079) tissues. No significant difference was found for the average depth level of damage between ureter and bladder tissue (p=0.76), however, the bladder tissue demonstrated a higher distribution of samples with damage to the deep MP level, while ureter tissue was slightly more likely to rupture into fat layers. The most notable difference in the distribution of damage depths among tissue types was with the renal pelvis, which had the highest probability of moderate damage to the level of the MP (76% vs. 36% and 2.0% for ureter and bladder, respectively).
Varying probe force significantly impacted the odds of resulting in deeper anatomical damage, with 0 g of force resulting in significantly lesser odds of deeper anatomical damage than 400 (p<0.0001) and 700 g (p<0.0001). A force of 700 g was not found to significantly increase the odds of deeper anatomical damage than 400 g (p=0.11). A force of 700 g was the only force for which some level of damage was guaranteed, while 0 g was the only force for which the probability of damage down to the level of the deep MP was virtually 0.
A probe contact time of 180 seconds significantly increased the odds of deeper anatomical damage when compared with 3 (p<0.0001) and 5 seconds (p<0.0001) and was noted to have the highest probability of rupturing into fat (23% vs. 3% and 1% for 5 and 3 seconds, respectively). Although increasing the contact time from 3 to 5 seconds did not significantly impact the odds of deeper anatomical damage (p=0.091), the probability of no damage or damage to the superficial MP decreased, while odds of damaging deep MP and rupturing into fat slightly increased. See Table 3 for a statistical summary of the histological analyses.
Results from ordered logistic regression to predict odds of resulting in deeper anatomical damage based on histological damage ratings. Statistically significant values are highlighted in bold.
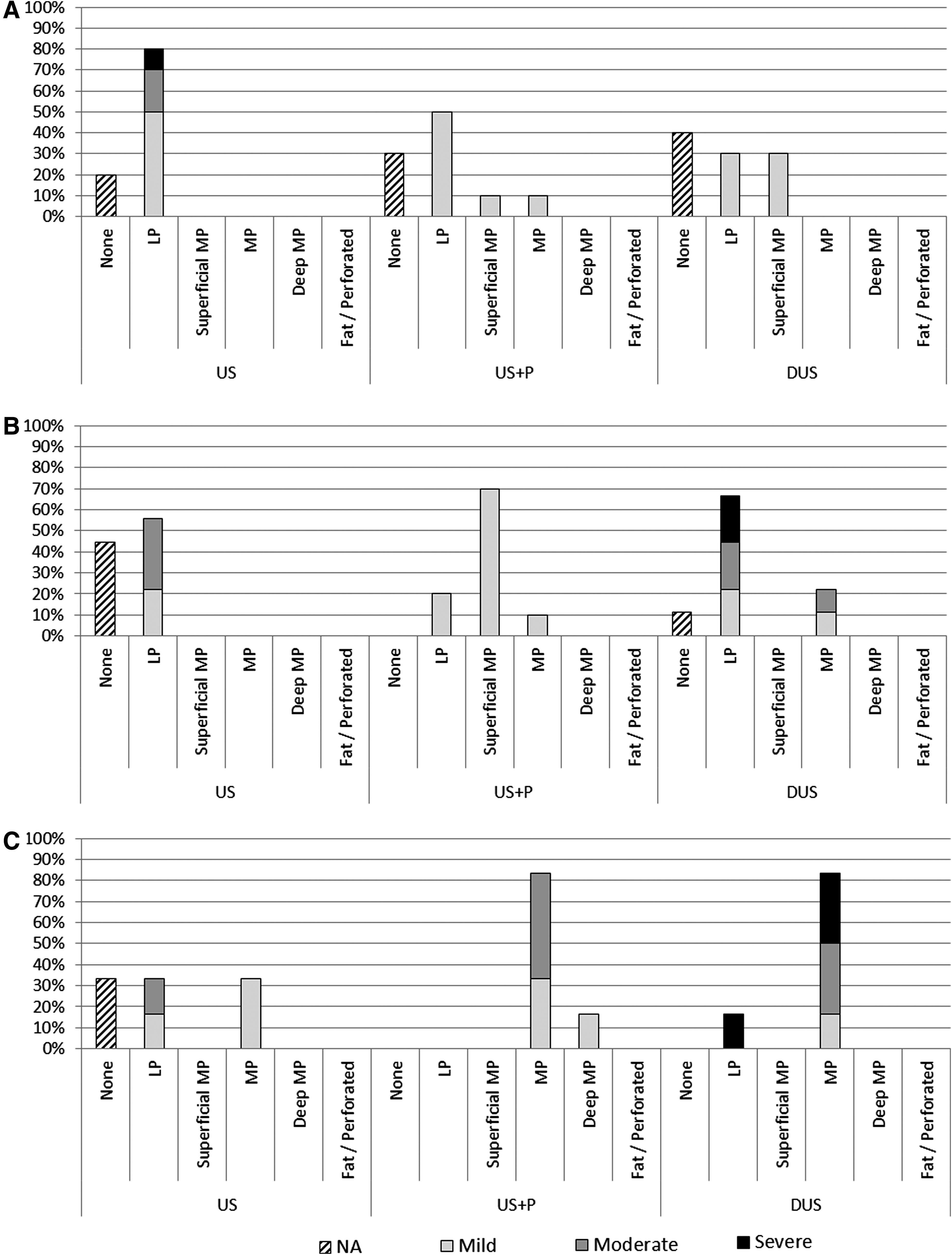
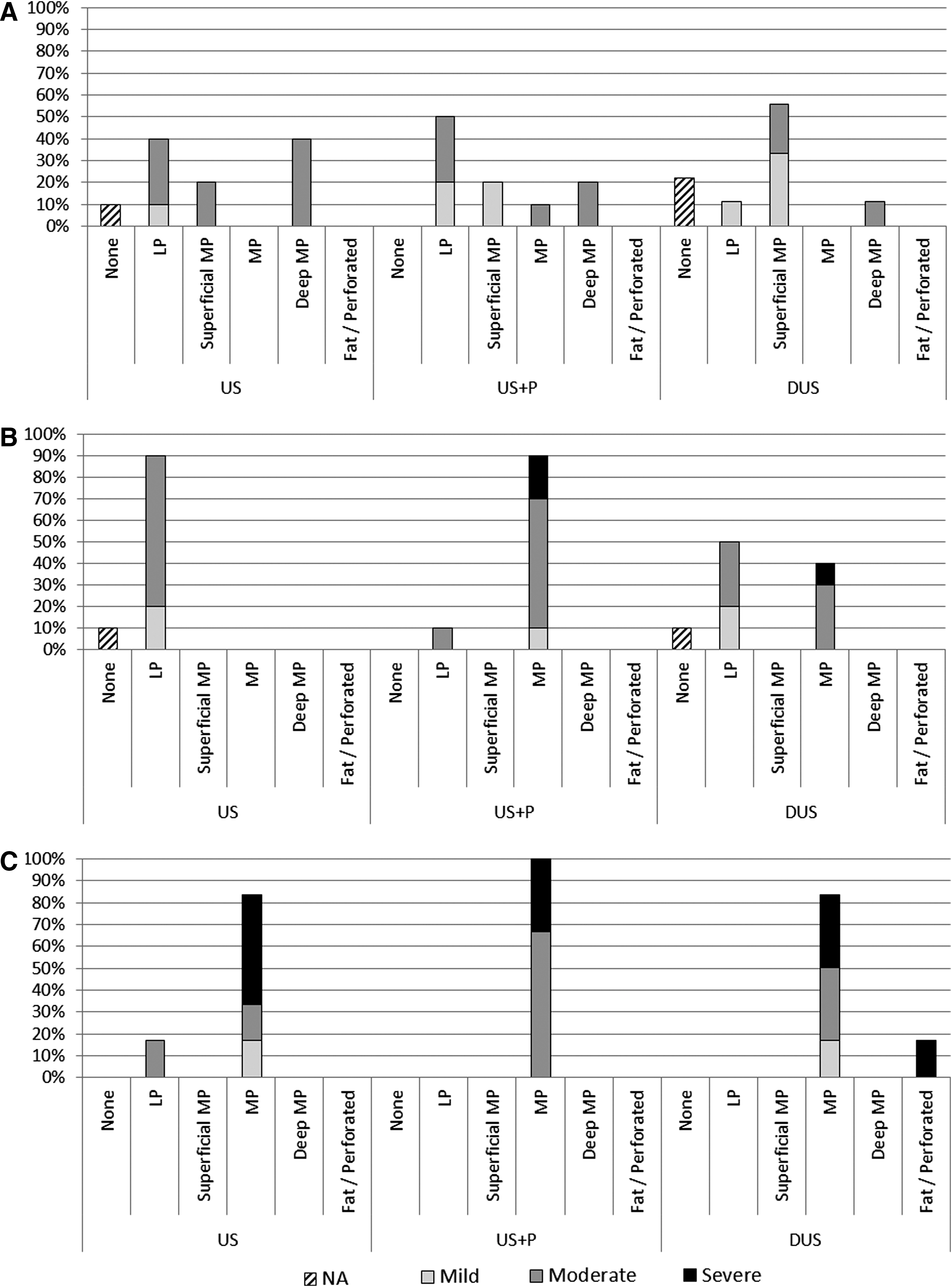
