
Abstract
Purpose:
Over the last decade, shockwave lithotripsy (SWL) success rates have been correlated with stone density, skin-to-stone distance (SSD), and stone diameter. However, time constraints and the technical challenge of manual measurement often preclude utilization of these parameters. In this study, we describe a scoring system that accurately predicts SWL stone-free rates, is simple to calculate, and can be easily included in the radiology report.
Materials and Methods:
Two hundred thirty-five patients who underwent SWL from 2011 to 2014 were evaluated. One hundred thirty-three had available preoperative imaging. Stone density, SSD, ellipsoid stone volume (ESV), and stone-free rates were determined. Receiver operator characteristic (ROC) curves were generated to determine cutoff values for each parameter. The Triple D Score was calculated based upon the number of cutoff values a stone fell below.
Results:
One hundred forty of the 235 patients (59.5%) who underwent SWL were stone free after single-session treatment. Seventy-six of the 133 (57.1%) patients with available preoperative imaging were stone free. ESV, SSD, and stone density were significant predictors of SWL success. Based upon the ROC curves, cutoffs of <150 μL for ESV, <12 cm for SSD, and <600 HU for stone density were established. A Triple D Score of 0, 1, 2, and 3 correlated with SWL success rates of 21.4%, 41.3%, 78.7%, and 96.1%, respectively.
Conclusions:
Readily available predictive tools are necessary to enhance SWL cost-effectiveness. The Triple D Score is simple to calculate and can be reported by radiologists. Incorporation of the Triple D Score into preoperative planning may increase the overall SWL success rates.
Introduction
S
Despite this, SWL remains an attractive component of the stone treatment armamentarium. Patients often prefer SWL because of its noninvasive nature and infrequent need for a stent. In addition, for the surgeon, it is a simple procedure to perform. Thus, the impetus to improve the efficiency of SWL remains.
We sought to develop a method to improve patient selection to optimize SWL outcomes. Numerous CT-based metrics have been described as predictors of SWL outcomes. Drawing from these reports, we developed a scoring system, the Triple D Score, which incorporates three metrics—stone density, stone volume (dimensions), and skin-to-stone distance (SSD), to augment the prediction of SWL treatment outcome.
Materials and Methods
We performed a retrospective analysis of consecutive renal and ureteral stones treated with the Medispec E3000™ at our institution from April 2011 to April 2014. Following the administration of an intravenous sedative, 2500 shocks at a rate of 96 shocks per minute were delivered with ramping up of power levels from 11 to 22 kV. In patients who developed cardiac arrhythmias, the shock rate was decreased to correspond with the heart rate.
All patients with previously untreated renal or ureteral stones greater than 4 mm that had available preoperative CT imaging as well as follow-up imaging through renal ultrasound or abdominal X-ray were included in our analysis. Results were determined after a single SWL treatment was administered. Effective treatment was defined as the absence of stone on abdominal X-ray and/or renal ultrasound 4 to 6 weeks following treatment.
The Triple D Score was formulated based upon the measurement of the three significant CT-based predictors in our cohort—ellipsoid stone volume (ESV), stone density based upon HU, and SSD. These measurements were determined by a radiologist who was blinded to the results of the stone treatment.
ESV was determined calculating the ellipsoid volume of the stone [volume=π/6*(AP*H*CC)] after measuring the anteroposterior and horizontal dimensions in the axial images and the craniocaudal dimension in the coronal images. SSD was calculated as described previously by Pareek and colleagues. 4 Stone density was measured by determining the average HU of an elliptical region of interest over the largest portion of the stone that could be included.
Student's t-test was utilized to determine statistical difference between these parameters. Receiver operator characteristic (ROC) curves were generated to establish cutoff values.
The Triple D Score was calculated for each targeted stone based upon whether the measured stone volume, density, and SSD were less than the cutoff value. Stone-free rates were then determined for each Triple D Score.
Results
Two hundred thirty-five patients underwent SWL. Of these, 140/235 (59.5%) were stone free. One hundred thirty-three patients met inclusion criteria and 76/133 (57.1%) were stone free following treatment. There was no significant difference in age, gender, stone laterality, or stone location between patients who were stone free and those who were not (Table 1).
The mean ESV among patients who were stone free following SWL was 153 μL versus 332 μL for those who failed treatment (p<0.001, Table 2). For stone density, the average attenuation value was 602 HU for stone-free patients and 886 HU for patients with residual stone (p<0.001). Finally, for SSD, an average SSD of 11.3 cm was measured for those who were stone free and 12.4 cm was noted for those who were not (p<0.05).