Figure 5 demonstrates the histological damage distribution among the lithotrite modes for bladder (Fig. 5A), ureter (Fig. 5B), renal pelvis (Fig. 5C) and contact durations of 3 and 5 seconds, with 0 g of force. Under such conditions, damage beyond the MP level was rare, only occurring in approximately 16% of US+P trials for the renal pelvis. When the applied force was increased to 400 g under the same conditions (Fig. 6A-bladder, Fig. 6B-ureter, Fig. 6C-renal pelvis), all modes demonstrated a slight shift in damage toward deeper anatomical levels with increasing severity. The most notable difference in damage when increasing force from 0 g to 400 g was found with bladder tissue, which had a significantly greater risk for damage to the deep MP level, when compared with renal pelvis and ureter tissues (p<0.001).
The histological damage distribution among lithotrite modes for bladder
The histological damage distribution among lithotrite modes for bladder
Discussion
Ultrasonic–pneumatic and DUS lithotriptors are known to have an improved ability to fragment stones compared to prior pneumatic technologies, and their use has now become common practice with percutaneous stone extraction. Some studies have shown the combined ultrasonic–pneumatic lithotrite to be the most efficient with regard to stone fragmentation, however, another in vitro study demonstrated the Cyberwand to reduce this time by almost half. 7 With any medical device, the balance between efficacy and safety must be evaluated—to date there has been limited information regarding the relative risk for damage to surrounding tissues with pneumatic and ultrasonic lithotripsy. Santa Cruz et al. used an ex vivo model to determine the relative safety of holmium:YAG lasers, coumarin pulsed-dye lasers, electrohydraulic, and pneumatic lithotripsy with regard to ureteral tissue damage; however, the impact on bladder and renal pelvis tissue was not evaluated. They determined that acute ureteral perforation while utilizing pneumatic lithotripsy was not feasible under their testing conditions. 14 Two other studies previously evaluating damage to ureteral and bladder porcine tissues were conducted before the introduction of ultrasonic–pneumatic and DUS modalities and did not include testing on renal pelvis tissue, which would be at most risk during percutaneous stone removal. 12,13 Animal tests from both studies revealed significant acute bladder and ureter tissue damage, demonstrated by visible mucosal lesions, edema, hemorrhage, and abrasions of the urothelial wall for contact durations ranging from 3 to 7 seconds. The risk of perforation during percutaneous nephrolithotomy in a large multinational prospective registry was 3.4%, however, to our knowledge, there is no clinical trial series comparing the risk of perforation with different lithotrites. 15 We present our findings in the hope of providing a better understanding of the extent of tissue damage associated with common lithotripsy modalities, operating techniques that may help to limit damage, and the margin of safety associated with the various urinary tract tissues.
Our findings suggest that when utilizing contact durations up to 5 seconds and a force of no more than 400 g, all modes of lithotripsy provide a reasonable margin of safety with all tissue types evaluated. Although the DUS mode was found to be the most likely to result in perforation, gross perforation did not occur when applying 400g of force for durations of 3 or 5 seconds. When the contact duration was extended beyond 5 seconds or force was increased to 700 g, the risk of perforation with DUS dramatically increased, especially with bladder and ureter tissues. Renal pelvis tissue demonstrated a significantly greater resistance to perforation compared with bladder and ureter tissue, while the latter two resulted in a similar risk of perforation. Overall, the likelihood of gross perforation between lithotrite modalities, contact times, forces, and tissues was a good predictor of the average anatomical depth, to which damage was observed.
The histological analyses of nonperforated samples revealed the thick MP layer of the renal pelvis provided a reasonable buffer for preventing damage to deeper tissue layers. Increasing the contact duration from 3 to 5 seconds while utilizing 400 g of force did not demonstrate any increase in the likelihood of perforation among the different modes of lithotripsy for different tissue types; however, the average anatomical depth that sustained damage was more frequently noted to occur to the deep MP level, suggesting that even 2 additional seconds of contact time has the potential to cause additional damage.