ROC curves were generated for each of these parameters (Fig. 1). The area under the curve (AUC) for ESV, SSD, and stone density was 0.7745, 0.6274, and 0.7752, respectively. Cutoffs based upon the value corresponding to the greatest sensitivity and specificity were established to be 150 μL for ESV, 600 HU for stone density, and 12 cm for SSD.
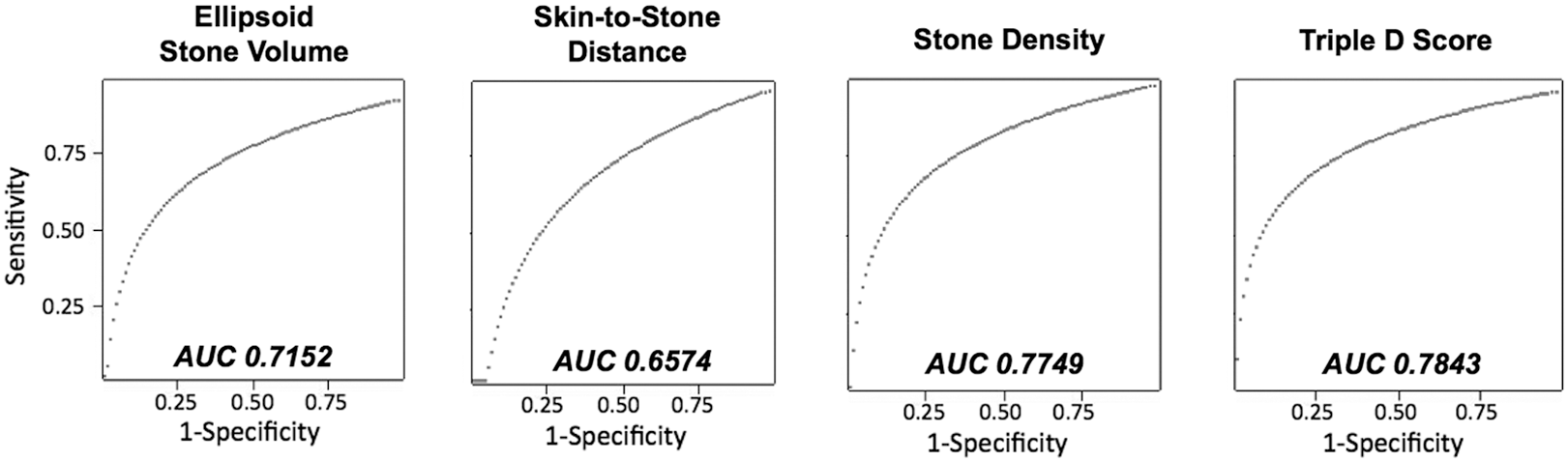
Receiver operator characteristic curves for measured CT parameters and Triple D Score.
The Triple D Score was calculated based upon the number of parameters that fell below the cutoff values. A Triple D Score of 0, 1, 2, and 3 correlated with stone-free rates of 21.4%, 41.3%, 78.7%, and 96.1%, respectively (Table 3). The AUC for the Triple D Score was 0.8338.
Discussion
Over the last decade, advancements in the technology for URS and SWL have led to improvements in the technical ease of each procedure, but have also yielded a divergence in their stone-free rates. With increasing surgeon experience and the rapid improvement of ureteroscope and fiber technology, URS stone-free rates have increased. In contrast, modernization of the shockwave lithotripter has led to a less cumbersome procedure; while, these devices have yielded a lower stone-free rate compared with their first-generation predecessors. 2
This decrease in treatment efficacy may be driven by technical limitations. Replacement of water, which facilitates minimal absorption of shockwave energy at the water–patient interface with the gel–patient interface, invariably results in air pockets that can markedly deteriorate the transmission of the shockwave. 5 In an in vitro demonstration, Pishchalnikov and colleagues reported that the presence of merely 2% air bubbles results in a 20% to 40% decrease in stone breakage. 6 In addition, while modern lithotripters have decreased anesthetic requirements for SWL, less frequent use of general anesthesia also results in increased movement during shockwave delivery. Cleveland and colleagues demonstrated that respiratory motion can lead to >20 mm of stone movement, resulting in nearly 75% of shockwaves missing the targeted stone. 7
In time, the technology of SWL will improve. Lithotripters with larger focal zones and constant stone targeting systems are being developed to improve the efficiency of shockwave delivery to the stone and limit injury to the surrounding renal parenchyma. 8,9 Tandem head lithotripters, which deliver closely timed shocks, are being investigated as a method to improve the generation of cavitation bubbles for better stone fragmentation. 10
However, at this point, an improvement in SWL efficiency will be driven by optimal use of the currently available devices. Improved identification of appropriate treatment candidates is necessary. Noncontrast computed tomography (NCCT) is commonly obtained before endourological management. 11 As such, investigators have focused on evaluating the predictive value of parameters that can be measured on NCCT. We sought to utilize the most effective of these predictors and formulate a score that integrates these parameters and provides a rapid assessment of the likelihood of SWL success. The Triple D Score was ultimately formulated based upon consideration of the SSD, stone density, and stone volume (dimensions).