Trials conducted for 3 and 5 seconds with 0 or 400 g of force (Figs. 4 and 5) were analyzed to determine the risks most likely to reflect those found in a clinical setting. Although the overall initial results suggested a greater frequency of gross perforations with ureter tissue compared with bladder (27/117 vs. 24/117), the histological analyses inclusive of more clinically relevant parameters for contact time and force revealed that the bladder tissue was most sensitive to an increase in force from 0 g to 400 g. Such results for the bladder are demonstrated by the greater shift in damage beyond the MP to the deep MP levels, accompanied by increased severity ratings, suggesting that more urothelial disruption occurred. While the exact clinical implications of varying damage to the LP, MP, and fat tissue layers are unclear, damage to the deep MP and fat layers may be more likely to be associated with urinary extravasation and subsequent stricture formation; this may be of particular concern for ureteroscopic applications of this technology.
Based on this data, we recommend limiting the extent to which pressure is applied to the probe when utilizing all modes of lithotripsy, in particular, for applications in the bladder. In addition, operators should take into account the variability in weight between devices when applying downward pressure, as the slight difference in weight of a device may further increase the likelihood for damage to occur. Applying pressure perpendicular to the tissue may also increase the impact of suction on tissue damage. When perpendicular to the tissue, the hollow probe becomes flush against the tissue and suction can slightly draw the tissue into the probe, limiting the extent to which fluid can flow into the probe. The impact of such suction on the tissue was grossly visible on the majority of samples and may increase risk of damage when compared to pneumatic-only modalities, where suction is not used. However, the ability to aspirate fragments remains one of the significant advantages of the lithotrite modes evaluated, and applying force at an angle may limit the extent to which tissue suction occurs.
The authors believe that differences in perforation rates among lithotrites that were evaluated may be due to the varying degree to which probe force may impact the transfer of energy to tissues. Increasing probe force by similar increments for different modes may increase the efficiency of energy transfer to different extents. It is possible that the efficiency of probe-tissue energy transfer for DUS lithotrites is more sensitive to increased contact force, resulting in greater urothelial fragmentation that may ultimately lead to an overall increased risk of gross perforation. Probe configuration and orientation are also likely to impact the risk of tissue damage. While both DUS and US+P modes have an inner probe that protrudes 1 mm beyond the outer probe, the smaller pneumatic probe of US+P may be adjusted to extend greater than 1 mm beyond the tip of the outer hollow US probe, distributing the probe force over the smaller probe rather than the full circumference of the outer hollow probe, thereby potentially increasing pressure on the tissue and risk of perforation.
The use of porcine urinary tract tissues limits the extent to which the risks of exact force values and contact durations used translate to damage in the clinical setting. Human urinary tract tissues have been reported to require lower perforation forces than those found in porcine models, suggesting our results are likely to overestimate the margin of safety associated with these devices. 16 This study is also limited in that, all testing was conducted at room temperature, possibly impacting the elasticity of the various tissues to different extents to what is typical for in vivo conditions. In vivo, different grades of filling may impact tissue thickness and tension, also limiting the extent to which our results translate clinically as our setup did not apply horizontal tension to tissue specimens. Our setup also assumed minimal mobility of tissues, where an in vivo setting may provide greater mobility and compliance that may serve to reduce perforation risk. The primary limitation of our histological damage analysis lies in the subjective thresholds used to determine the severity and damage for each specimen, for which the clinical relevance of the sequential damage ratings is unclear.
Conclusion
Mode of lithotripsy, tissue type, probe force, and probe-tissue contact duration all significantly impacted the extent of damage and likelihood for perforation to occur. The DUS mode was most likely to result in perforation when in contact with tissue for greater than 5 seconds with probe force of 700 g. Renal pelvis was most resistant to perforation and damage beyond the MP, and although no significant difference was found for perforation risk between bladder and ureter tissue, bladder tissue demonstrated deeper anatomical damage when force was increased from 0 g to 400 g. Most importantly, all devices and tissue types provided a reasonably margin of safety for probe-tissue contact times of 3 and 5 seconds with no more than 400 g of force—representing what would most commonly be seen in clinical practice.
Footnotes
Disclosure Statement
Manoj Monga, MD, serves as a paid consultant for Boston Scientific, Cook Urological, Bard Urological, and Gyrus ACMI. No competing financial interests exist for the remaining authors.