SSD is a predictor of treatment success in ureteral and renal stones. 4,12,13 It is theorized that traveling a greater distance may attenuate the force of the shockwave. Prior studies have reported cutoff values between 10 and 11 cm. 4,13 In our study, there was a significant difference in mean SSD among those who were stone free (11.3 cm) and those who were not (12.4 cm). Interestingly, the cutoff SSD was 12 cm, a higher value compared with what was noted in previous studies. It is possible that as SWL has evolved, greater SSD is overcome by improved surgeon expertise, perhaps with facilitation of more accurate fluoroscopic targeting of stones in obese patients. Similarly, more experienced surgical teams may be able to establish better coupling between the lithotripter and patient, reducing air pockets that limit energy transfer. 14
Stone density has been demonstrated in a multitude of studies to have predictive value for SWL success. Two groups have reported that stones with a HU density >900 are significantly more likely to fail SWL. 13,15 Ouzaid and colleagues noted a 96% success rate for stones below 970 HU, while 62% of patients above that threshold failed treatment. 16 In our analysis, stone density was the strongest predictor of treatment success, with an AUC of 0.7752 on ROC curve analysis.
A variety of measurements have been evaluated in the assessment of stone size. These include the stone diameter, surface area, and volume. 17 –19 In a multivariate analysis, Bandi and colleagues demonstrated the stone volume to be a more accurate predictor compared with the stone diameter for SWL success. 19 They hypothesized that the determination of stone burden by stone diameter or area can lead to inaccurate assessment as this metric does not account for stone depth. One factor that limits routine implementation of stone volume is its requirement for specialized software and technicians, which is not available to most practitioners. Our metric for stone volume, ESV, was developed for the purpose of overcoming this barrier. ESV can be rapidly determined with measurement of the anteroposterior, horizontal, and craniocaudal stone diameters. Notably, when ESV is compared with the computer-generated 3D stone volume, the correlation coefficient is r=0.9893. In our study, we found ESV to be a strong predictor of SWL success, with an AUC of 0.7745.
Clinical decision-making is typically based upon the simultaneous consideration of several key variables. While identification of individual SWL predictors is important, the next step in their application is a modality for combined assessment. The Triple D Score integrates three powerful predictors of SWL success into a single score, where a score of 0, 1, 2, and 3 correlates with success rates of 21.4%, 41.3%, 78.7%, and 96.1%, respectively (Fig. 2). This streamlined integration of SWL predictors allows for rapid stratification of patient suitability for this treatment modality.
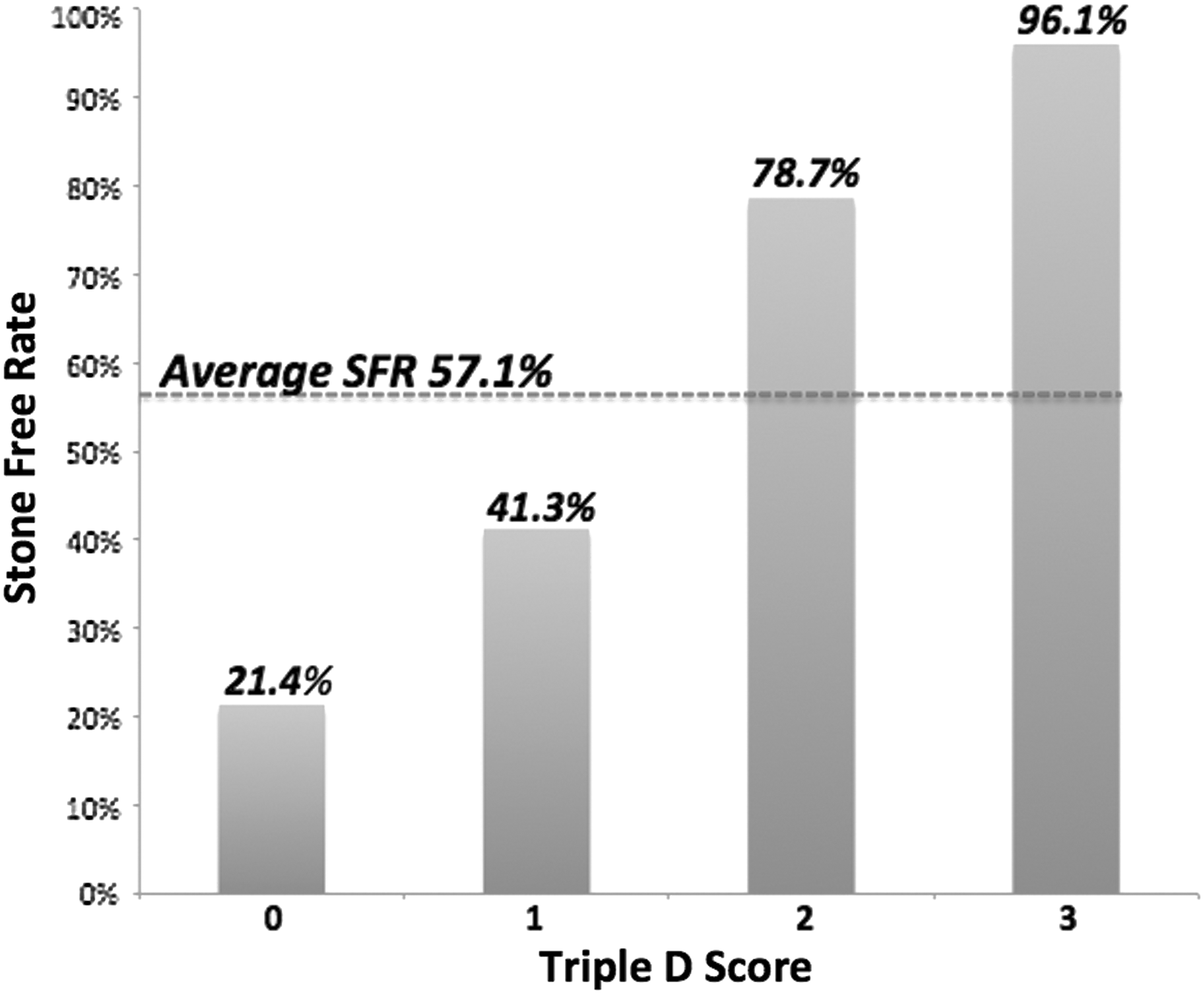
Stone-free rate based upon Triple D Score.
The utility of such scoring systems is further underscored by the shifting clinical landscape in this accountable care era. Cost effectiveness of all aspects of healthcare is under increasing scrutiny. Clinical practice patterns, ranging from diagnostic tests ordered to procedural interventions, are subject to being de-emphasized through reductions in reimbursement if they are felt to contribute to wasteful spending. In light of the noted trend of unfavorable stone-free rates of SWL in comparison to URS, improving cost effectiveness is important for maintaining the viability of this noninvasive stone treatment modality. A recent analysis by Cone and colleagues (2013, in process) compared the costs of URS and SWL. The authors noted a significantly lower cost for a single session of SWL versus URS ($3167 vs. $4470, p<0.001). However, there was a greater overall cost for SWL due to its more frequent need for auxiliary interventions. Their cost effectiveness analysis revealed that the SWL success rate of greater than 65% was required for SWL to be a cost-effective treatment modality. This analysis suggests a role for predictive systems such as the Triple D Score, where accurate preoperative assessment of treatment success can facilitate cost-effective therapy. In this case, a Triple D Score of 2 or 3, which correlates with success rates of 78% and 96%, respectively, indicates an ideal SWL candidate.
There are limitations to our study. In addition to its retrospective nature, the limited number of patients with available preoperative imaging may adversely influence the predictive accuracy of the cutoff values described. Also, as some authors have noted that residual stones may still pass after 6 weeks, 20 our postoperative follow-up period may underestimate the stone-free rates.
Conclusions
The Triple D Score appears to be a useful predictor of SWL treatment outcomes. Further evaluation of the Triple D Score with a prospective study is warranted to better assess its predictive capability. Inclusion of the Triple D Score in radiology reports will offer a readily accessible means to integrate predictive parameters from CT imaging into treatment planning. Using the Triple D Score may improve the cost effectiveness of SWL by limiting its use only to patients likely to have favorable outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.